Download presentation
Presentation is loading. Please wait.

2
Terminology in Chest XRays PA view- chest close to xray plate xray tube 6 feet from patient Pt erect AP view- back close to plate xray tube 3 feet from pt pt supine PA – sharper less magnified Both generally taken in full inspiration Oblique- taken with pt standing obliquely. Right oblique is with right chest against the plate Lateral decubitus – side of supine pt on the plate with xray tube horizontal Apical Lordotic- xray tube angled at 45’ Sternal & rib views

3
HOW TO READ A CHEST X-RAY Switch off all unnecessary lights. 1.Identify patient name,age,sex,hosp #. Date of xray and side marker (R or L) 2.. Check the adequacy and tech quality of film Exposure- mid thoracic intervertebral disc should be clearly visible or a finger held behind the black part of the film should be just visible. Underexposed film is pale- lung appears consolidated/pulm edema. Overexposed film is black – suggest emphysema Position – Supine or erect. PA,APor lat Rotation (centered)- Spinous process of upper thoracic vertebrae should be central & Medial ends of clavicles must be equidistant from the central spinous process Lung volume (Degree of inspiration)- Right hemidiaphragm should reach the anterior end of 6 th / 7 th rib or the 9 th / 10 th rib posteriorly on full inspiration > 6 th rib in expiration indicates hyperinflation( emphysema) < 5 th rib indicates underinflation ( crying infant) Film taken in expiration may simulate disease – cardiomegaly, pulmonary congestion 1
 2.. Check the adequacy and tech quality of film Exposure- mid thoracic intervertebral disc should be clearly visible or a finger held behind the black part of the film should be just visible. Underexposed film is pale- lung appears consolidated/pulm edema. Overexposed film is black – suggest emphysema Position – Supine or erect. PA,APor lat Rotation (centered)- Spinous process of upper thoracic vertebrae should be central & Medial ends of clavicles must be equidistant from the central spinous process Lung volume (Degree of inspiration)- Right hemidiaphragm should reach the anterior end of 6 th / 7 th rib or the 9 th / 10 th rib posteriorly on full inspiration > 6 th rib in expiration indicates hyperinflation( emphysema) < 5 th rib indicates underinflation ( crying infant) Film taken in expiration may simulate disease – cardiomegaly, pulmonary congestion 1.")
4
(CONTD.) 3. Check the extrathoracic soft tissue- Start at the top with the supraclavicular areas, neck, shoulder,- look for subcutaneous emphysema., calcified glands Continue down each side of the chest Assess breast shadows. Finally check under the diaphragm for air 4.. Check the bony cage Ribs,clavicles, scapulae,shoulder jts,thoracic spine 5..Check for medical equipment like ET tube, CVP line -Tip of ET tube should be about 2 cm from carina 6. F. Check the superior mediastinum for widening or abnormal masses and identify the trachea thymus causes widening upto 2yrs 7. Check the heart- its positioned with 1/3 of its diameter to the right and 2/3 to the left of the spinous process. A low diaphragm will cause a right shift and a high d a left shift. The heart’s full dia should be less than ½ of the internal thoracic dia at its widest point ( cardiothoracic ratio) 8.Check the diaphragms, Cp & Cp angles. R dia 3 cm higher than left. Outline should be smooth with highest point medial to the midline of the hemithorax Gastric bubble seen under L diaphragm 9.. Hilum Hilar shadows- made up of pulm art and large veins. Left hilum normally 2 cm higher than right 10.Lungs Lung pattern- all the markings in a normal lung are vascular. They disappear 2 cm or less from the lung margin Lung zones- Upper – apex to 2 nd costal cartilage, Middle -2-4 cartilage lower – below 4 th cartilage
 8.Check the diaphragms, Cp & Cp angles. R dia 3 cm higher than left. Outline should be smooth with highest point medial to the midline of the hemithorax Gastric bubble seen under L diaphragm 9.. Hilum Hilar shadows- made up of pulm art and large veins. Left hilum normally 2 cm higher than right 10.Lungs Lung pattern- all the markings in a normal lung are vascular. They disappear 2 cm or less from the lung margin Lung zones- Upper – apex to 2 nd costal cartilage, Middle -2-4 cartilage lower – below 4 th cartilage.")
5
Features of Anatomy seen on PA VIEW

6
LATERAL VIEW

7
Normal PA view

8
PA VIEW Each lobe is covered by visceral pleura.The visceral pleura bordering adjacent surfaces of 2 lobes form the septa,which separates the lobes. The space between 2 adjacent septae is called the interlobar fissure- a fissure is a narrow space; a septa is a divider. The 2 terms are used interchangeably Right lung has 3 lobe-RUL,RML,RLL separated by septa or fissures R major fissure runs obliquely downwards from 5 th thoracic vertebra to the diapraghm to a point just behind the ant cp angle. Not normally seen in PA view as it is not parallel to the x-ray beam The Right minor fissure intersects the lateral chest wall at the level of anterior portion of 4 th rib(+/_2) RUL made up of apical,anterior & posterior bronchopulmonary segments RML made up of lateral and medial segments RLL made of superior, medial basal, ant basal, lateral basal and post basal
 RUL made up of apical,anterior & posterior bronchopulmonary segments RML made up of lateral and medial segments RLL made of superior, medial basal, ant basal, lateral basal and post basal.")
9
PA view Left lung is made of LUL & LLL The LUL is made up of apicoposterior and anterior segments The lower or lingular division of the LUL is made up of sup & inf seg The LLL is made up of the sup, medial basal, ant basal, lat basal and postbasal

10
NORMAL CXR Trachea is central Dome of R diapraghm is at the level of 6 th rib L hemidiapraghm is 3cm lower than the R Heart size is < 50% of the thoracic diameter. 2/3 of the heart lies to the L and 1/3 to the R of the spine Cardiac apex & gastric bubble are to the left Horizontal fissure lies at the level of the 4 th costal cartilage. Mediastinum is < 25% of the chest width

11
HEART BORDERS 1.Aortic knuckle 2.Pulm. Artery 3.L.atrial appendage 4.L ventricle 5.R atrium 6.trachea 7.R dome of diaphragm 8.gas bubble in stomach 9.horizontal fissure

12
CT ratio MRD:maximum R diameter MLD :maximum L diameter. ID : internal diameter

13
USEFUL RULES & SIGNS The Silhouette Sign Contiguous objects of the same density are not seen separately The 4 basic densities are air, fat, water and metal The silhouette sign is seen when a border of the heart, aorta, or diaphragm is obliterated The heart and ascending aorta are anterior structure

14
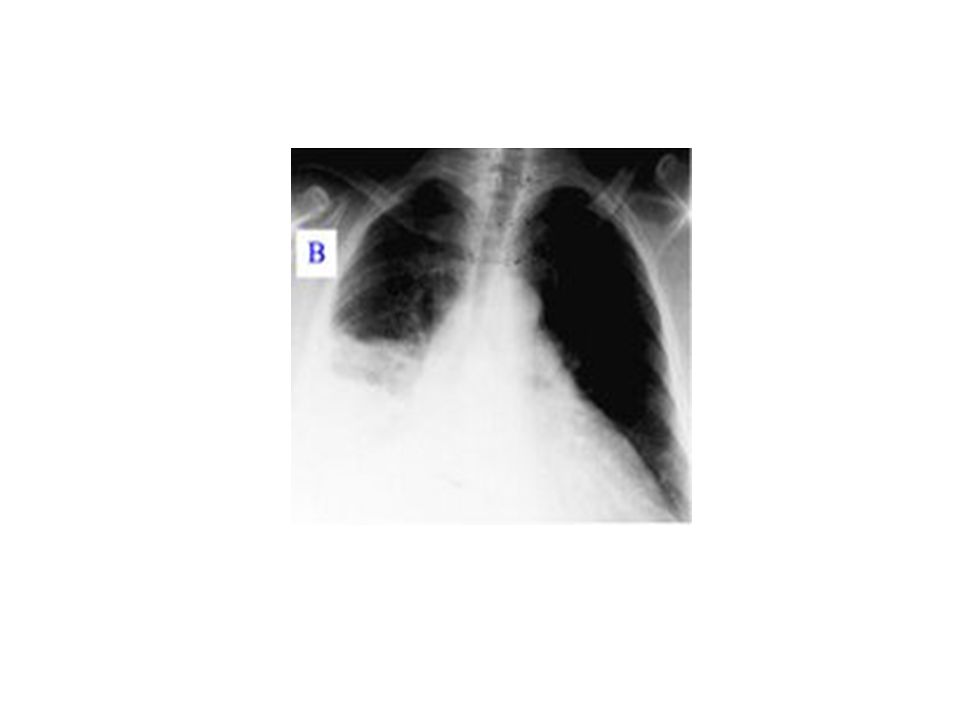
Causes of confluent opacification of a hemithorax There are four main causes of confluent opacification of a hemithorax - consolidation (that is, material within the air-spaces and pleural effusion - that is, material within the pleural space, which could be serous fluid, blood, or pus. Complete collapse of one lung with the mediastinum shifting over the the abnormal side can also cause a "white out" on the abnormal side. Finally, after a pneumonectomy the mediastinum shifts to the empty hemithorax and the residual pleural space fills with fluid and fibrotic material leaving the patient with a complete "white out" on the side that has been operated on. Consolidation and pleural effusion are the two most common, and it can be difficult to distinguish between them - of course, they can coexist.

15
Collapse-RML Silhouette sign

16
RML COLLAPSE-LATERAL

17
RML collapse..graphic

18
Collapse Collapse of a lobe is caused by proximal obstruction – for example, by a neoplasm, mucus plug, such as in a postoperative patient, or foreign body, such as in a child.

19
AIR BRONCHOGRAM The bronchi are not normally seen on the xray as they are thin walled, contain air and are surrounded by air in the alveoli Visualisation of air in the bronchi is known as an air bronchogram Air- filled bronchi can be seen if surrounded by diseased lung which contains no air (eg pneumonia, hyaline membrane disease,RDS)
")
20
RDS

21
SAIL SIGN The normal thymus lies in the sup, ant mediastinum. In the infant, it may appear to widen the mediastinum in a PA view, being largest at about 2 years of age The inferior border of the R thymic lobe is a straight line. When it rests on the R horizontal fissure it produces an appearance referred to as the “sail sign”

22
“sail sign”

23
RUL collapse..graphic

24
Findings in COLLAPSE/ATELECTASIS Increased Radiopacity Shift of fissure, hilum, mediastinum Crowding of vessels & airways within the lobe Crowding of ribs Compensatory emphysema Elevation of the hemi diaphragm ( tenting )
")
25
LLL COLLAPSE

27
PNEUMONIA- RUL CONSOLIDATION Not very dense opacity Loss of contingous borders No volume loss Air bronchogram Loss of vascular markings

28
Medial segment of R middle lobe CONSOLIDATION

30
RM&LL PNEUMONIA

31
TB HILAR ADENOPATHY

32
APICAL TB

33
MILIARY TB

34
Pl. effusion R

Similar presentations







 –Partial.>")














