Download presentation
Presentation is loading. Please wait.

1
NeurosurgeryNeurosurgery

2
Outline A & P Pathology Diagnostics/Pre-operative Testing Medications/Anesthesia Positioning/Prepping/Draping Supplies/Instrumentation/Equipment Dressings/Drains/Post-op Care Procedures: Carpal Tunnel Release, Craniotomy, Cervical Discectomy, Lumbar Discectomy, Ventroperitoneal Shunt

3
Nervous System Functions: Senses changes in environment Interprets changes Stimulates movement to respond to these changes

4
Organization of the Nervous System Two systems: 1. CNS Central Nervous System Two major parts: Brain and Spinal Cord 2. PNS Peripheral Nervous System Everything else

5
Peripheral Nervous System Two major parts: Afferent Nervous System Sensory neurons take info from PNS to CNS Efferent Nervous System Motor neurons take info from CNS to PNS

6
Efferent Nervous System Motor nervous system 2 parts: 1.Somatic Nervous System Skeletal muscle control Conscious control 2.Autonomic Nervous System Cardiac muscle, smooth muscle, and glands Unconscious control Has 2 divisions: Sympathetic Division Parasympathetic Division

7
Autonomic Nervous System Sympathetic vs. Parasympathetic Controlled by hypothalamus and medulla oblongata Both are different nerves going to the same effector or target Are antagonistic Parasympathetic = decreased skeletal blood flow, increased organ blood flow (quietly eating) Sympathetic = increased skeletal blood flow, decreased organ blood flow (eatus interruptus by a bear!) Also called fight or flight; prepares body for emergencies
 Sympathetic = increased skeletal blood flow, decreased organ blood flow (eatus interruptus by a bear!) Also called fight or flight; prepares body for emergencies.")
8
Spinal Cord Functions: Info to and from the brain Integration of reflexes Location: Begins at foramen magnum and extends to 2 nd lumbar About 16-18” in length

9
Spinal Cord Support Structures Vertebra 33 total 7 cervical 12 thoracic 5 lumbar Sacrum formed by 5 fused bones Coccyx formed by 4 fused bones

11
Intervertebral Disks Separate vertebrae Outer layer is tough and called the annulus fibrosis Inner core is soft and called the nucleus pulposus Bear stress incurred with body weight and when lifting

12
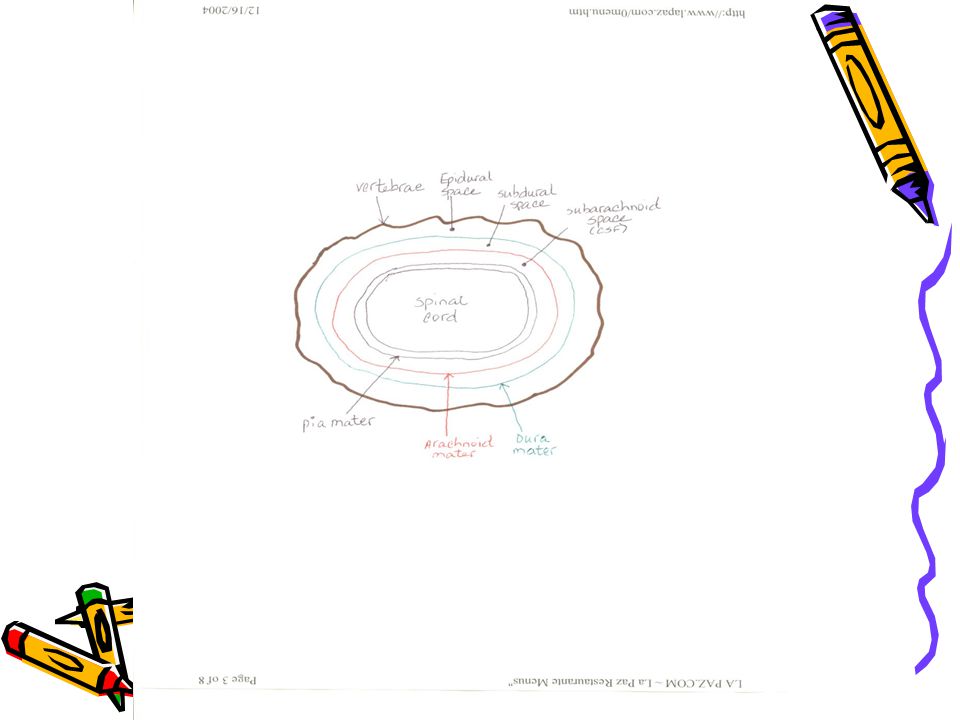
Spinal Cord Support Structures Meninges Between vertebra & spinal cord Epidural space between vertebra and dura mater 1.Dura Mater outermost layer extends to S-2 Subdural space between dura mater and arachnoid 2.Arachnoid extends to S-2 Subarachnoid space contains CSF 3.Pia Mater adheres directly to spinal cord and extends to L-2 Meninges also cover brain/continuous layer/difference epidural space not present

14
Spinal Nerves 31 pair Names and numbers depend on where enter and exit Each has a ventral and dorsal root Ventral root = motor Dorsal root = sensory 8 cervical 12 thoracic 5 lumbar 5 sacral 1 coccygeal

16
Brain Protected by the cranium or skull

18
Brain 4 major parts: Brain stem Diencephalon Cerebellum Cerebrum Weight about 3 lbs.

20
Support Structures of the Brain 1. Meninges Continuous layer with spinal cord NO epidural space

21
Support Structures of the Brain 2. Cerebrospinal fluid (CSF) About 800ml produced each day by the choroid plexus, a specialized set of capillaries Circulates inside subarachnoid space through central canal of spinal cord and the ventricles of the brain Reabsorbed in arachnoid villus found in the parietal lobe Functions as a shock absorber and circulates nutrients
 About 800ml produced each day by the choroid plexus, a specialized set of capillaries Circulates inside subarachnoid space through central canal of spinal cord and the ventricles of the brain Reabsorbed in arachnoid villus found in the parietal lobe Functions as a shock absorber and circulates nutrients.")
22
Support Structures of the Brain 3.Blood Brain Barrier Specialized set of capillaries exclusive to the central nervous system Less permeable than any other capillaries in the body Advantage = keeps out unwanted chemicals Disadvantage = difficult to diffuse materials out, hence difficulty in treating conditions such as encephalitis

23
Brain Stem 3 parts: Medulla oblongata Pons Midbrain

24
Medulla oblongata Contains: 5 of 12 cranial nerves Pyramids: function only with motor neurons/a crossing of the spinal nerve impulses Reflex centers: hiccupping, sneezing, coughing Vital reflex centers: Cardiac center – heart rate Vasoconstrictor center-BP via blood vessel diameter control Respiratory center - breathing

25
Pons Above medulla Switching point for motor neurons Respiratory center

26
Midbrain or Mesencephalon Above pons Involuntary eye and head movement in response to auditory stimuli

27
Diencephalon 2 parts: Thalmus Hypothalmus

28
Thalmus Relay center for sensory information Interprets stimuli for example pain from changes in temperature (hot stove) 1 st level of reasoning occurs here Recognizes crude touch NOT localized touch
 1 st level of reasoning occurs here Recognizes crude touch NOT localized touch")
29
Hypothalmus Controls large number of subconscious functions Controls most of Autonomic nervous system Where endocrine and nervous systems interface Homeostasis regulation of the body Controls: body temp, thirst, hunger, sleep and waking habits, psychosomatic disorders, rage and aggression

30
Cerebellum 2 nd largest part of the brain Primarily a motor area Controls skeletal muscles, subconsciously Receives sensory input from eyes, muscles, joints, and inner ear Posture, balance, coordination, equilibrium Muscle sense tells body where other parts are

31
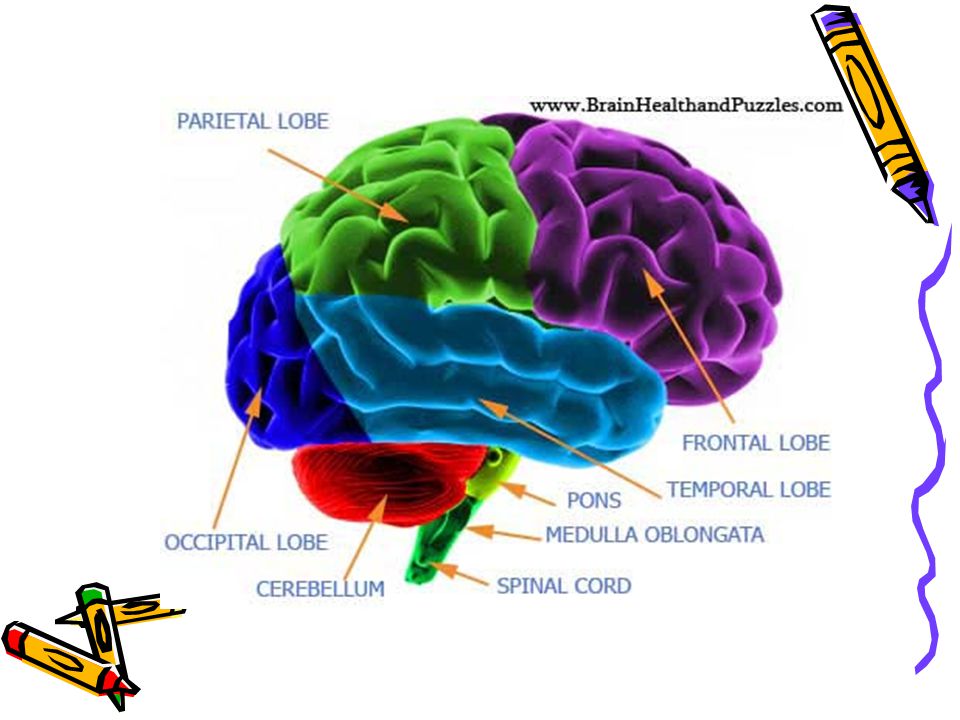
Cerebrum Largest part of brain Motor/sensory/association area 4 Lobes: frontal, parietal, occipital, temporal Each controls a specific function be it motor or sensory Limbic system: controls emotion/functions in cerebral cortex and diencephalon See page 970 Figure 24-4 in Price

32
Cerebrum Lobes’ Function Frontal Memory, abstract thinking, ethics, judgement, emotion, expressive speech, motor Parietal Sensory, receptive speech, written word Temporal Auditory, olfactory Occipital Visual cortex Visual association

33
Cranial Nerves All originate in the brain stem EXCEPT the 1 st and 2 nd Classified as sensory or mixed (sensory and motor) nerves Directly off of brain Do not go through the spine Identified by Roman numerals and names
 nerves Directly off of brain Do not go through the spine Identified by Roman numerals and names")
34
Cranial Nerves I.Olfactory - sense of smell II.Optic – sense of sight/vision III.Occulomotor – eyeball, eyelid movement (medial, inferior, superior rectus, inferior oblique), pupil constriction, lens accommodation Muscle sense for eyeball IV.Trochlear – eyeball movement (superior oblique) Muscle sense for eyeball V.Trigeminal – masseter muscle control Sensory part has 3 branches: ophthalmic (forehead to corner of eye), maxillary (corner of eye to upper lip/teeth), and mandibular (lower lip/teeth/tongue) All three convey sense of touch, pain and temp changes VI.Abducens - same as IV eyeball movement (lateral rectus) and eyeball muscle sense FYI: EOM formula LR6(SO4)3
, pupil constriction, lens accommodation Muscle sense for eyeball IV.Trochlear – eyeball movement (superior oblique) Muscle sense for eyeball V.Trigeminal – masseter muscle control Sensory part has 3 branches: ophthalmic (forehead to corner of eye), maxillary (corner of eye to upper lip/teeth), and mandibular (lower lip/teeth/tongue) All three convey sense of touch, pain and temp changes VI.Abducens - same as IV eyeball movement (lateral rectus) and eyeball muscle sense FYI: EOM formula LR6(SO4)3")
35
Cranial Nerves VII.Facial- facial muscles, lacrimal and salivary glands anterior 2/3 of tongue (taste) VIII.Vestibulocochlear -last of totally sensory nerves; has 2 branches: vestibular conveys balance and cochlear which conveys sense of hearing IX.Glossopharyngeal -salivary gland secretion and posterior 1/3 of tongue X.Vagus – internal organ control motor and sensory; originates in medulla and goes down through neck into chest and abdomen XI.Accessory – controls head and neck movement, speech, and muscle sense for the head XII.Hypoglossal – tongue muscles: swallowing, speech, muscle sense for tongue
 VIII.Vestibulocochlear -last of totally sensory nerves; has 2 branches: vestibular conveys balance and cochlear which conveys sense of hearing IX.Glossopharyngeal -salivary gland secretion and posterior 1/3 of tongue X.Vagus – internal organ control motor and sensory; originates in medulla and goes down through neck into chest and abdomen XI.Accessory – controls head and neck movement, speech, and muscle sense for the head XII.Hypoglossal – tongue muscles: swallowing, speech, muscle sense for tongue")
36
Neuro Pathology

37
Cervical Spine Pathology Very serious Can have severe consequences related to all of the spinal cords’ nerve pathways Spondylosis is osteophyte or bone spur formation in the spinal canal Cervical disk extrusion acute or chronic Treatment errs on the side of caution due to potential extreme consequences of surgical intervention

38
Thoracic Pathology Spondylosis Extrusion of disk

39
Lumbar Pathology Spondylosis Stenosis Spondylolithesis Disk extrusion

41
Neoplasms/Tumors Two types: Primary Originate in nervous tissue or meninges Secondary Are metastasized from other parts of the body May be classified as benign or malignant

42
Tumors Benign tumors: “Craniopharyngiomas, epidermoids, hemangiomas, menigiomas, acoustic neuromas, and pituitary microadenomas” Price, 2004 Malignant tumors: “Astrocytes or gliomas” Price, 2004 Benign usually excisable via craniotomy Malignant normally cannot be completely removed but efforts are made to remove most

43
Head Trauma Includes; Scalp lacerations, fractures, hematomas (epidural or subdural), and brain injuries
, and brain injuries")
45
Spinal Cord Trauma Vertebral Fracture Vertebral Dislocation Herniated disk into spinal canal Laceration from GSW or MVA

46
Cerebrovascular Disease #3 cause of death in US Symptoms reflect ischemia (TIAs) or hemorrhage Intracranial aneurysm Arteriovenous malformations Brain hemorrhage Stroke or cerebrovascular accident (CVA)
 or hemorrhage Intracranial aneurysm Arteriovenous malformations Brain hemorrhage Stroke or cerebrovascular accident (CVA)")
47
Congenital Pathology Craniosynotosis “premature closure of the cranial sutures” Price, 2004 Hydrocephalus result of obstructed CSF flow Spina bifida

48
Infection Abscess Subdural empyema Post-op infection

49
Spinal Cord Tumors Intramedullary in the spinal cord Intradural in dura, outside spinal cord Extradural outside spinal cord Price, 2004

50
Peripheral Nerve Pathology Carpal tunnel syndrome - compression of the median nerve Ulnar nerve compression – compression of ulnar nerve by the ligament of Osborne Price, 2004

51
Diagnosis History and physical Symptoms usually specific to area of pathology Electroencephalogram (EEG) X-ray Myelogram CAT Scan MRI Cerebral arteriograms
 X-ray Myelogram CAT Scan MRI Cerebral arteriograms")
52
Medications Lidocaine 1% with epinephrine Topical hemostatic agents: gelfoam, avitene, surgicel, bone wax Antibiotic irrigants Topical papaverine for prevention of spasm during intracranial artery surgery Methyl methacrylate with cranioplasty Heparin saline irrigation again with intracranial artery surgery Contrast solutions with cerebral arteriography Gliadel wafers (tumor bed of glioblastoma)
")
53
Anesthesia General Could be local with MAC for minor laceration suturing

54
Positioning Cranial Surgery Supine primarily, with a specialty headrest and or fixation devices Can be lateral or semi- lateral Sitting Prone Varies with location of access Spinal surgery Anterior procedures require supine Posterior procedures require prone

55
Preps Will require shave especially on head Varies with surgeon preference: betadine, alcohol, chlorohexidine Care taken NOT to get in patient’s eyes or facial orifices

56
Draping Toweled out Adhesive type drape Specialty drapes: laparotomy, thyroid, craniotomy, lumbar Stockinette for peripheral procedures

57
Supplies Marking pen Disposable bi-polar cord Monopolar pencil/bovie Cottonoids/patties Raney clips Hemostatic clips Shunt catheters, tubing, connectors Cotton balls Hemovac drain Nerve stimulator Telfa Microscope drape C-Arm drape Ultrasound wand drape

58
Instruments Minor tray if laminectomy and craniotomy trays do not have basic instrumentation Laminectomy tray Craniotomy tray Basic ortho tray Plates and screws Specialty self-retaining retractor trays: Greenburg

59
Miscellaneous Instrumentation See pages 987-990 in PRice

60
Equipment microscope Video tower YAG or CO 2 laser Positioning equipment: Mayfield headrest, Gardner-Wells Operative Ultrasound machine Stereotaxis system CUSA Cavitron ultrasonic aspirator Bipolar and monopolar ECU Nitrogen source for power equipment (saws/drills) Mayfield overbed table Headlight and light source C-Arm and monitor Cell saver Fluid warming and temperature regulating equipment
 Mayfield overbed table Headlight and light source C-Arm and monitor Cell saver Fluid warming and temperature regulating equipment")
61
Dressings/Drains/Post- op Care Dressings surgeon preference Drains surgeon preference Post-op care: keep field sterile until patient has left the OR Careful with moving patient to avoid patient injury and hemorrhage

62
Post-operative Complications Infection Hemorrhage Nerve damage CSF leakage Meningitis Neurological deficits

Similar presentations





>")




 Pia mater -inner membrane, contains.>")











 Bone – Cranium, Vertebrae 2) Meninges – Three connective tissue membranes covering the brain and spinal cord a) Dura Mater – outermost,>")
 Brain and spinal cord Peripheral Nervous System (PNS) ◦ nerves.>")
