Download presentation
Presentation is loading. Please wait.

1
Medical Treatment of Obesity
F.Hosseinpanah,M.D Endocrine Research Center Shahid Beheshti University of Medical Sciences 2th Iranian congress of obesity 29-30 Oct,2009 Tehran

2
Outline Introduction Sibutramine Orlistat Other drugs
Critical appraisal Conclusion

3
Some important Questions
Head-to-head comparisons of approved agents Long-term safety and efficacy of older drugs (e.g., phenteramine) Combination therapy Treatment of children and adolescents Treatment of elderly Identification of patients with a response to treatment Do drugs confer long-term, individual and population, reductions in morbid and mortal squeal of obesity
 Combination therapy. Treatment of children and adolescents. Treatment of elderly. Identification of patients with a response to treatment. Do drugs confer long-term, individual and population, reductions in morbid and mortal squeal of obesity.")
6
Outcome Measures Weight Waist W/H ratio Lipid profile BP , HR
Hb A1c , c peptide , Insulin Conversion of IGT to DM

7
Measures of weight loss
Mean weight loss ( Kg ) Percentage weight loss Percentage of individuals losing ≥ %5 or ≥ %10 of baseline weight Maintenance of weight loss during study Absolute weight loss (i.e. in excess of placebo )
 Percentage weight loss. Percentage of individuals losing ≥ %5 or ≥ %10 of baseline weight. Maintenance of weight loss during study. Absolute weight loss (i.e. in excess of placebo )")
8
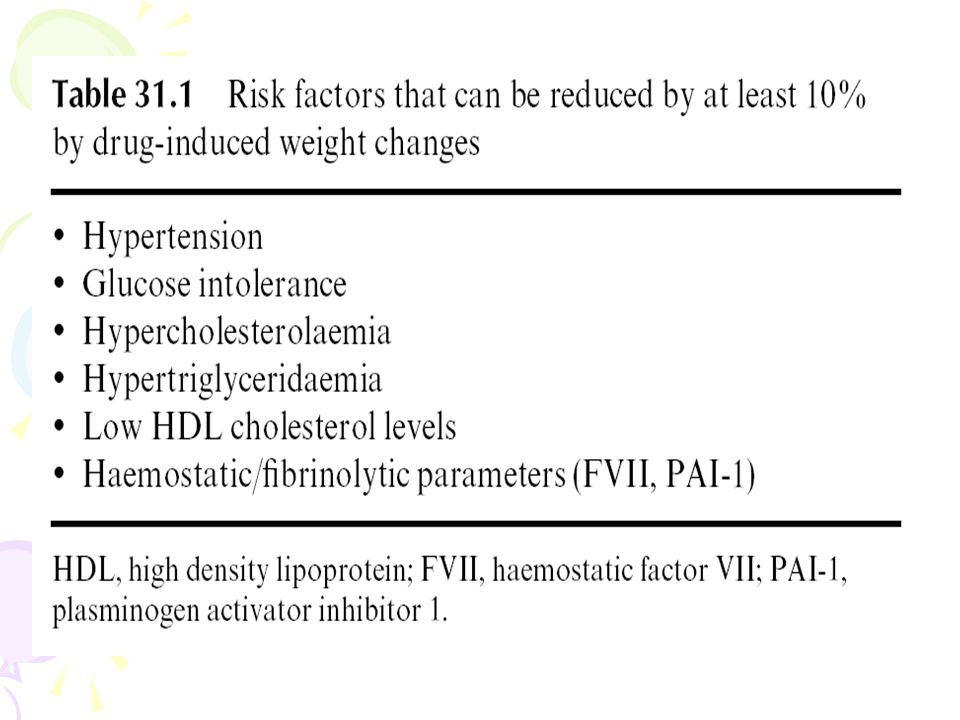
Potential benefits of weight loss
weight loss in overweight and obese patients - even as little as five to ten percent of initial body weight – is associated with an improvement in cardiovascular risk factors (Goldstein 1992; Blackburn 1995; Colditz 1995)
")
10
Obesity Guidance: Efficacy Criteria
US FDA criteria at the end of year 1: Mean placebo-subtracted weight loss > 5% Proportion of subjects who lose > 5% of baseline body weight is greater in drug- vs. placebo-treated group EMEA* criteria at end of year 1: mean placebo-subtracted weight loss > 10% Proportion of patients who lose > 10% of baseline body weight is greater in drug- vs. placebo-treated group *Europeans Medicines Evaluation Agency

11
Sibutramine The brand name is Meridia
Sibutramine induces weight loss primarily through its effects on food intake and to a lesser degree through its effect on metabolic rate. Sibutramine affects serotonin and norepinephrine metabolism in the brain by stimulating satiety at the appetite centers in the brain. Rapid absorption , peak plasma concentration are reached within one or two hours

12
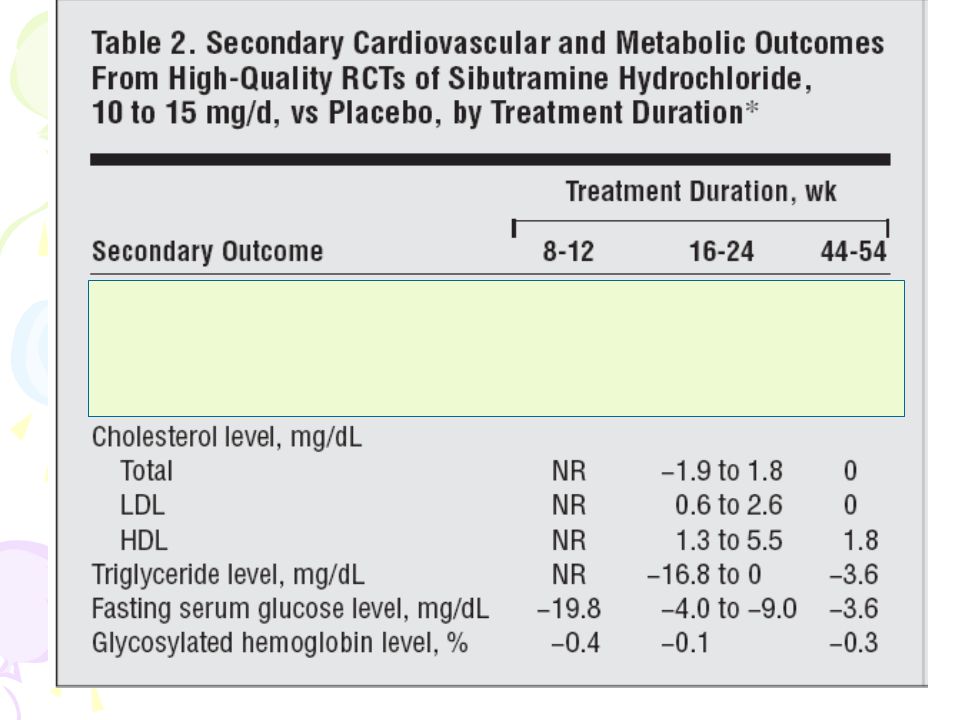
ARCH INTERN MED/VOL 164, MAY 10, 2004

13
Inclusion Criteria (1) randomized controlled trial
(2) sibutramine, 10 to 20 mg/d, was administered (3) placebo controlled trial (4) overweight or obese subjects (BMI≥25) (5) subjects were aged 18 years or older (6) weight loss was assessed (7) 8-week duration or longer (8) 29 studies were pooled
 sibutramine, 10 to 20 mg/d, was administered. (3) placebo controlled trial. (4) overweight or obese subjects (BMI≥25) (5) subjects were aged 18 years or older. (6) weight loss was assessed. (7) 8-week duration or longer. (8) 29 studies were pooled.")
15
-5.06(-6.16to-3.96)
")
16
-4.45Kg(-5.29 to -3.62)
")
19
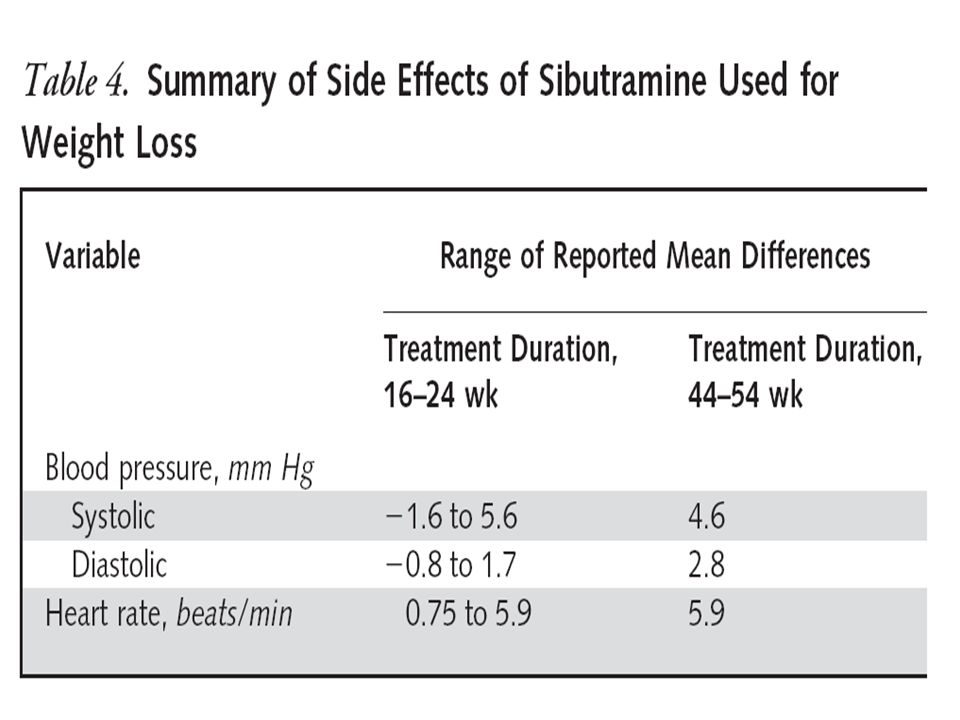
What About Side Effects?
Common side effects include: Dry mouth Headache Constipation Insomnia Increased blood pressure

20
THE LANCET • Vol 356 • December 23/30, 2000

21
%3 withdrawal in sibutramine group due to excessive BP increases

23
(J Clin Endocrinol Metab 90: 1460–1465, 2005)
")
24
RCT Sample size: 60 adolescents, aged 14–17 yr F/U:6 months Intervention: sibutramine (10 mg/d) or matching placebo Outcome: weight, waist, Hip, BP, lipid profile, echocardiogram

28
Ann Intern Med. 2006;145:81-90.

29
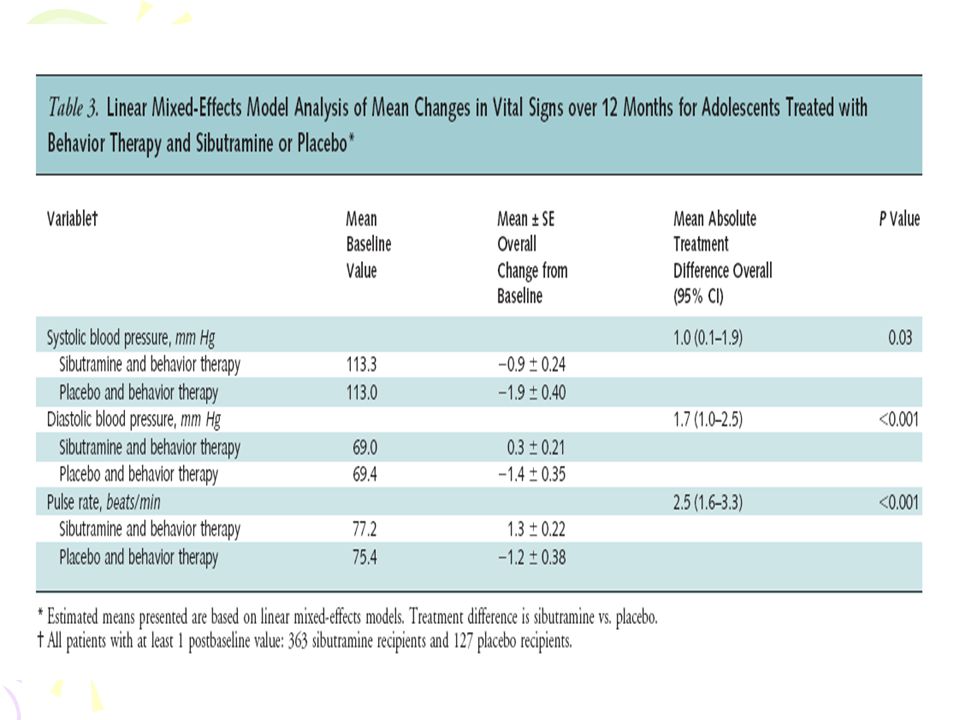
RCT Participants: 498 participants 12 to 16 years of age with a body mass index (BMI) that was at least 2 units more than the U.S. weighted mean of the 95th percentile based on age and sex, to the upper limit of 44 kg/m2. Setting: 33 U.S. outpatient clinics. Interventions: Site-specific behavior therapy plus 10 mg of sibutramine or placebo. Blinded study medication dose was up titrated to 15 mg or placebo at month 6 if initial BMI was not reduced by 10% Length of F/U: 12 mo. Measurements: Body mass index, waist circumference, body weight, fasting lipid and glycemic variables, safety, and tolerability.
 that was at least 2 units more than the U.S. weighted mean of the 95th percentile based on age and sex, to the upper limit of 44 kg/m2. Setting: 33 U.S. outpatient clinics. Interventions: Site-specific behavior therapy plus 10 mg of sibutramine or placebo. Blinded study medication dose was up titrated to 15 mg or placebo at month 6 if initial BMI was not reduced by 10% Length of F/U: 12 mo. Measurements: Body mass index, waist circumference, body weight, fasting lipid and glycemic variables, safety, and tolerability.")
33
Cautions Only 76% and 62% of the sibutramine and placebo recipients, respectively, completed the trial.

34
Implications Sibutramine plus behavioral therapy for 1 year can reduce weight and improve metabolic risk factors in some very obese adolescents.

35
Orlistat The Brand name is Xenical
Orlistat prevents the digestion of dietary fat. It inactivates pancreatic lipase that is involved with fat digestion , and about 30 percent less fat is absorbed. Less than %1 is absorbed . It does not alter the pharmacokinetics of digoxin , phenytoin , warfarin , glyburide ,ocp , alcohol , furosemide ,captopril , nifedipine , or atenolol

36
Orlistat meta analysis
22 studies were pooled Average age , 48 years Average BMI , 36.7 Kg/m Seventy-three percent were women Meta-Analysis: Pharmacologic Treatment of Obesity, Ann Intern Med. 2005;142:

37
-2.75Kg (-3.31 to -2.20)
")
40
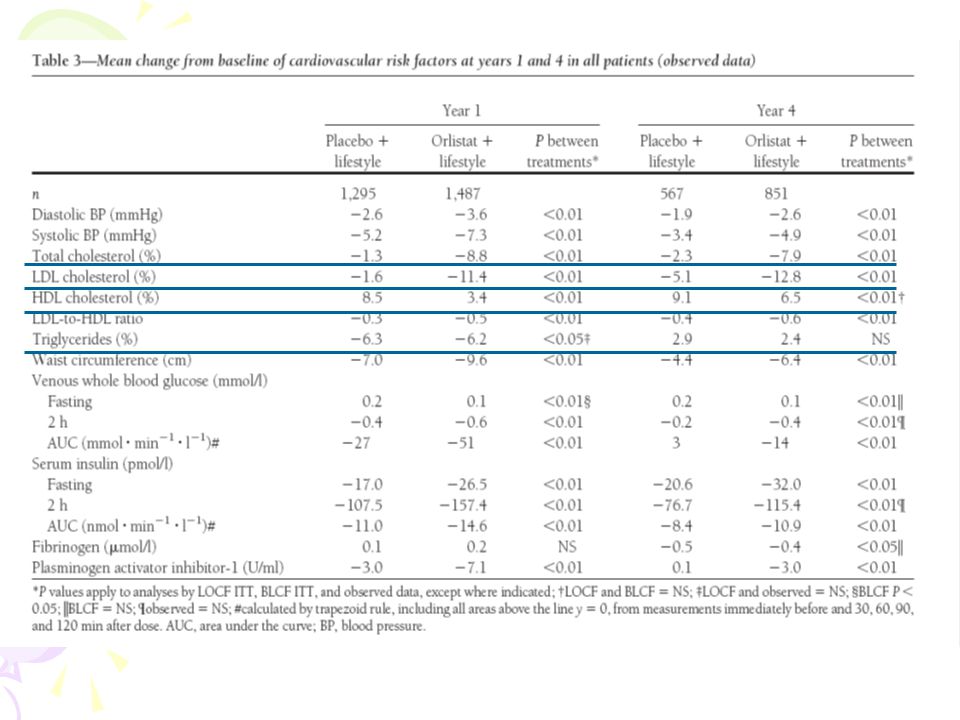
N = 3305 , BMI ≥ 30 F/U = 4 y Diet + placebo VS DIET + orlistat ( 120 mg TDS ) DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY 2004
 DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY")
41
Attrition rate = %54 in the orlistat and %34 in the placebo

43
What About Side Effects?
Gastrointestinal symptoms Increased flatus Abdominal discomfort Oily spotting Fecal Incontinence More severe if intake of fat is more than 100 grams. Nutritional concerns Fat-soluble vitamins may be malabsorbed. Daily multi-vitamin is recommended

44
Side Effects In clinical trials, 1.1–6% of patients treated with orlistat and 0.6–1.3% of placebo recipients withdrew because of gastrointestinal adverse event In a large 2-year, double-blind, multicentre study, vitamin supplementation was required in 14.1% of orlistat treated patients and in 6.5% of placebo-treated patients Drug Safety 2006; 29 (4):
:")
45
JAMA. 2005;293:

46
Participants: 539 obese adolescents aged 12-16 years ,BMI 2 units above the 95th percentile.
F/U: 54 weeks Setting: 32 centers in the United States and Canada Interventions: 120-mg dose of orlistat VS placebo Outcomes: BMI, Waist,Hip, glucose and insulin responses to oral glucose challenge ,Lipid profile , DEXA Similar proportions of participants in each treatment group completed the study (65% for orlistat and 64% for placebo).
.")
50
Generally mild to moderate gastrointestinal tract adverse events occurred in 9% to 50% of the orlistat group and in 1% to 13% of the placebo group.

51
phentermine six placebo controlled RCTs contributed data to the pooled analysis. The duration of treatment with phenteramine varied from 2 to 24 weeks. Mean Weight Change in Treated Patients Compared with Placebo (95% CI) was 3.6 kg ( 0.6 to 6.0 kg) Pharmacotherapy for obesity: a quantitative analysis of four decades of published randomized clinical trials. Int J Obes Relat Metab Disord. 2002;26:262-73
 was 3.6 kg ( 0.6 to 6.0 kg) Pharmacotherapy for obesity: a quantitative analysis of four decades of published randomized clinical trials. Int J Obes Relat Metab Disord. 2002;26:")
52
Diethylpropion Nine Placebo controlled RCTs contributed data to the pooled analysis. The duration of treatment with diethylpropion varied from 6 to 52 weeks. More than 80% of enrolled individuals were female Mean Weight Change in Treated Patients Compared with Placebo (95% CI ) was 3.0 kg ( 1.6 to 11.5 kg) Pharmacotherapy for obesity: a quantitative analysis of four decades of published randomized clinical trials. Int J Obes Relat Metab Disord. 2002;26:262-73
 was 3.0 kg ( 1.6 to 11.5 kg) Pharmacotherapy for obesity: a quantitative analysis of four decades of. published randomized clinical trials. Int J Obes Relat Metab Disord. 2002;26:")
54
Drug treatment in obese elderly adults

55
prevalence Seventy percent to 77% of adults between the ages of 65 to 74 are overweight For adults 75 years and older, the incidence is 60% to 66% The occurrence of obesity among older adults ranges from 33% to 39% for those 65 to 74 years of age and 20% to 25% for those 75 years and older CDC, National Center for Health Statistics, National Health and Nutrition Examination Survey. Health, United States (Table 70); 2002.
;")
56
Age<65 Age >65 Normal 23.7 (541) 33.3 (346) Overweight
Prevalence of excess weight in subjects aged 50 years and over in Tehran ( Tehran Lipid and Glucose Study) Age<65 Age >65 Normal 23.7 (541) 33.3 (346) Overweight 43.7 (998) 44.9 (467) Obesity 32.6 (745) 21.8 (226)
 Age<65. Age >65. Normal (541) 33.3 (346) Overweight (998) 44.9 (467) Obesity (745) 21.8 (226)")
57
The main issues in elderly
Impaired gastric absorption and motility The effects of altered body composition on drug distribution Impaired renal and hepatic function High likelihood of concurrent morbidities and use of polypharmacy , producing the possibility of drug interactions.

58
Most of the trials , recruited patients under 65 years of age.

60
Continued..

61
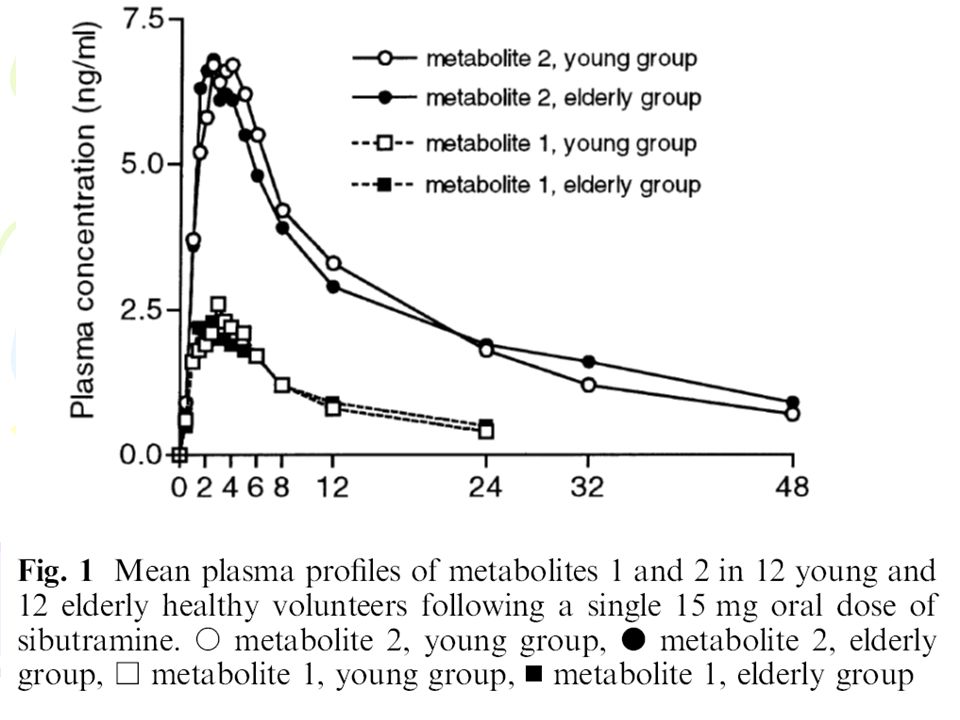
Segal KR, Lucas C, Boldrin M, et al
Segal KR, Lucas C, Boldrin M, et al. Weight loss efficacy of orlistat in obese elderly adults. J Obes Research 1999;7(Suppl 1):26. Hind ID, Mangham JE, Ghani SP, et al. Sibutramine pharmacokinetics in young and elderly healthy subjects. Eur J Clin Pharmacol 1999;54(11):847– 9.
:26. Hind ID, Mangham JE, Ghani SP, et al. Sibutramine pharmacokinetics in young and elderly healthy subjects. Eur J Clin Pharmacol 1999;54(11):847– 9.")
65
Pharmacologic therapy has not been sufficiently studied in adults older than 65 years of age, so weight loss medications are usually not recommended. If a clinician suspects a patient who has obesity may improve with drug therapy and wishes to start an agent, orlistat may be a better choice than sibutramine or phentermine.

67
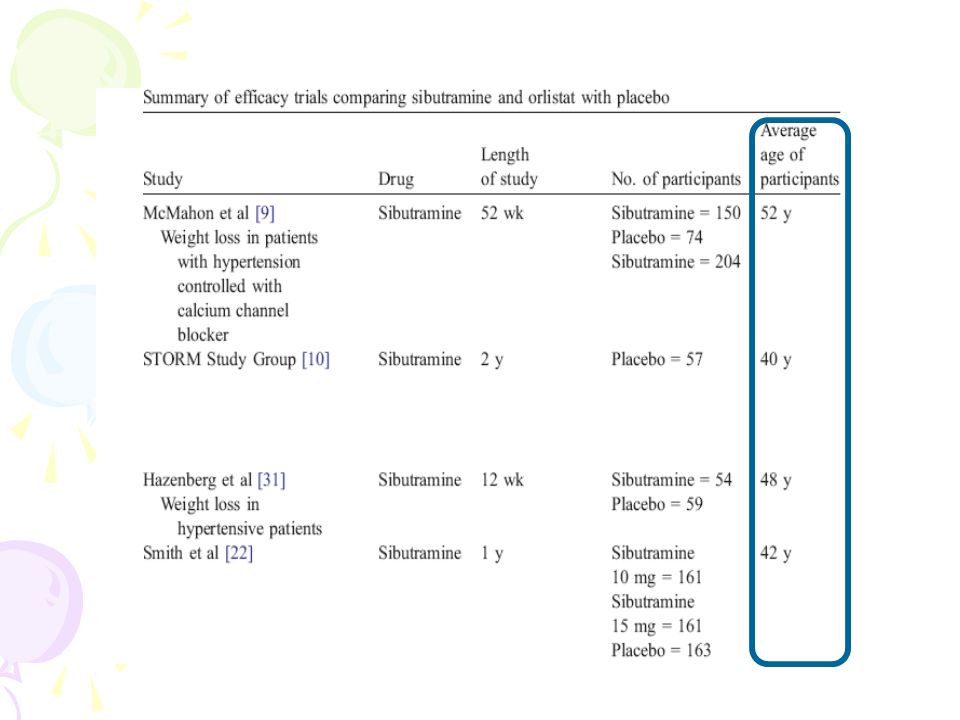
Eight such studies were found comparing weightloss of orlistat and sibutramine
Four of the seven studies comparing sibutramine and orlistat mono-therapy showed that sibutramine was significantly more efficacious for weight loss The weighted mean difference in weight loss was 2.2 kg (95% CI 0.5–3.9) favouring sibutramine.
 favouring sibutramine.")
68
Three studies investigated orlistat and sibutramine as combination therapy, and two found it to be significantly better than orlistat alone, but not better than sibutramine alone No significant difference in dropout rate was seen, although the point estimate indicated a lower risk in sibutramine-treated patients

71
Pharmacotherapy Drugs approved for long-term use by the FDA may be used as part of a comprehensive weight loss program including diet and physical activity. Evidence Category B. For patients with a BMI of 30 or above with no concomitant risk factors or diseases For patients with a BMI of 27 or above for those with concomitant risk factors or diseases (hypertension, dyslipidemia, CHD, type 2 diabetes, sleep apnea) If after at least 6 months on a weight loss regimen of an LCD, increased physical activity, and behavior therapy, pharmacotherapy can be considered as part of a comprehensive program for the following patients: Patients with a BMI 30 who have not lost the recommended 1lb/week on lifestyle therapy. Other patients with a BMI of 27 to 29.9 if they have hypertension, dyslipidemia, CHD, type 2 diabetes, or sleep apnea. There are few long-term studies evaluating the safety or effectiveness of many currently approved weight loss medications. At present, sibutramine and orlistat are the only drugs available for long-term use. Weight loss medications should be used only by patients who are at increased medical risk because of their weight and should not be used for cosmetic weight loss.
 If after at least 6 months on a weight loss regimen of an LCD, increased physical activity, and behavior therapy, pharmacotherapy can be considered as part of a comprehensive program for the following patients: Patients with a BMI 30 who have not lost the recommended 1lb/week on lifestyle therapy. Other patients with a BMI of 27 to 29.9 if they have hypertension, dyslipidemia, CHD, type 2 diabetes, or sleep apnea. There are few long-term studies evaluating the safety or effectiveness of many currently approved weight loss medications. At present, sibutramine and orlistat are the only drugs available for long-term use. Weight loss medications should be used only by patients who are at increased medical risk because of their weight and should not be used for cosmetic weight loss.")
72
Some important Questions
Head-to-head comparisons of approved agents Long-term safety and efficacy of older drugs (e.g., phenteramine) Combination therapy Treatment of children and adolescents Treatment of elderly Identification of patients with a response to treatment Do drugs confer long-term, individual and population, reductions in morbid and mortal squeal of obesity
 Combination therapy. Treatment of children and adolescents. Treatment of elderly. Identification of patients with a response to treatment. Do drugs confer long-term, individual and population, reductions in morbid and mortal squeal of obesity.")
73
Critical appraisal Methodological quality was moderate or good
blinding High attrition rate Run in period Last observation carry forward analysis (LOCF) Younger and older people Sex , ethnicity , social class High risk vs low risk groups Recruitment method
 Younger and older people. Sex , ethnicity , social class. High risk vs low risk groups. Recruitment method.")
74
Critical appraisal A careful assessment of the safety of antiobesity medications may be more important than for drugs used to treat other conditions , in which the drugs are less liable to misused. Obesity is a chronic condition. In light of this, longer-term data on the effectiveness and safety would be helpful.

75
Conclusions The most well-studied medications are sibutramine and orlistat Mean weight loss was 2.8–5.7kg more for sibutramine 10–20 mg/day than placebo Mean weight loss was 1.3–4.2kg more for orlistat120mg three times daily than placebo Weight loss attributable to these medications are modest but still may be clinically significant The maximal duration of published treatment results is two years for sibutramine and four years for orlistat When drug therapy is discontinued , weight is regained Near maximal weight loss is achieved by six months in most trials There are no data on cardiovascular outcomes and mortality For obese patients with HTN or dyslipidemia , orlistat can be considered as first line Pharmacologic therapy can be offered to obese patients who have failed to achieve their weight loss goals through diet and exercise alone. However, there needs to be a doctor–patient discussion of the drugs’ side effects, the lack of long-term safety data, and the temporary nature of the weight loss achieved with medications before initiating therapy.

76
With better understanding of complexity of energy balance regulation
Ultimately , goal must be to use this understanding to develop more effective strategies not only for treatment , but also for the primary prevention of obesity

77
Thanks for your kind attention

Similar presentations