Download presentation
Presentation is loading. Please wait.

1
Anatomy and Physical Examination of the Lower Back
Sports Medicine Fellowship Uniformed Services University of the Health Sciences

2
Objectives Review the functional anatomy of Lumbar spine
Review Physical Examination of LS spine Correlate clinico-pathologic dx with pertinent physical findings

4
Epidemiology of back pain
The most common musculoskeletal disorder in industrialized societies Second only to common cold as cause of lost work time Estimated that ~ 80% of population will experience at least one disabling episode of back pain at some time during their lifetime The most common cause of disability in persons under the age of 45

5
Epidemiology of back pain (cont.)
When compensation from lost work, long-term disability, and medical and legal expenses are considered, is the most costly of all medical dx’s

6
PATIENT HISTORY “OPQRSTU”
Onset Palliative/Provocative factors Quality Radiation Severity/Setting in which it occurs Timing of pain during day Understanding - how it affects the patient Onset Palliative/Provocative factore Quality Radiation Severity/Setting in which it occurs Timing of pain during day Understanding - how it affects the patient

7
“Red Flags” in back pain
Hx of cancer Unrelenting nocturnal pain Weight loss Fever, chills, night sweats Age < 15 or > 50 Neurologic deficits Decreased motor and/or sensory innervation Urinary and/or fecal incontinence

8
Anatomy Vertebra Body, anteriorly Functions to support weight
Vertebral arch, posteriorly Formed by two pedicles and two laminae Functions to protect neural structures

9
Vertebral arch 7 vertebral processes arise from vertebral arch
3 lever-like processes - provide attachments sites for ligaments and muscles Spinous process 2 Transverse processes 4 articular processes Arise from junction of pedicle and laminae

10
Vertebral Arch Space enclosed by body and vertebral arch is the vertebral foramen Successive vertebral foramen form the vertebral canal

12
Ligaments Anterior longitudinal ligament
Posterior longitudinal ligament Interspinous ligament Supraspinous ligament Ligamentum flavum

14
Intervertebral Disc Most common site of back pain
Normally comprises ~ 25% of length of spine Consists of a central nucleus pulposus Reticulated and collagenous substance Composed of ~ 88% water Annulus fibrosus Consists of concentric lamellae of fibrocartilage fibers arranged obliquely With each layer, they are arranged in opposite directions

16
Facet Joint Formed by articulation of inferior and superior processes of subsequent vertebrae Orientation in lumbar spine is toward sagittal plane, allowing flexion and extension but limiting rotation of the lumbar vertebrae Helps to prevent anterior movement of superior vertebra on inferior vertebra Articular surfaces are made up of noninnervated articular cartilage Capsule and synovial membrane are innervated with pain receptors

19
Physical Examination Inspection Palpation Bony Soft Tissue
Range of Motion Neurologic Examination Special Tests

20
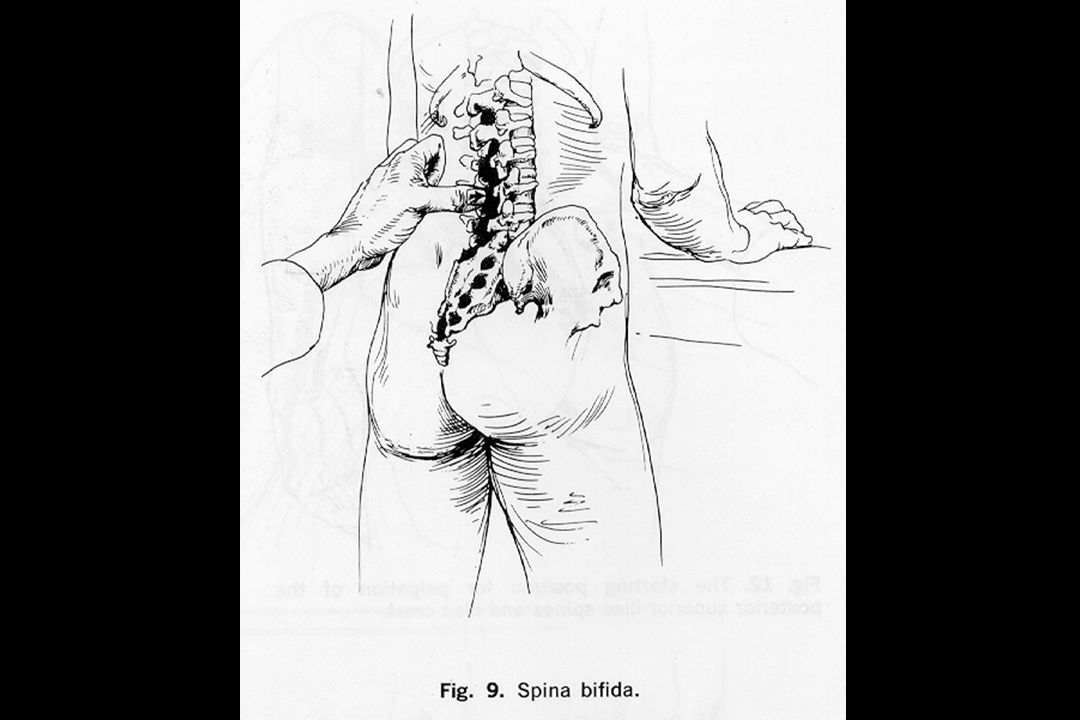
Inspection Observe for areas of erythema Infection
Long-term use of heating element Unusual skin markings Café-au-lait spots Neurofibromatosis Hairy patches (Faun’s beard) Lipomata Spina bifida
 Lipomata. Spina bifida.")
22
Inspection (cont.) Posture Shoulders and pelvis should be level
Bony and soft-tissue structures should appear symmetrical Normal lumbar lordosis Exaggerated lumbar lordosis is common characteristic of weakened abdominal wall

25
Bone Palpation Palpate L4/L5 junction (level of iliac crests)
Palpate spinous processes superiorly and inferiorly S2 spinous process at level of posterior superior iliac spine Absence of any sacral and/or lumbar processes suggests spina bifida Visible or palpable step-off indicative of spondylolisthesis

29
Common area of pain due to low back sprains or the avulsion of a tendon from the posterior superior iliac spines

30
ANTERIOR PALPATION ANTERION PALPATION
Anteriorly, umbilicus lies at L3-L4 disc space, the point where aorta divides into common iliacs Anterior portions of L4, L5, and S1 vertebral bodies and discs are palpable below the aorta’s division

31
Soft Tissue Palpation 4 clinical zones Midline raphe
Paraspinal muscles Gluteal muscles Sciatic area Anterior abdominal wall and inguinal area

32
Palpate as a unit on either side of midline
Note any tenderness, spasm, defects, or dissimilarity

34
Sciatic nerve exits pelvis thru greater sciatic foramen under the piriformis muscle
Midway between the greater trochanter and ischial tuberosity To palpate the sciatic nerve, have pt flex hip, and locate the midpoint Herniated disc or lesion compressing the nerve roots can cause tenderness to palpation

35
Have pt perform abdominal crunch, then palpate each segment of rectus abdominis, noting any weakness or deficit Abdominal muscles are segmental and receive segmental innervation Pain in inguinal area usually indicates pathology in hip joint

37
Range of Motion Flexion Extension Lateral Bending Rotation

41
Flexion - 80º Extension - 35º Side bending - 40º each side Twisting º

42
Neurologic Examinaion
Includes an exam of entire lower extremity, as lumbar spine pathology is frequently manifested in extremity as altered reflexes, sensation and muscle strength Describes the clinical relationship between various muscles, reflexes, and sensory areas in the lower extremity and their particular cord levels

43
Neurologic Examination (T12, L1, L2, L3 level)
Motor Iliopsoas - main flexor of hip With pt in sitting position, raise thigh against resistance Reflexes - none Sensory Anterior thigh

44
Neurologic Examination (L2, L3, L4 level)
Motor Quadriceps - L2, L3, L4, Femoral Nerve Hip adductor group - L2, L3, L4, Obturator N. Reflexes Patellar - supplied by L2, L3, and L4, although essentially an L4 reflex and is tested as such

45
L2, L3, L4 testing

46
Neurologic Examination (L4 level)
Motor Tibialis Anterior Resisted inversion of ankle Reflexes Patellar Reflex (L2, L3, L4) Sensory Medial side of leg
 Sensory. Medial side of leg.")
47
L4 LEVEL Motor: Tibialis Anterior -Resisted inversion of ankle Reflexes: Patellar Reflex Sensory: L4 dermatome covers medial side of leg

48
Neurologic Examination (L5 level)
Motor Extensor Hallicus Longus Resisted dorsiflexion of great toe Reflexes - none Sensory Dorsum of foot in midline

49
L5 LEVEL Motor: Extensor Hallicus Longus -Resisted dorsiflexion of great toe Reflexes - none Sensory: Dorsum of foot in midline

50
Neurologic Examination (S1 level)
Motor Peroneus Longus and Brevis Resisted eversion of foot Reflexes Achilles Sensory Lateral side of foot

51
S1 LEVEL: Motor: Peroneus Longus and Brevis -Resisted eversion of foot Reflexes: Achilles Sensory: Lateral side of foot

52
Special Tests Tests to stretch spinal cord or sciatic nerve
Tests to increase intrathecal pressure Tests to stress the sacroiliac joint

53
Tests to Stretch the Spinal Cord or Sciatic Nerve
Straight Leg Raise Cross Leg SLR Kernig Test

56
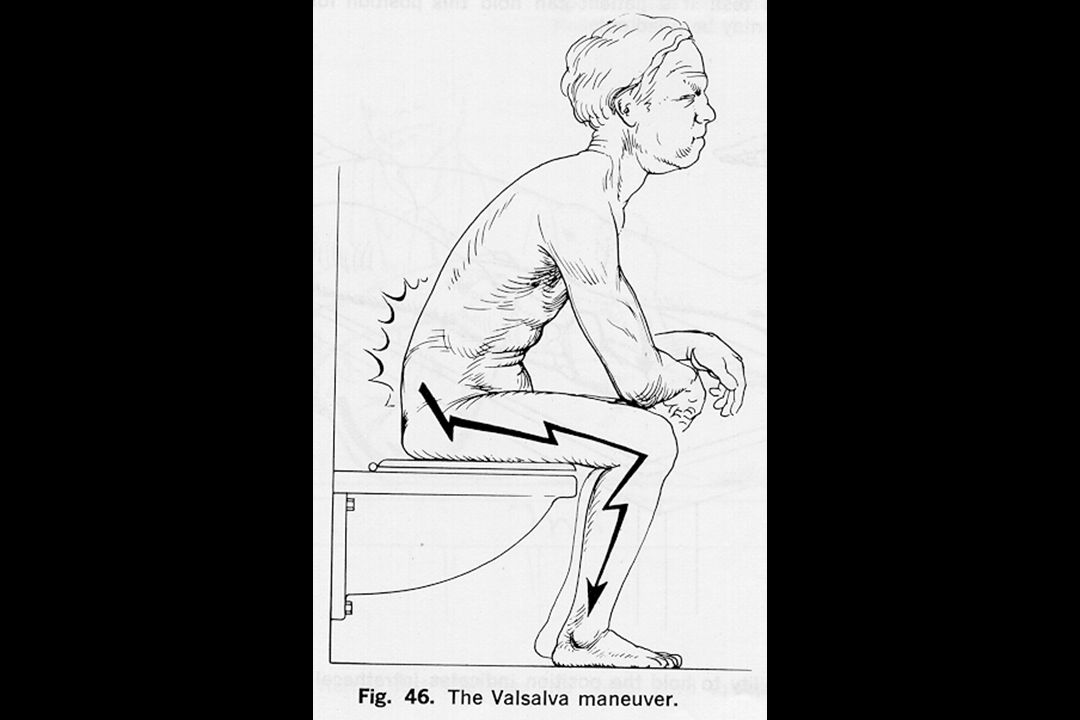
Test to increase intrathecal pressure
Valsalva Maneuver Reproduction of pain suggestive of lesion pressing on thecal sac

58
Tests to stress the Sacroiliac Joint
Pelvic Rock Test FABER Test

60
Flexion A- Bduction External Rotation

61
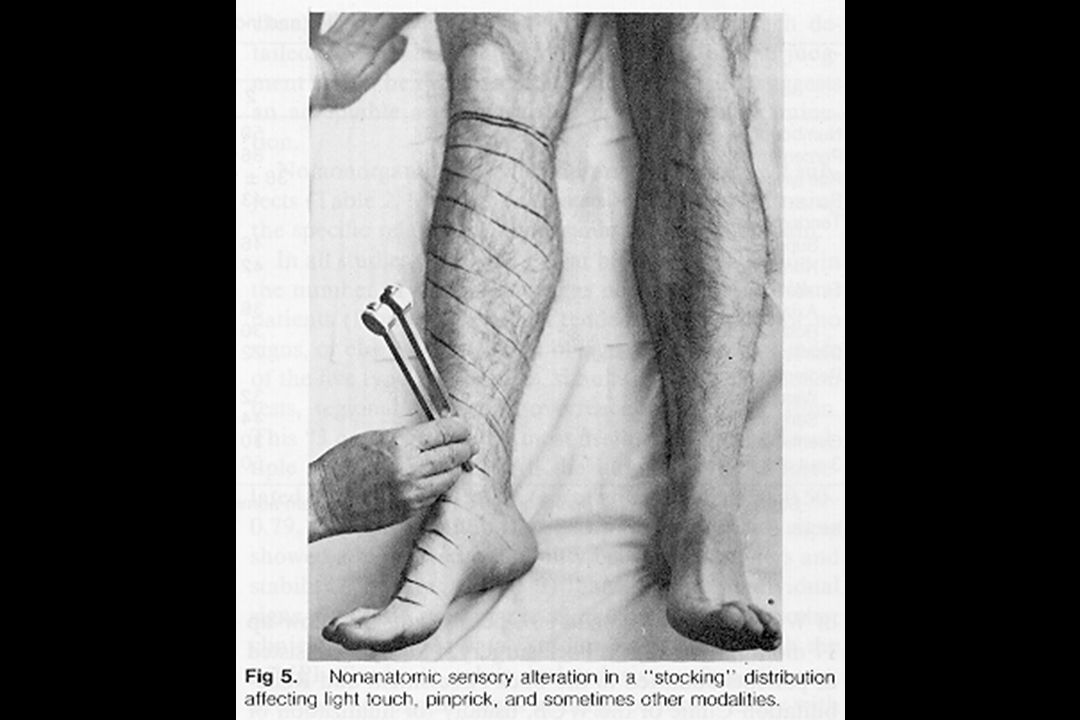
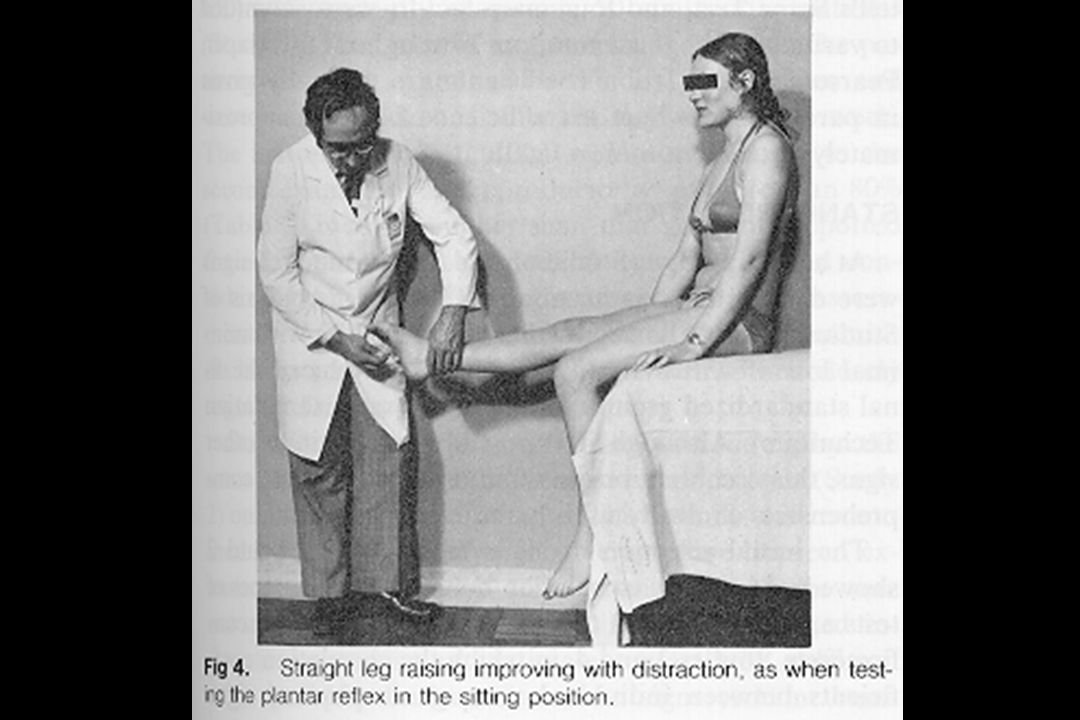
Non-organic Physical Signs (“Waddell’s signs”)
Non-anatomic superficial tenderness Non-anatomic weakness or sensory loss Simulation tests with axial loading and en bloc rotation producing pain Distraction test or flip test in which pt has no pain with full extension of knee while seated, but the supine SLR is markedly positive Over-reaction verbally or exaggerated body language Waddell, et al. Spine 5(2): , 1980.
: ,")
67
Hoover Test Helps to determine whether pt is malingering
Should be performed in conjunction with SLR When pt is genuinely attempting to raise leg, he exerts pressure on opposite calcaneus to gain leverage

70
Common Causes of Low Back Pain
Muscular spasm, strain Ligament sprain Spondylosis Herniated nucleus pulposus Facet joint dysfunction Spondylo-lysis or -listhesis Seronegative spondyloarthropathies

71
Clearing up the terms Spondylosis
Degenerative joint disease affecting the vertebrae and intervertebral disc Spondylolysis Fracture in pars interarticularis Spondylolisthesis Displacement of one vertebra on another

72
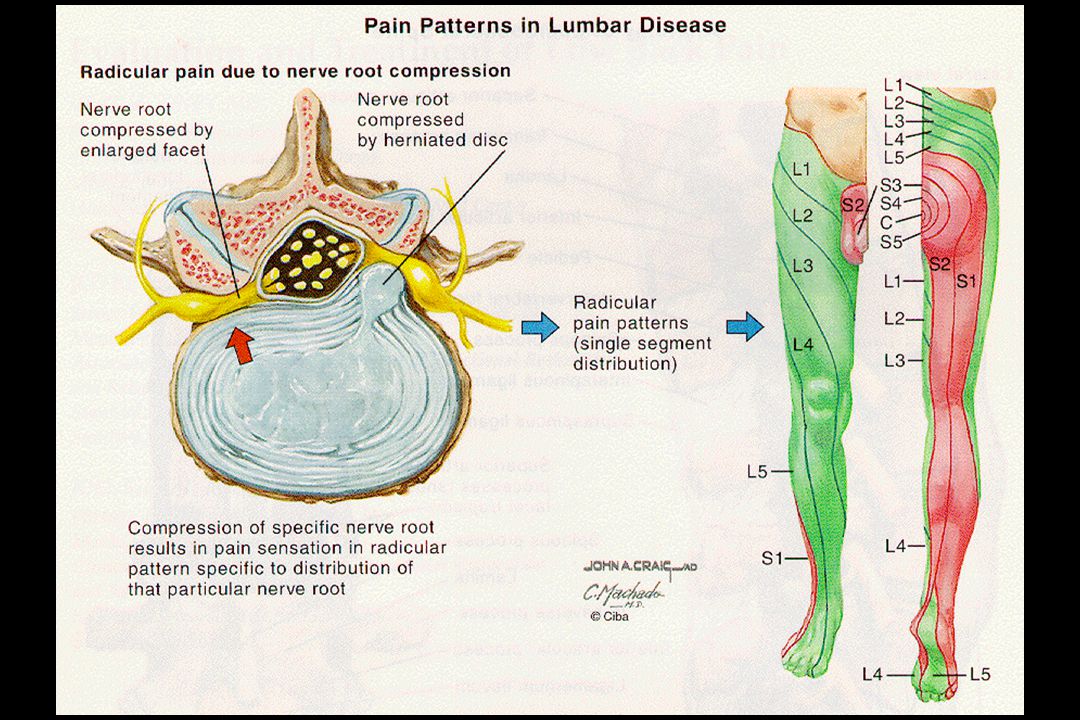
Disc rupture and herniation

75
Spondylo-lysis and -listhesis

79
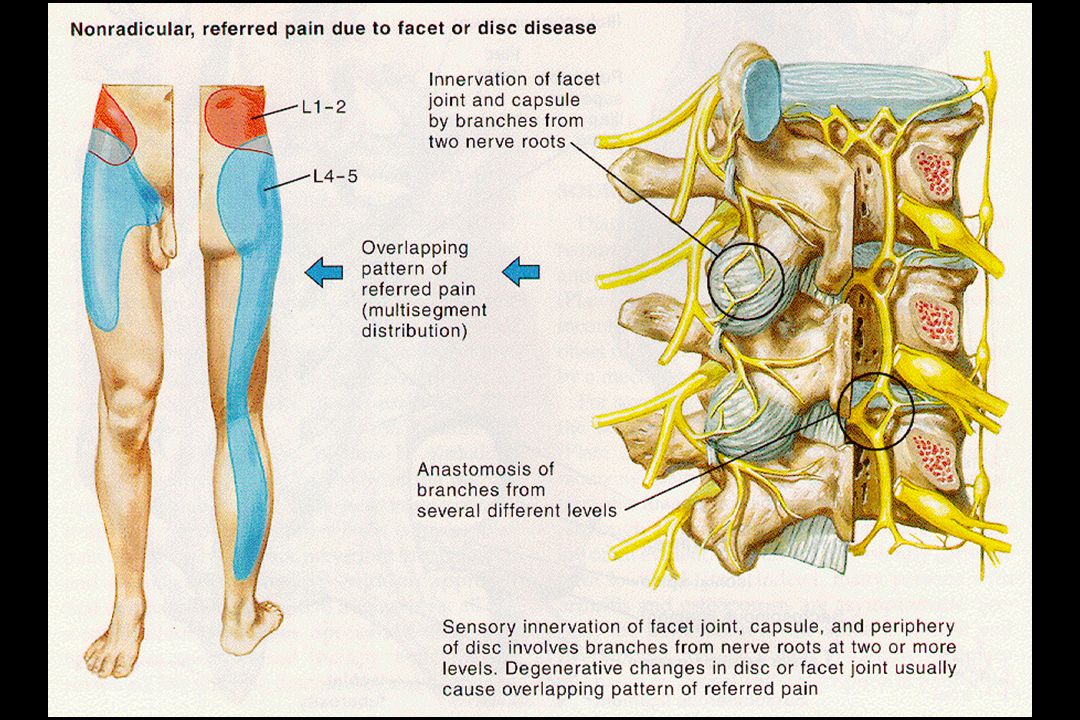
Facet joint pain

81
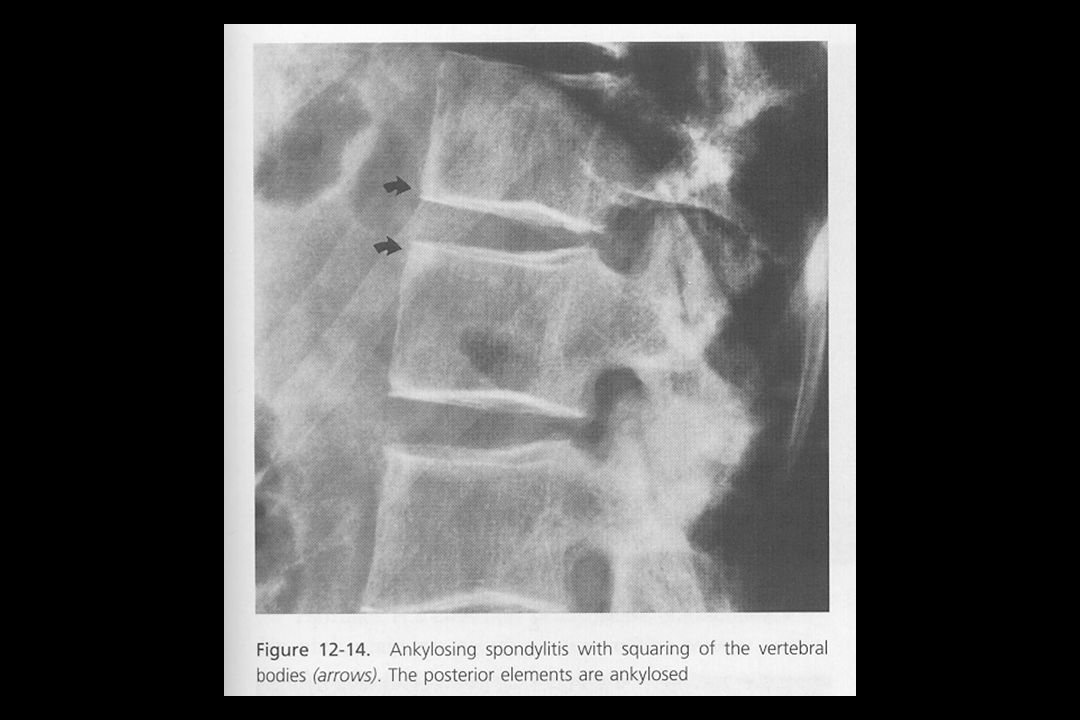
Ankylosing spondylitis

Similar presentations
































>")
















