Download presentation
Presentation is loading. Please wait.

1
Infectious Disease Division
Sexually Transmitted Infections and 2010 CDC STD Treatment Guidelines April 11, HIV/STD/TB/Hepatitis Symposium Bismarck ND David McNamara, M.D. Infectious Disease Division Gundersen Lutheran La Crosse WI

2
Disclosures No commercial disclosures
Dakota AIDS Education & Training Center

3
Learning Objective At the end of the presentation, participants should be familiar with basics of: Common Sexually Transmitted Infections 2010 CDC STD Treatment Guidelines Common presentations of HIV HIV Screening

4
What is Your Professional Discipline?
Nurse Physician Public Health (RN, Epidemiologist) Allied Health Laboratory Social Worker Other
 Allied Health. Laboratory. Social Worker. Other.")
5
Overview Sexually Transmitted Infections Case # 1 Case # 2 Case # 3
Summary

6
Sexually Transmitted Infections
Common Wide variety of pathogens can be transmitted sexually Often transmit more efficiently male→female than female→male Sequelae Direct effect of pathogen on body Infertility, ectopic pregnancy, cancer, transmission to fetus

7
Some (not all) Pathogens Transmitted Sexually
T. pallidum (Syphilis) Neisseria gonorrhoeae Chlamydia trachomatis Ureaplasma urealyticum Mycoplasma genitalium Haemophilus ducreyi (Chancroid) Chlamydia trachomatis L1, L2, L3 (Lymphogranuloma venereum) Klebsiella granulomatis (Granuloma Inguinale) Trichomonas vaginalis Scabies, Pediculosis pubis HSV, Herpes Simplex Virus HIV HBV, HDV CMV, EBV Human Papilloma Virus (HPV) HHV-8, Kaposi’s Sarcoma Herpes Virus (KSHV)
 Neisseria gonorrhoeae. Chlamydia trachomatis. Ureaplasma urealyticum. Mycoplasma genitalium. Haemophilus ducreyi (Chancroid) Chlamydia trachomatis L1, L2, L3 (Lymphogranuloma venereum) Klebsiella granulomatis (Granuloma Inguinale) Trichomonas vaginalis. Scabies, Pediculosis pubis. HSV, Herpes Simplex Virus. HIV. HBV, HDV. CMV, EBV. Human Papilloma Virus (HPV) HHV-8, Kaposi’s Sarcoma Herpes Virus (KSHV)")
9
©FMH Graphics

10
Overview Sexually Transmitted Infections Case # 1 Case # 2 Case # 3
Summary

11
Case #1 19 year-old female student presents for routine care
Sexually active with male partner Feels well, no GU symptoms Cervical swab Routine pap smear Chlamydia/Gonorrhea Nucleic Acid Amplicification Test (NAAT) Chlamydia NAAT returns positive
 Chlamydia NAAT returns positive.")
12
How should she be treated?
Ceftriaxone 250 mg IM x 1 dose Azithromycin or doxycycline for patient Azithromycin or doxycycline for both patient and her partner Cipro 500 mg PO BID x 7 days Confirm NAAT with culture prior to treatment

13
Chlamydia Chlamydia trachomatis Most common bacterial STI
Often asymptomatic Can give urethritis in men Common cause of infertility Scarring of fallopian tube (Pelvic Inflammatory Disease) 10-15% of women with untreated Chlamydia develop PID Women often re-infected if partner not treated Treat with azithromycin or doxycycline Sexually active women need yearly Chlamydia/gonorrhea testing
 10-15% of women with untreated Chlamydia develop PID. Women often re-infected if partner not treated. Treat with azithromycin or doxycycline. Sexually active women need yearly Chlamydia/gonorrhea testing.")
15
Observed Single dose treatment advantage
treatment completed No sexual intercourse for 7 days after treatment completed Test of cure not recommended 3 month re-testing recommended to screen for re-infection

16
How should her sexual partner be managed?
Timely treatment of sexual partner important to reduce risk of re-infecting index patient, others Instruct patient to refer most recent sexual partner, and any other partners within 60 days of Chlamydia diagnosis, for testing and treatment If sexual partner(s) unlikely to present for treatment, consider Expedited Partner Therapy Patient must inform partner, provide written material to seek evaluation for symptoms of complications (testicular pain, pelvic pain) Patient-delivered prescription or antibiotic for partner(s) Not for Men who have sex with Men (MSM) Very high HIV risk, partners need testing/treatment
 unlikely to present for treatment, consider Expedited Partner Therapy. Patient must inform partner, provide written material to seek evaluation for symptoms of complications (testicular pain, pelvic pain) Patient-delivered prescription or antibiotic for partner(s) Not for Men who have sex with Men (MSM) Very high HIV risk, partners need testing/treatment.")
19
Overview Sexually Transmitted Infections Case # 1 Chlamydia Case # 2
Summary

20
Case #2 28 year old man presents with painful, burning urination x 1 week Yellow urethral discharge x 3 days “I’ve never had this before!” Reports 3 female sexual partners in last several months Intermittent condom use, only when partner is new

21
Public Health Image Library
Urethral swab taken Gram stain Gram Negative Diplococci Public Health Image Library

22
Likely etiology of urethritis?
Chlamydia Herpes Simplex Virus Gonorrhea E. coli UTI/ epididymitis Syphilis

23
How should this be treated?
Ceftriaxone 250 mg IM x 1 Ceftriaxone 250 mg IM + Azithromycin 1g PO x 1 Doxycycline 100 mg PO BID x 7 days Ciprofloxacin 500 mg PO BID x 7 days Cefixime 400 mg PO x 1

24
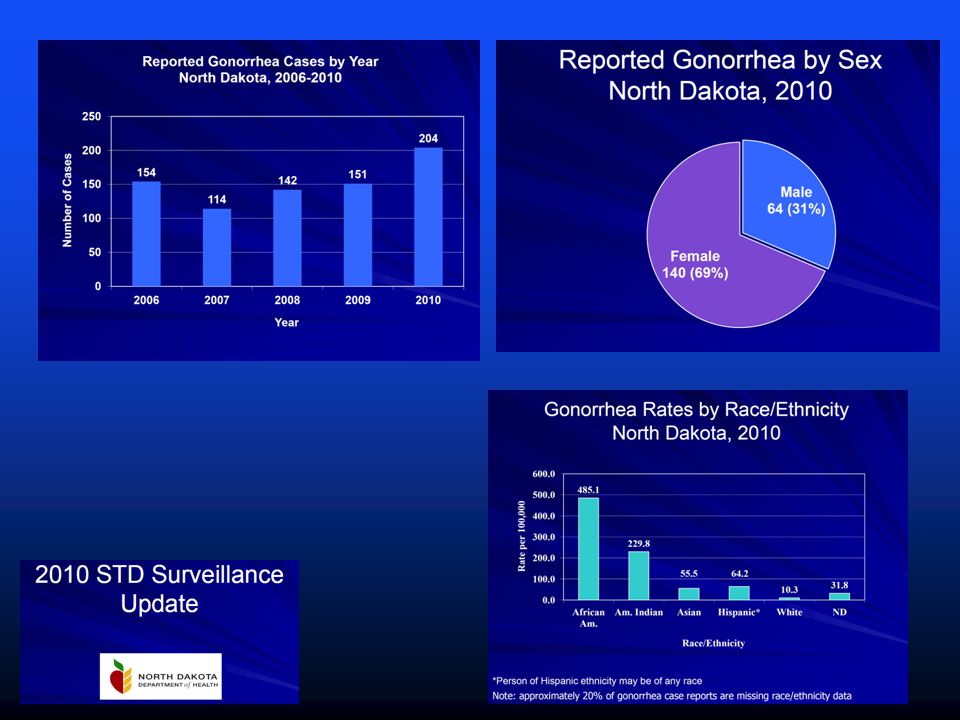
Gonorrhea Neisseria gonorrhoeae 700,000 cases/year in U.S.
Men: urethral discharge, urethritis Women: asymptomatic, dysuria, vaginal discharge, PID Diagnosis: Gram Stain Culture: Thayer-Martin media or chocolate agar NAAT on urine, urethral swab, cervical swab Will transmit to infant during birth

25
Provide treatment for Chlamydia together with Gonorrhea
Common co-infections Cipro/Levofloxacin resistent Gonorrhea now common Resistance to Cephalosporins rare but expected to increase Routine test of cure not recommended (only if symptoms) Rescreen at 3 months to detect re-infection
 Rescreen at 3 months to detect re-infection.")
28
Overview Sexually Transmitted Infections Case # 1 Chlamydia
Case # 2 Gonorrhea Case # 3 Case # 4 Case # 5 Summary

29
Case # 3 32 year old man presents with ulcer on penis
Does not hurt, present for 1 week Married, wife doesn’t have any symptoms Travels frequently for business several sexual encounters per year with other men 2 years ago Treated for gonorrhea HIV test negative at that time Uses condoms “most of the time”

30
Public Health Image Library

31
Most likely etiology of penile ulcer?
Herpes Simplex Virus Syphilis Gonorrhea Chlamydia Lymphogranuloma Venereum (LGV)
")
32
Syphilis Treponema pallidum 36,000 cases/year in U.S. 2/3 in MSM
A systemic disease Primary: painless genital ulcer (chancre) Secondary: rash Latent asymptomatic at first neurologic, bone, heart disease in years Pregnancy: transmission to infant Diagnosis: RPR or VDRL blood test All patients with Syphilis need HIV testing! All partners need evaluation, usually presumptive treatment
 Secondary: rash. Latent. asymptomatic at first. neurologic, bone, heart disease in years. Pregnancy: transmission to infant. Diagnosis: RPR or VDRL blood test. All patients with Syphilis need HIV testing! All partners need evaluation, usually presumptive treatment.")
33
Primary and secondary syphilis
Benzathine PCN G 2.4 Million Units IM x 1 dose Latent Syphilis Early: Benzathine PCN G 2.4 Million Units IM x 1 dose Late, or unknown duration: Benzathine PCN G 2.4 Million Units IM x q week x 3 doses Tertiary: cardiac, Gumma (need to rule out Neurosyphilis) Benzathine PCN G 2.4 Million Units IM x q week x 3 doses Neurosyphilis Penicillin G 24 million units/day (continuous IV infusion) x days
 Benzathine PCN G 2.4 Million Units IM x q week x 3 doses. Neurosyphilis. Penicillin G 24 million units/day (continuous IV infusion) x days.")
35
Overview Sexually Transmitted Infections Case # 1 Chlamydia
Case # 2 Gonorrhea Case # 3 Syphilis Case # 4 Case # 5 Summary

36
CC: Sore Throat 20 year-old woman presents to University Student Health Service sore throat “achy all over” for past 5 days joints ache, fevers, “I feel rotten” missed classes for 3 days “exhausted”

37
PMH: otherwise well Meds: oral contraceptives Social History grew up in rural ND sophomore business major occasional alcohol use no tobacco new boyfriend for 3 months

38
Exam VS: Temp 100.3° F Awake, alert, looks tired and ill
Oropharynx red; tonsils swollen Small, swollen mobile cervical lymph nodes Lungs: clear Cor: RRR with normal s1s2 no murmurs Abdomen soft, nontender, no HSM Joints: no effusions or synovitis Skin: rash on chest, back

41
Labs WBC N45 L5 M28 B9 E4 Hb 12.8 g/dL platelets 112,000 Group A Strep PCR: negative Assessment? Febrile illness with pharyngitis, leukopenia and rash Differential diagnosis?

42
Likely Diagnosis? Mononucleosis Epstein-Barr Virus Infection
Streptococcal Pharyngitis Acute HIV infection Severe Cold

43
Further testing? Monospot: negative CMV Antibody IgG positive, IgM negative Testing for HIV infection? HIV Antibody Screen: negative HIV Viral Load: 770,000 copies/mL

44
Diagnosis: Acute HIV Infection
Illness associated with initial HIV infection Fever, body aches, sore throat, swollen lymph nodes common Rash in 50% Uncommonly recognized Important to make diagnosis: reduce HIV transmission to others sexual partners, infants treat HIV before advanced AIDS develops

45
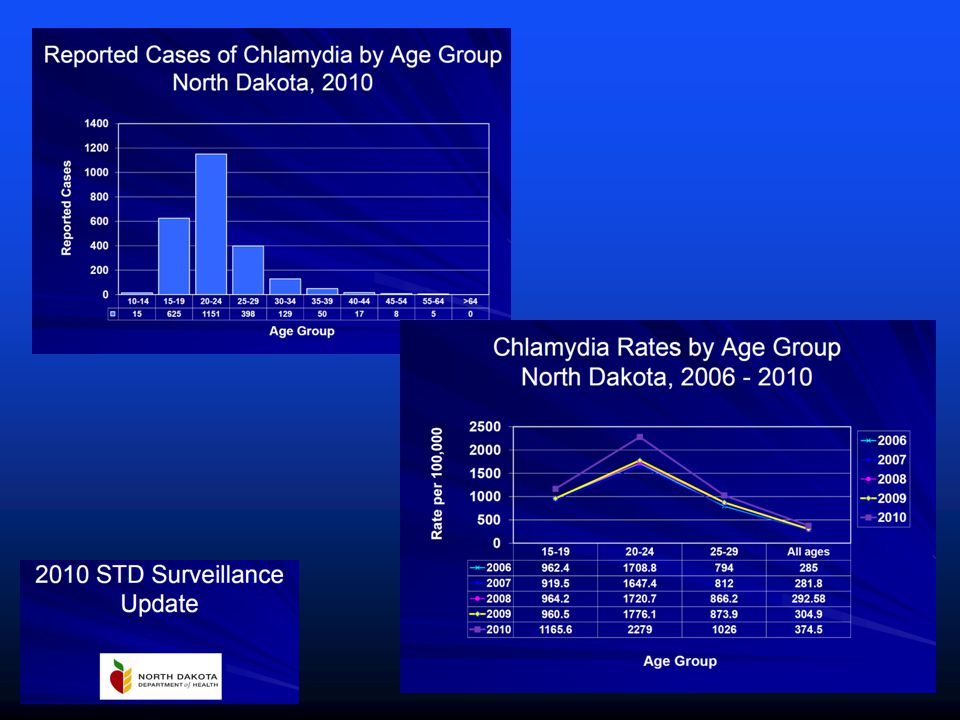
Is there HIV in North Dakota?
ND a low incidence state, but…

47
The data have been adjusted for reporting delays.
In the United States and dependent areas, the prevalence rate of AIDS among adults and adolescents was estimated at per 100,000 at the end of The rate for adults and adolescents living with AIDS ranged from an estimated 2.2 per 100,000 in American Samoa to an estimated per 100,000 in the District of Columbia. The District of Columbia is a metropolitan area. Use caution when comparing its AIDS rate to state AIDS rates. Note: The data have been adjusted for reporting delays. 47

48
The proportional distribution of AIDS cases by transmission category has shifted since the beginning of the epidemic. In 1985, male-to-male sexual contact accounted for 64% of all AIDS cases; in 2006, this transmission category accounted for 43% of all AIDS cases. The proportion of AIDS cases attributed to injection drug use increased during 1985–1994 and then slightly decreased, accounting for 19% of cases in 2006. The proportion of AIDS cases attributed to male-to-male sexual contact and injection drug use decreased from 9% in 1985 to 5% in 2006. The proportion of AIDS cases attributed to high-risk heterosexual contact increased from 3% in 1985 to 32% in 2006. The remaining AIDS cases were those attributed to hemophilia or the receipt of blood or blood products and those in persons without an identified risk factor. The data have been adjusted for reporting delays and cases without risk factor information were proportionally redistributed.

49
Of AIDS diagnoses in 2009 among adult and adolescent males, 66% of infections were attributed to male-to-male sexual contact and 15% were attributed to heterosexual contact. Approximately 12% of infections were attributed to injection drug use and 6% were attributed to male-to-male sexual contact and injection drug use. Most (76%) of the AIDS diagnoses in 2009 among adult and adolescent females had infections attributed to heterosexual contact, and 22% attributed to injection drug use. All displayed data have been estimated. Estimated numbers resulted from statistical adjustment that accounted for reporting delays and missing risk-factor information, but not for incomplete reporting. Heterosexual contact is with a person known to have, or to be at high risk for, HIV infection. 49
 of the AIDS diagnoses in 2009 among adult and adolescent females had infections attributed to heterosexual contact, and 22% attributed to injection drug use. All displayed data have been estimated. Estimated numbers resulted from statistical adjustment that accounted for reporting delays and missing risk-factor information, but not for incomplete reporting. Heterosexual contact is with a person known to have, or to be at high risk for, HIV infection. 49.")
51
North Dakota Since 1984 ~ 10 new cases/year Total 505 227 live in ND
316 AIDS 189 HIV (non AIDS) 227 live in ND
 227 live in ND.")
52
North Dakota

53
Human Immunodeficiency Virus
Infects CD4+ T-lymphocytes immune system control of infection and cancer Initial infection often has a febrile, viral syndrome Retrovirus integrates into host cell DNA, chronic infection Usually asymptomatic afterwards Gradual, progressive failure of T-cell arm of immune system Death often in 8-12 years if undiagnosed/ untreated

56
CDC 2006 HIV Testing Guidelines
Major departure from prior guidelines Test all persons years old at least once, regardless of risk factors Make HIV testing routine, similar to cholesterol or blood pressure screening “Opt-out” testing: Inform patient of HIV testing Verbal assent ok; written consent not required Patient can “opt out” if desired

57
HIV Testing Healthcare provider orders “HIV 1/2 Antibody” blood test
Lab runs a 2 part test: Initial screen: HIV Antibody ELISA very sensitive, not as specific some false positives occur if ELISA positive, lab runs HIV Antibody Western Blot test very specific

58
Prenatal HIV Testing All pregnant women need an HIV blood test Reason?
Prevent mother-to-child transmission (MTCT) of HIV Untreated HIV+ mother: 20-30% risk of transmission of HIV to infant Treated HIV+ mother: <2-5% MTCT
 of HIV. Untreated HIV+ mother: 20-30% risk of transmission of HIV to infant. Treated HIV+ mother: <2-5% MTCT.")
59
Case #4 Lessons Learned Heterosexual contact most common route of HIV infection in women HIV Antibody test will not detect HIV infection until 3-5 weeks after infection Consider Acute Retroviral Syndrome in differential diagnosis of acute febrile illness, especially if rash, sore throat, leukopenia or thrombocytopenia Lab testing: HIV Antibody (takes 3-5 weeks for + Ab) HIV Viral Load (HIV RNA PCR)
 HIV Viral Load (HIV RNA PCR)")
60
Overview Sexually Transmitted Infections Case # 1 Chlamydia
Case # 2 Gonorrhea Case # 3 Syphilis Case # 4 HIV Summary

61
Why does this matter in ND?

64
HIV, STIs have been less common here than in many parts of the country
Potential for missed, delayed diagnoses North Dakota developing rapidly More connected than we used to be Incidence of HIV, STIs likely to rise Timely recognition of HIV increasingly important

65
Summary Recognize, treat common STIs
Recognize signs of HIV infection and make diagnosis Screen for HIV infection in order to: Avoid transmission to others Prevent advanced AIDS Prevent transmission to infants

66
Acknowledgements Anne Grande, Education Coordinator Dakota AIDS Education & Training Center Christopher Wegner, HIV Prevention Capacity Building Coordinator, American Red Cross Further resources: cdc.gov North Dakota Department of Health,

Similar presentations