Download presentation
Presentation is loading. Please wait.

1
ABDOMINAL INCISION اعداد الطالب بإشراف الدكتور علي احمد محمد عبيد
اعداد الطالب بإشراف الدكتور علي احمد محمد عبيد بمشاركة سيف ماجد ياسر عليوي رانيا جودي

2
Introduction Incision: A cut produced surgically by a sharp instrument that creates an opening into an organ or space in the body. Abdomen: The part of the trunk that lies between the thorax and the pelvis

3
Considerations in Selecting the Type of Incision
Certainty of diagnosis Speed of entry Body status Presence of previous scars Potential for problems with hemostasis Cosmetic outcome

4
A well-planned incision has FOUR essential elements:
Accessibility: must provide ready access to the expected pathology and adequate exposure. Extensibility: must be extensible if the scope of operation needs to be increased.

5
Preservation of function: should interfere minimally with abdominal wall function muscles must be split in the direction of its fibers rather than cut across; and the incision must Not divide nerves. Security: should heal with adequate strength to reduce the risk of wound disruption and incisional hernia

6
Skin and muscle incisions
Langer’s lines. sken incisions made parallel to Langer's lines may heal better and produce less scarring than those that cut across. Split the muscles in the direction of their fibers, rather than transecting them. Rectus is an exception due to its segmental innervation and presence of tendinous intersection

7
Be careful Any mistake, such as a badly placed incision, worse methods of suturing, or ill-judged selection of suture material, may result in serious complications such as haematoma formation, an ugly scar, an incisional hernia, or, worst of all, complete disruption of the wound

8
Layers of Abdominal Wall
Skin Superficial fascia Deep fascia Muscles Transversalis fascia Extraperitoneal fascia Peritoneum

9
RECTUS ABDOMINIS Origin: Symphysis pubis, pubic crest
Insertion: 5th, 6th and 7th costal cartilage and xiphoid Nerve Supply: Lower six thoracic nerves Rectus Sheath:made up of the aponeuroses of the three Anterolateral abdominal muscles as they converge at the linea alba

10
External Oblique Origin: lower 8 ribs. Insertion: Xiphoid Linea alba
, pubic crest, pubic tubercle, iliac crest. Nerve Supply: Lower six thoracic nerves, iliohypgastric n. , ilioinguinal n.

11
Internal Oblique Origin:Lumbar Fascia,iliac crest,
lateral 2 thirds of inguinal L. Insertion: Lower three ribs, costal cartilage,Xiphoid, Linea alba,symphasis pubis. Nerve Supply:Lower 6 thoracic nerves, iliohypogastric n. , ilioinguinal n.

12
Transversus Abdominis
Origin: lower 6 costal cartilage, lumbar fascia, iliac crest, lateral third of inguinal L. Insertion:Xiphoid process, Linea alba, symphasis pubis. Nerve Supply: Lower 6 thoracic nerves, iliohypgastric n. , ilioinguinal n.

13
Blood Supply 5 intercostals arteries subcostal arteries
4 lumbar arteries Superior epigastric artery, internal thoracic artery Inferior epigastric artery – external iliac artery Deep iliac circumflex artery- external iliac artery.

14
Innervations Intercostal n. T7-12 thoracic n. Iliohypogastric n.
Anterior cutaneous branch Lateral cutaneous branch T7-12 thoracic n. Iliohypogastric n. Ilioinguinal n. Genitofemoral n.

16
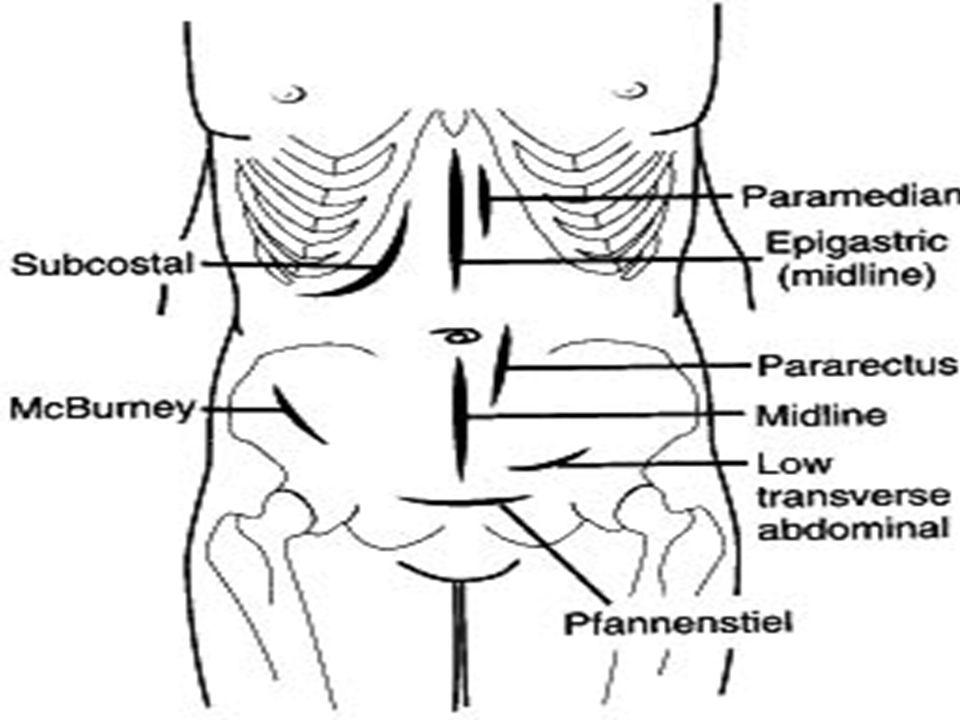
Classification of incisions
Vertical incision : Midline incisions Paramedian incisions Transverse and oblique incisions : Kocher's subcostal Incision Transverse Muscle dividing incision Mc Burney’s grid iron or muscle splitting incision. Oblique Muscle cutting incision Pfannenstiel incision Abdominothoracic incisions.

17
Abdominal Regions

18
Vertical incisions (Midline incisions)
Upper Midline Incision From xiphoid to above umbilicus. Skin superficial and deep fascia linea alba extraperitoneal fat (abundant and vascular) peritoneum. Division of the peritoneum is best performed at the lower end of the incision, just above the umbilicus so that falciform ligament can be seen and avoided Lower Midline Incision From the umbilicus superiorly to the pubic symphysis inferiorly. the peritoneum should be opened in the uppermost area to avoid possible injury to the bladder. Allow access to pelvic organs. Full Midline Incision Great exposure is needed.
 peritoneum. Division of the peritoneum is best performed at the lower end of the incision, just above the umbilicus so that falciform ligament can be seen and avoided. Lower Midline Incision. From the umbilicus superiorly to the pubic symphysis inferiorly. the peritoneum should be opened in the uppermost area to avoid possible injury to the bladder. Allow access to pelvic organs. Full Midline Incision. Great exposure is needed.")
19
Vertical incisions (Midline incisions)
Disadvantages: More painful. Chest complications. Wound infection……Ugly scar…… Incisional hernia…. etc Advantages: It is almost bloodless. No muscle fibers are divided. No nerves are injured. Good access to the upper abdominal viscera. It is very quick to make as well as to close.

20
Paramedian incisions 2 to 5 cm lateral to the midline.
Over the medial aspect of the bulging transverse convexity of the rectus muscle.(linea semilunaris) Extra access can be obtained by sloping the upper extremity of the incision upwards to the xiphoid. (Myo-Robson extension)
 Extra access can be obtained by sloping the upper extremity of the incision upwards to the xiphoid. (Myo-Robson extension)")
21
Paramedian incisions Disadvantages: Advantages:
It doesn’t give good access to contralateral structures. Difficult to extend superiorly as is limited by costal margin. atrophy of the muscle medial to the incision. (due to weakening the lateral blood and nerve supply of the muscle) Advantages: Provide access to the lateral structures such as the spleen or the kidney. Lower incidence of postoperative incisional hernia. (rectus muscle??).
 Advantages: Provide access to the lateral structures such as the spleen or the kidney. Lower incidence of postoperative incisional hernia. (rectus muscle ).")
23
Subcostal Incision (Kocher’s incision)
Incision parallel with right costal margin. (started at the midline, 2 to 5 cm below the xiphoid and extends downwards, outwards and parallel to and about 2.5 cm below the costal margin) It shows excellent exposure to the gall bladder and biliary tract and can be made on the left side to show access to the spleen. Have two modification: Chevron (Roof Top) Modification. The Mercedes Benz Modification.
 It shows excellent exposure to the gall bladder and biliary tract and can be made on the left side to show access to the spleen. Have two modification: Chevron (Roof Top) Modification. The Mercedes Benz Modification.")
24
Chevron (Roof Top) Modification
The incision may be continued across the midline into a double Kocher incision or roof top approach. Access to the upper abdomen. (esp. with broad costal margin) Used for: Total Gastrectomy. Operations for renovascular hypertension. total oesophagectomy. liver transplantation. Extensive hepatic resections. Bilateral adrenalectomy………etc
![]()
25
The Mercedes Benz Modification
consists of bilateral low Kocher’s incision with an upper midline incision up to the xiphisternum. Excellent access to the upper abdominal viscera. (mainly the diaphragmatic hiatuses)
")
26
Disadvantages: It is a muscle cutting incision.
Dividing the 8th and 9th intercostal ns leading to weakness of the ant. abd. wall.

27
(II)-Transverse muscle dividing incision
Its made through rectus sheath and muscle and through the oblique and transversus latrally Its rare to damage more than 1 nerve so post operative abdominal weakness is minimal It gives good exposure Its unnecessary to suture the cut ends of rectus muscles

28
(III)- muscle-splitting McBurney
Oblique skin incision 5 cm above and medial to the anterior superior iliac spine External, internal and transversus muscle are incised or split to incised fascia transversalis and peritoneum No post operative weakness if palpation reveals a mass, the incision can be placed directly over the mass. For most. Appendectomies ,sigmoid colon The Ilioinguinal and Iliohypogastric nerves Inguinal hernia

29
Good healing. Cosmetic appearance

30
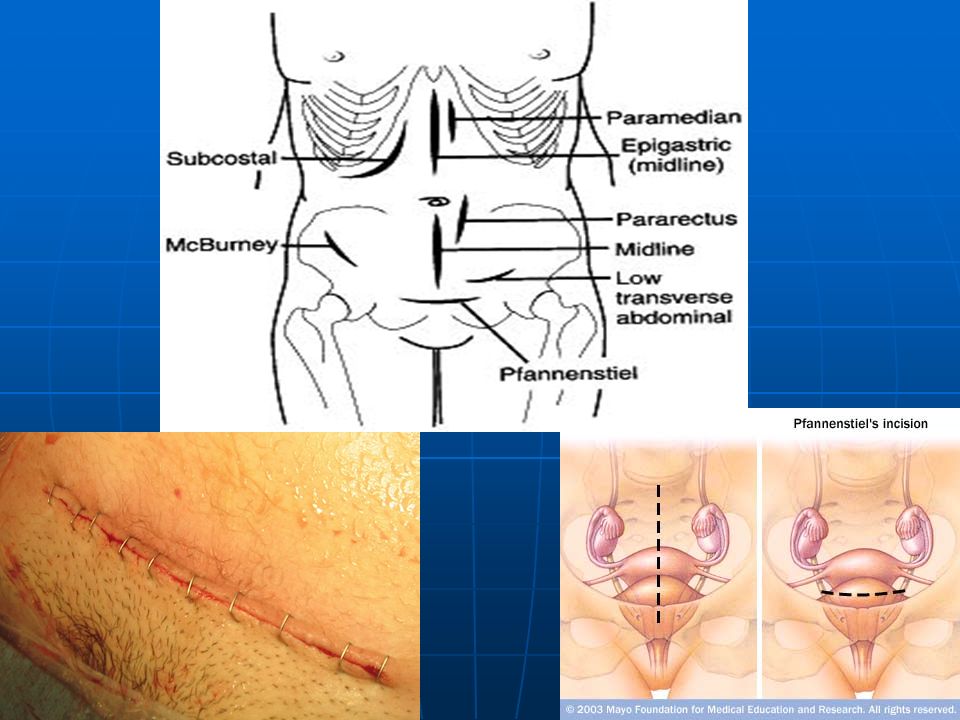
(IV)-Pfannenstiel incision (smile incision)
It is a generally horizontal (slightly curved) line just above the pubic symphysis 5 cm. It is for obstetric delivery and hernia repair bladder, prostate . Advantages: It is a cosmetic incision. It does not distort the umbilicus and heals faster than the traditional vertical incision.
 line just above the pubic symphysis 5 cm. It is for obstetric delivery and hernia repair bladder, prostate . Advantages: It is a cosmetic incision. It does not distort the umbilicus and heals faster than the traditional vertical incision.")
32
Thoracoabdominal Incision
It is done for exposing lower thoracic, upper abdominal & retroperitoneal compartments. It converts the pleural and peritoneal cavities into one common cavity. On the right side, for hepatic resection, on the left side for resection of lower esophagus and upper stomach. It is done through intercostal space 5 through 9 or by resection of ribs 7-9.

33
Disadvantages: Opening the 2 cavities increases the mortality and morbidity rates. Anatomic compilations are encountered, e.g. splenic and phrenic nerve injuries and postoperative pain from transection of costal arch.

35
Thank you

Similar presentations







 in the diaphragm. Give the.>")













