Download presentation
Presentation is loading. Please wait.

1
Growth & Development in Adolescence KN AGARWAL, President Healthcare & Research Association for Adolescents E mail : adolcare@hotmail.com

2
Growth & Development in Adolescence 1.Succession of events in development of secondary sexual characteristics during puberty is consistent. 2.There is individual variation in the age of onset, duration and tempo of Growth.

3
Ethnic & Sibling variability in the onset and duration of Puberty 1.Ethnic- American Blacks enter puberty earlier than Whites: Breast Stage-2 at 8 years of age Blacks 48%(average age 8.8yr; PH- 8.7yr); Whites-only 15%(Av age 9.9yr; PH 10.7 yr). However, “Menarche” same time 12.2yr and 12.8yr, respectively. 2.Besides racial “Onset of Puberty” is different in an individual child, as well as in case of siblings (Ann Hum Biol 2005; et al Das Gupta)
.")
4
Puberty encompasses- - Somatic Growth & Sexual development 1.Adolescent growth spurt, 2.Development of secondary sexual characteristics. 3.Attainment of fertility. 4.Establishment of individual sexual identity. 5.Timing for Puberty onset has wide variability- 6.Girls- 8-12 years and Boys- 9-14 years of age.

5
Adolescent Growth Spurt 1.Begins distally with enlargement of Hand and Feet, followed by the Arms & Legs and finally by the Trunk and Chest. 2.Larynx, pharynx and lungs—Voice 3.Androgens- a) Sebaceous glands- Acne, b) Optic globe-myopia and c) dental- jaw growth, loss of deciduous teeth eruption of permanent cuspids, premolars, and finally molars.
 Sebaceous glands- Acne, b) Optic globe-myopia and c) dental- jaw growth, loss of deciduous teeth eruption of permanent cuspids, premolars, and finally molars..")
6
Puberty -GIRLS 1.First sign of ovarian estradiol secretion is breast development “Thelarche”.SMR-B-2 (Breast budding)- GROWTH IN HEIGHT. 2.Estradiol is a good stimulator of “GH” it doubles the growth velocity “PEAK HEIGHT VELOCITY’(9-10 cm / yr). Coincident with B-3. Follows B-2 by 1 yr. 3.Change in body shape 4.Growth under arm hair followed by secretion 5.Menarche follows PHV by 14-18 months. 6.Adult size breast
. Coincident with B-3. Follows B-2 by 1 yr. 3.Change in body shape 4.Growth under arm hair followed by secretion 5.Menarche follows PHV by months. 6.Adult size breast.")
7
Development of breast and pubic hair in girls- (Indian Data) Development of breast and pubic hair in girls- Sexual maturity Breast Pubic hair (Mean age = 13.6yr) Stages (SMR) 1. Preadolescent Pre-adolescent 2. Bud stage and papilla elevated sparse lightly pigmented straight as small mould (10.2 yr) around medial border of labia (22%) 3. Areola enlarged no contour darker, more and curly + (92%) separation(11.6 yr) 4. Areola and papilla form secondary coarse curly mound (13.6 yr) abundant (98.8%)
 around medial border of labia (22%) 3. Areola enlarged no contour darker, more and curly + (92%) separation(11.6 yr) 4. Areola and papilla form secondary coarse curly mound (13.6 yr) abundant (98.8%).")
9
Menarche & linear growth The growth in the post menarche period is limited as girls can gain 5-6 cm in linear growth, only. Thus the maximum gain in height is pre-menarche in SMR- stages –B-2 & B-3.

10
Puberty- BOYS 1.Adrenarche is the ONSET & CONTINUITY of male PUBERTY 2.Testosterone/dihydrotestosterone are needed in large concentration to initiate “GH” via the androgen receptors. (Thus later than girls by 1-2 yr). 3.Initiation testicular volume > 4 ml; maximum growth “PHV” (10-11 cm /year) attained at Testicular volume 10-12 ml. (During SMR- G 3-4). 4.Testosterone –Deepens the voice and increases body muscle mass (lean body mass).
. 3.Initiation testicular volume > 4 ml; maximum growth PHV (10-11 cm /year) attained at Testicular volume ml. (During SMR- G 3-4). 4.Testosterone –Deepens the voice and increases body muscle mass (lean body mass)..")
13
Development of genitals and pubic hair in boys- B. SMR Penis Scrotum & testes Pubic hair 1. Preadolescent Testes <4 ml none 2. Slight or no Enlarged darker scrotum scanty long (60%) enlargement(11.3 yr) pigmented Testes>4mm 3. Longer (12.8 yr) Testes 6-8 ml dark, small, curling +(97%) 4. Larger, glans + Testes 10-12 ml resemble adult type but less in breadth increased scrotum dark quantity and curls(99%) (14.1 yr) 5. Adult size Testes 12 ml spread to medial surface of thigh (16.4 yr) Facial hair 14.8 yr.
 enlargement(11.3 yr) pigmented Testes>4mm 3. Longer (12.8 yr) Testes 6-8 ml dark, small, curling +(97%) 4. Larger, glans + Testes ml resemble adult type but less in breadth increased scrotum dark quantity and curls(99%) (14.1 yr) 5. Adult size Testes 12 ml spread to medial surface of thigh (16.4 yr) Facial hair 14.8 yr..")
14
Adolescent Growth Spurt Adolescence Growth - Period extends for 2.5 to 3 years; to cross Sexual Maturity stages 2-5. Height gain is 27-29cm in boys & 24- 26cm in girls; (1 cm height will need 4500 Kcal) Weight gain in both 25-30 kg.
 Weight gain in both kg..")
15
Bone Growth- Completes in Adolescence 1.Quantitatively important bone mineral accretion occurs-increase in bone density during SMR-2 to 4(Cortical bone growth). 2.Bone mineral density- 50% completes during first month of life to puberty onset; 30% in puberty and 20% in late adolescence to adult. 3. 1 cm height gain needs Ca-20g; 30% gets absorbed (need 1300 mg/d Natl Acad. Sci. USA-97-98; AJCN 2005;-p 175). Take 4 cups of milk/d. DEFICIECY-FRACTURES
. Take 4 cups of milk/d. DEFICIECY-FRACTURES.")
16
Brain Growth in Adolescence 1.Early Childhood- Maximum Brain grows as “Frontal circuits”- related to organization and planning. 2.Adolescence- Brain grows in the rear of the brain- linked more to language learning and spatial understanding. Thus brain development continues. 3.Myelination of the prefrontal cortex continues in adolescence.

17
SEXUAL DIMORPHISM – 1.Shoulder growth in boys and hip growth in girls. 2. They start puberty with similar fat and lean body mass content. Girls finally have 27% fat and boys 18%, from 16%. In boys gain in lean body mass is twice than the girls. But girls reduce LBM from 80% to 74%.These changes are due to sex hormones 3.Maintenance cost of lean body mass needs more energy.Thus boys have increased deposition of protein and minerals e.g. Fe/Ca/Zn. Sports- need oxygen & nutrition.

18
Sexual Dimorphism in Fat Distribution

19
Growth Monitoring during Adolescence

20
Assessment stages of SMR

21
Somatic growth 1.Caineo et al 2004; Ann Hum Biol. p-182- growth measured on daily basis has Stasis, steep changes, and continous growth period with wide individual variation. 2.Cole et al 2000. BMI curves lost sensitivity in puberty. 3.Already said sexual growth varies in onset and duration- ethnic, individual & sibling..

22
Growth pattern- variations Asian children- Chinese, Japanese, Korean, Taiwanese and Indian have similar linear growth-max difference 1 cm at 17 yr age. NCHS and Europeans are taller by >7cm at 50 th and 97 th centile at 17 yr. BMI is lower in American-Indians

25
How to Measure - somatic growth in adolescence Assess sexual maturity. Ht,wt, BMI, SFT for age in relation to Sexual Maturity. BMIBMI (kg/m 2 )- “Adolescence”.- SMR related -BMI. SFT-triceps+biceps sub scapular + suprailiac in relation to SMR Waist/hip ratio >0.8 women; 0.9 men.
- Adolescence .- SMR related -BMI. SFT-triceps+biceps sub scapular + suprailiac in relation to SMR Waist/hip ratio >0.8 women; 0.9 men..")
26
REGIONAL DISTRIBUTION OF FAT Central Obesity- Excess abdominal fat(Android)-more associated with hyperglycemia, hyperlipidemia, increased triglycerides, hypertension seen more in South Indians &South Asians Peripheral fat around body(Gynoid)- is associated with less morbidity & mortality
-more associated with hyperglycemia, hyperlipidemia, increased triglycerides, hypertension seen more in South Indians &South Asians Peripheral fat around body(Gynoid)- is associated with less morbidity & mortality")
27
For comparison 1.Growth data – Somatic and Sexual growth data and the table prepared for ADOLESCENT children; Indian Pediatr 1992 & 2001(-The Growth-2003 CBS Publ. book) are the best available sets on affluent Indian children. 2. Virani 2005; Ann Hum Biol-Pondicherry 40 yr data-secular growth in 20 yr has plateaued. Indians are shorter than Europeans.
 are the best available sets on affluent Indian children. 2. Virani 2005; Ann Hum Biol-Pondicherry 40 yr data-secular growth in 20 yr has plateaued. Indians are shorter than Europeans..")
28
Agarwal’s data 1989-91. CDC 2000, did not use the NHANES III –1998- 99 data in growth curves, as obesity had significantly increased as compared to 1976-84 data. Agarwal et al data on affluent children was collected during 1989-1991. In 2002; 2000 boys were re-examined in Delhi by us; there was no secular trend for height, but obesity was observed in 10% as compared to 95th centile.

29
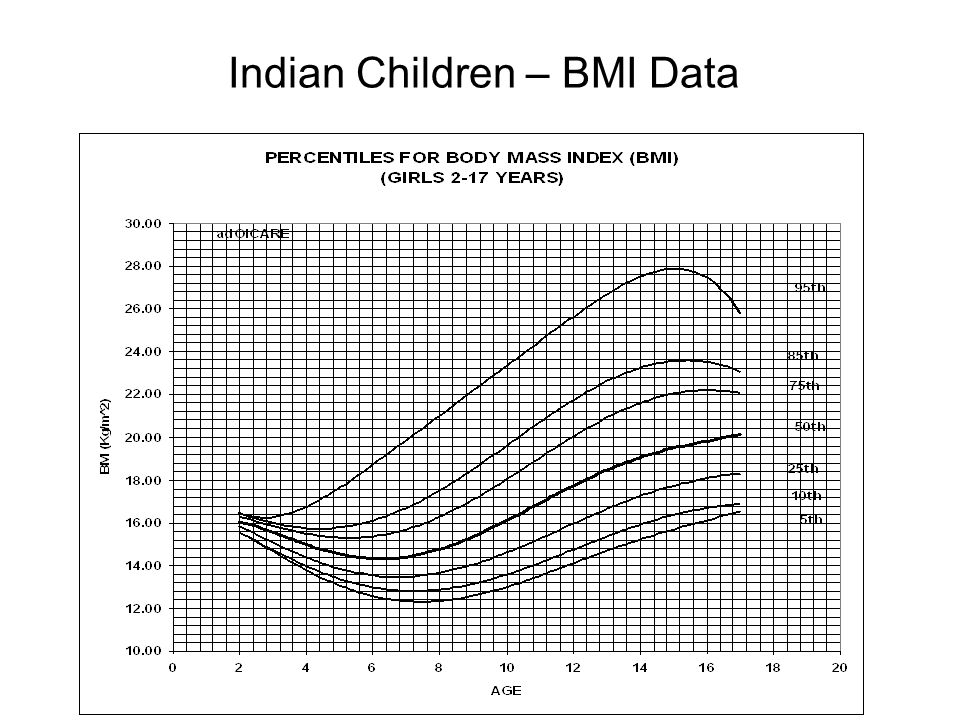
Indian Children – BMI Data

31
Indian Children Ht & Wt Data

33
. No age period could be identified for peak height velocity Height gain was similar to affluent Indian children in adolescent growth spurt. Deficit of early life in height was not corrected. Weight gain was 38% of the affluent Indian. Puberty – in Undernourished

34
Undernourished- early life to adolescent ICMR-1982-96 (Agarwals) Boys had delayed maturation of: Genitals by 1.54 yr; Pubic hair by 0.82 yr and Axillary hair by 0.65 yr. Testicular vol. was similar. Girls had delayed breast development by 2.19 yr. Menarche was delayed by 0.82 yr

35
Undernourished Adolescents until 17.5 yr of age (To achieve linear growth) Maintain their vital functions by mobilising amino-acids from body muscles as demonstrated by increased serum enzyme activities i.e. LDH, ALP, AST, ALT, CK,CK- MB and CK-mm. 31- phosphorus magnetic resonance spectroscopy showed that -ATP and Pi were significantly increased at the cost of Pcr (Phosphocreatinine). These changes simulate myopathic status (Agarwals-Acta Peditar. 1994).
. These changes simulate myopathic status (Agarwals-Acta Peditar. 1994)..")
36
Higher mental functions- undernourished adolescents There was deficit in higher mental abilities related to personal and current information, orientation, mental control, logical memory, attention span, visual reproductive and associative learning: impairment in overall memory function in set formation and conditional learning (Agarwals-Acta Paediatr 1995).
.")
37
Soft neurological signs- undernourished adolescents Soft neurological signs observed in preschool years persisted affecting repetitive speed movements more with higher degree of overflow and dysrythmia (Agarwals-Nutr Res 1995). Thus chronic UN affects brain function for finger coordination.

38
Higher mental functions- undernourished adolescents Reaction time studies by Audio-visual RT apparatus and electromyograph:- showed affects on perceptual abilities, information processing and analytical capabilities (Agarwals-I J M R; 1998). Those who became normally nourished still had raised RT, due to early life UN.

39
BRAIN- MRI studies-in undernourished Adolescent MRI and cognitive evoked potential studies- Frontal lobes- Size was reduced & Asymmetry of anterior as well as posterior lobes was less pronounced. P3 latency was normal, but the P2 and P3 amplitudes were higher suggesting neuronal compensation. (Agarwals-Nutr Res 1996).
..")
40
No scientific study to show that nutrition supplement will improve the peak height velocity or the total height to compensate the stunting of early life. N F I-study-(Agarwals- IJMR-1989;) children 6-8 yr of age followed for 2 yr (preadolescent undernourished) with (450-500 kcal & protein10- 12g/ day), supplement given 172 days/yr.- did not show any height gain. LESSONS IN THIS AGE GROUP:
 children 6-8 yr of age followed for 2 yr (preadolescent undernourished) with ( kcal & protein10- 12g/ day), supplement given 172 days/yr.- did not show any height gain. LESSONS IN THIS AGE GROUP:.")
41
Other nutrition related adolescent health issues- Lesions of Atherosclerosis begin to accelerate. 1997-98 D. R. I.(Natl. Acad Sci, USA)-Folate 400ug/d-Prevents Atherosclerosis, clogging of arteries, heart attack, stroke- and reduce homocystein in smokersJAMA-1995 p1049-57. Vitamin E-10 IU, Prevents Ca-deposit in Bl. Vs; neutralizes oxidation of bad LDL cholesterol-RBC membrane antioxidant in smokers. LANCET-1996;p786. Cont.
-Folate 400ug/d-Prevents Atherosclerosis, clogging of arteries, heart attack, stroke- and reduce homocystein in smokersJAMA-1995 p Vitamin E-10 IU, Prevents Ca-deposit in Bl. Vs; neutralizes oxidation of bad LDL cholesterol-RBC membrane antioxidant in smokers. LANCET-1996;p786. Cont..")
42
Extremes of nutrition intake i) Overeating resulting in overweight and obesity; Induce rapid growth and early bone maturation; mestural functions; hypertension, diabetes, hyperlipidemia etc. ii) for social pressure to reach cultural ideals of thinness - excessive dieting e.g. anorexia nervosa- 1% (more in girls) and bulimia-can lead to renal failure, secondary amenorrhea irregular heart rate, bone marrow hypoplasia, osteoporosis and dental erosion.
 for social pressure to reach cultural ideals of thinness - excessive dieting e.g. anorexia nervosa- 1% (more in girls) and bulimia-can lead to renal failure, secondary amenorrhea irregular heart rate, bone marrow hypoplasia, osteoporosis and dental erosion..")
43
Dieting+ Intensive physical training for-thinness Alters hypothalamic-pitutary axis in adolescent girls – menstural functions altered and bone density reduced. Problems-Missing meals (girls)/reduced frequency/too much carbonated drinks, ice cream, french fries etc - low in macronutrient & micronutrients?
/reduced frequency/too much carbonated drinks, ice cream, french fries etc - low in macronutrient & micronutrients .")
44
Energy/ Protein/ Fat Needs around 136500Kcal as total cost of adolescent growth spurt.Peak energy needs- In girls with budding of mammary gland(SMR II-III) in boys(SMR-III-IV); 2200 and 3000Kcal resp/d Protein 12-14% of energy- Boys 0.34g/cm ht. Girls 0.28g/cm ht. Fat-<30% of total Kcal;7% saturated/ 10% polyunsaturated and 10% monounsaturated fat. Cholesterol ideally 200mg/day.

45
Cont.-Natl. Acad Sci USA-1997-98 Recommends-B-complex group :Pyridoxine1.3mg, Riboflavin 1.3mg, Niacin 16mg,Thiamin 1.2mg folate 400ug pantothenic acid 5.0mg, Biotin 25ug, Choline 550mg, --Important for cellular energy metabolism Vitamin C-Collagen synthesis Vitamin D for Ca absorption.

46
THANKS Welcome to write : e-mail adolcare@hotmail.com

Similar presentations