Download presentation
Presentation is loading. Please wait.

1
Radiology of urinary system Dr. Sameer Abdul Lateef

2
* Infestation by Schist. Haematobium. *The ova deposited into sub-mucosa of urinary bladder and to less extent at the wall of ureters. *The ova calcify and excrete toxin producing necrosis of tissue lead to granulomatous tubercles and extensive fibrosis. *Calcification is very common and important diagnostic findings. Very common in bladder,less frequent in lower ureters,but in advanced case involve the whole length of ureter. *The appearance depends on degree of fullness of bladder ; thin linear opacity outlining bladder wall. Empty bladder shows crowded linear opacities with calcified plaques. Empty bladder shows crowded linear opacities with calcified plaques.

3
IVU: Early stage – cobble stone Later filling defects due to graneulomatos papilloma Carcinoma is important complication Ureters : dilated and tortuous In early stage hydroureter and hydronephrosis + reflux IVU: Early stage – cobble stone Later filling defects due to graneulomatos papilloma Carcinoma is important complication Ureters : dilated and tortuous In early stage hydroureter and hydronephrosis + reflux

4
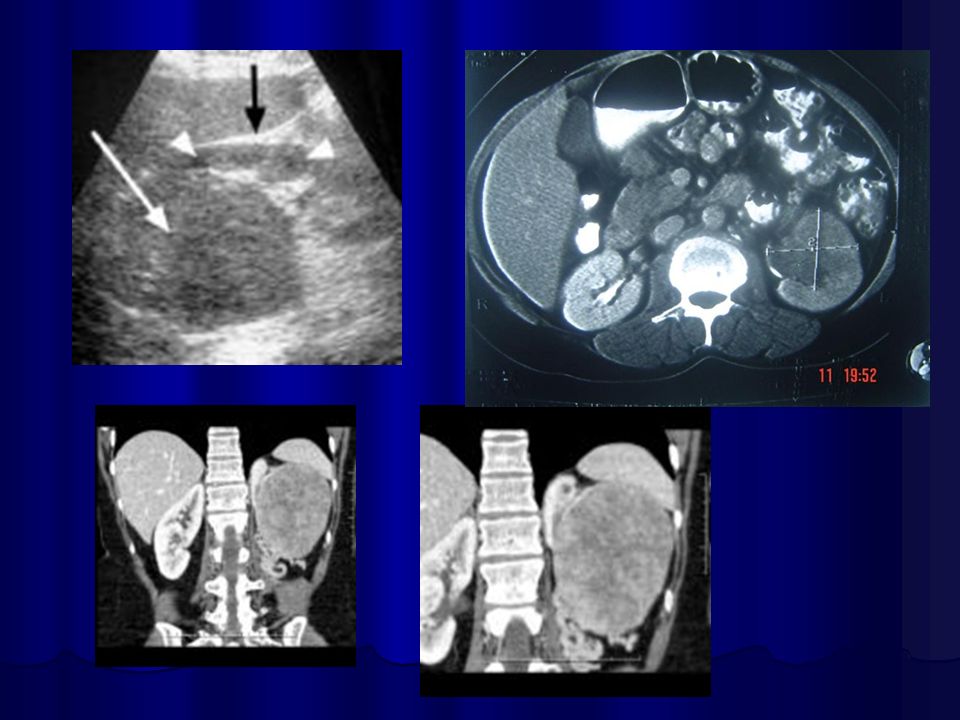
SPACE OCCUPING LESION SIMPLE RENAL CYST * Common cause of renal mass. * Uncommon under age of 30 years, most common over 50 years. * Single or multiple. * Usually cortical in origin. * Varies in size ; few mm to 25 cm. * Contains straw color fluid, with thin fibrous wall lines by flat epithelium. * Clinically silent, large cyst can shows palpable mass. * Calcification is rare, normal renal function.

5
Renal cyst cont. KUB : 1- Cyst in upper pole displace kidney downward. Cyst at medial surface displace the kidney laterally.with enlarged kidney 2- Smooth local bulge of renal out-line. 3- Calcifications rare 3% usually in hemorrhagic cyst.

6
Renal S.O.L (cyst)
")
7
RENAL CYST IVU :- * Nephrogram shows filling defect. *Displacement, elongation & stretching of PCS which depend on size and site of the cyst. US :- US :- shows echo-free cystic lesion with posterior enhancement. shows echo-free cystic lesion with posterior enhancement.

10
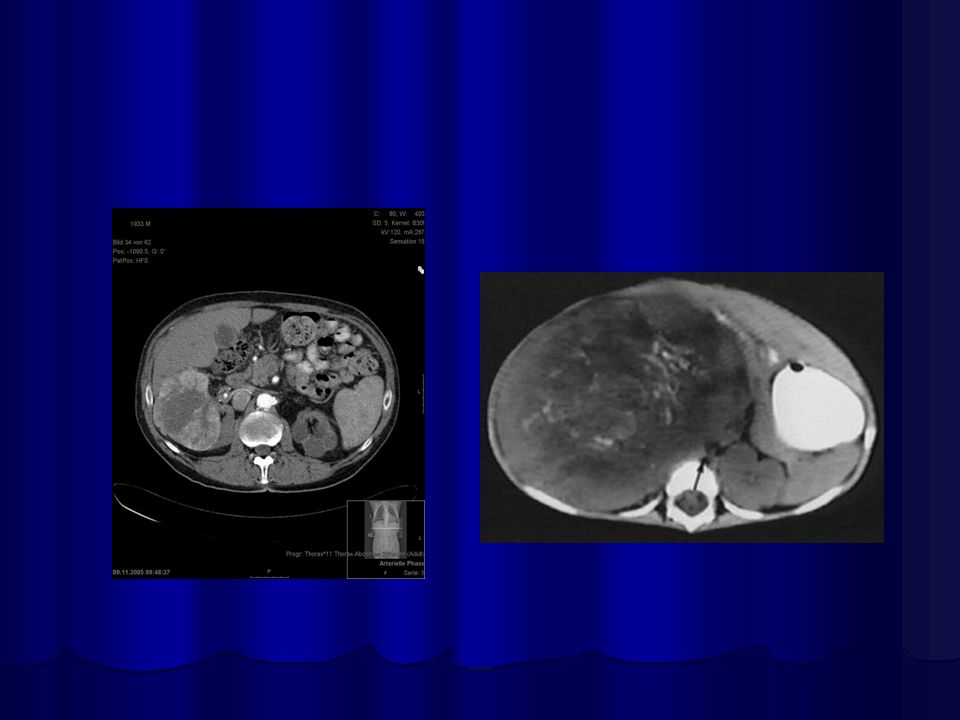
RENAL TUMOR Adenocarcinoma ( Hyper nephroma) * Comprise 80% of renal malignant tumor. next epithelial T. of renal pelvis (transitional cell Ca.) ; Nephroblastoma ( Wilm ’ s Tumor ). * Clinically may be silent or presented with loin pain, heamaturia and loin mass. * Usually unilateral, rare bilateral. KUB :- * Soft tissue mass. * Bulging in renal out-line. * Diffuse renal enlargement. * Calcification occur in 6 % of cases.
 ; Nephroblastoma ( Wilm ’ s Tumor ). * Clinically may be silent or presented with loin pain, heamaturia and loin mass. * Usually unilateral, rare bilateral. KUB :- * Soft tissue mass. * Bulging in renal out-line. * Diffuse renal enlargement. * Calcification occur in 6 % of cases..")
11
IVU :- IVU :- * Nephrogram shows filling defect which is irregular. * Distracted PCS. * Hydronephrosis. * Amputation & missing calyces. * Large non-functioning kidney. AngiogramUSCTMRI

13
WILM’S Tumor Most common abdominal malignancy in childhood Most common abdominal malignancy in childhood ( 1 – 5 years ), 3% bilateral ( 1 – 5 years ), 3% bilateral KUB & IVU:- Large soft tissue mass displacing bowel loops, distracted calyces,Non functioning kidney Large soft tissue mass displacing bowel loops, distracted calyces,Non functioning kidney
, 3% bilateral ( 1 – 5 years ), 3% bilateral KUB & IVU:- Large soft tissue mass displacing bowel loops, distracted calyces,Non functioning kidney Large soft tissue mass displacing bowel loops, distracted calyces,Non functioning kidney")
15
Epithelial tumor of renal pelvis

16
BLADDER Tumor * Common tumor of urinary tract. * The are of epithelial origin and all are malignant. Radiological appearance :- Filling defect in cystogram stage, well defined or lobulated, plaque like and irregular in non- papillary type. Filling defect in cystogram stage, well defined or lobulated, plaque like and irregular in non- papillary type. Calcification in plain film due to encrusting of urinary salts. Ureteric obstruction

18
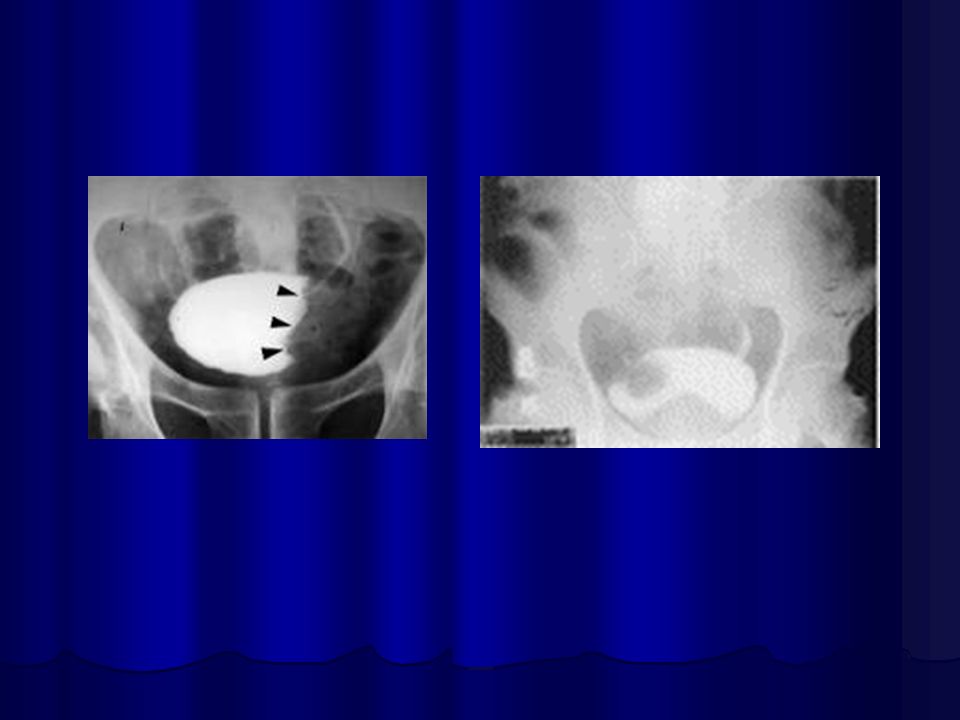
PROSTATIC Enlargement Common cause of lower urinary obstruction. Either Benign prostatic hyperplasia or Carcinoma. Common cause of lower urinary obstruction. Either Benign prostatic hyperplasia or Carcinoma. Benign Hyperplasia :- Plain film:- * Enlargement of bladder shadow due to residual urine. *Prostatic calculi or calcification.

19
IVU ( cystogram stage ) * Elevated bladder base. *Lower ureter elevated and curved (fish hook ). * Back pressure to both kidney & ureters. * Thick trabeculated bladder wall and diverticula formation. * Large size prostate produce filling defect like appearance. * Post-voiding residual volume.

23
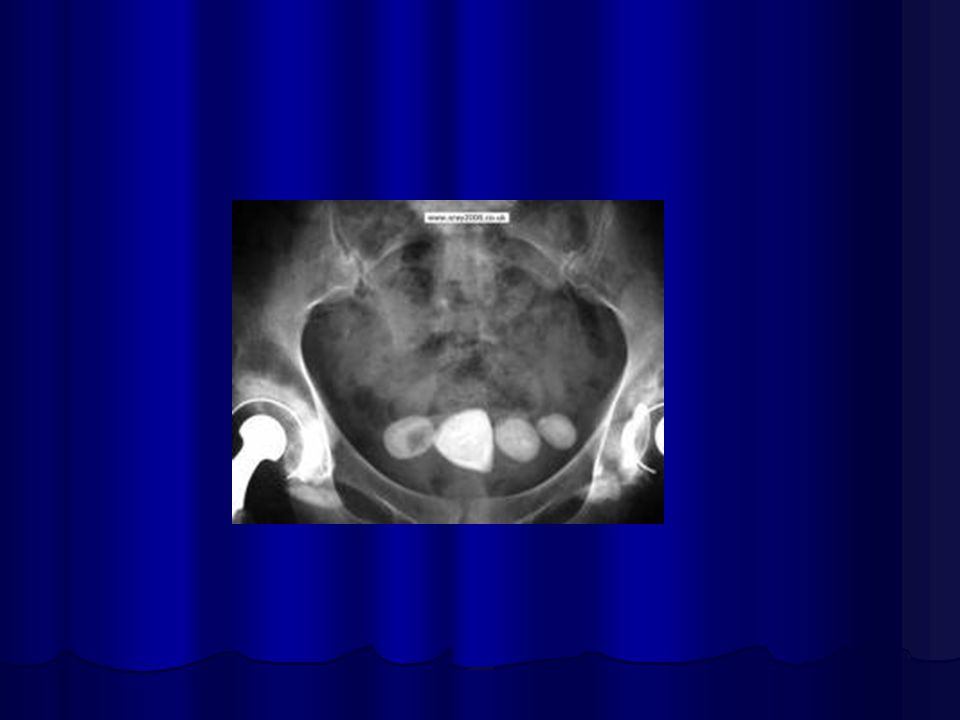
Produce similar changes except: Produce similar changes except: * Plain film shows evidence of metastasis to the bone especially in the pelvis. * The prostatic urethra shows irregular narrowing and stretching. * US can distinguish between BPH & Ca.

24
Bony metastasis

Similar presentations
















: Principal Modality (2): Faculty.>")







