Download presentation
Presentation is loading. Please wait.

2
Physical Examination of the Patient with Pain
DR.BAHMAN ROSHANI

3
Physical Examination of the Patient with Pain
Goals developing the patient’s trust, gaining insight into the impact of pain on the patient’s level of functioning, identifying potential pain generators.

4
Physical Examination of the Patient with Pain
main categories; 1.sensation, 2.motor, 3.reflexes, 4.and coordination

5
Physical Examination of the Patient with Pain
SENSATION AND SENSORY EXAMINATION peripheral nociceptors mechanical nociceptors,( pinch, pinprick), heat nociceptors (temperature greater than 45°C) , polymodal nociceptors,( mechanical, heat, (and chemical noxious stimuli. “fast” or quickly sensed pain, A-ð and C-fibers / Slow pain,
, heat nociceptors (temperature greater than 45°C) , polymodal nociceptors,( mechanical, heat, (and chemical noxious stimuli. fast or quickly sensed pain, A-ð and C-fibers / Slow pain,")
6
Physical Examination of the Patient with Pain
A-d fibers at a rate of( 2 to 30 m/s) sharp,shooting pain C-fibers less than 2 m/s, dull, poorly localized burning pain. .
 sharp,shooting pain. C-fibers less than 2 m/s, dull, poorly localized burning pain. .")
7
Sensory alterations should be described in standardized terms in order to create a more universal record of symptoms. Hyperesthesia Hyperesthesia (hyperalgesia and allodynia). Hyperalgesia is severe pain in response to mild noxious stimuli,. Allodynia is the sensation of pain in response to a non-noxious stimuli (e.g., light touch, fabric on skin). using the contralateral side as a control (when possible). C-fibers painful stimulus warm temperature. A-d pinprick and cold. A-b fibers are examined through light touch, vibration, and joint position
. Hyperalgesia is severe pain in response to mild noxious stimuli,. Allodynia is the sensation of pain in response to a non-noxious stimuli (e.g., light touch, fabric on skin). using the contralateral side as a control (when possible). C-fibers painful stimulus warm temperature. A-d pinprick and cold. A-b fibers are examined through light touch, vibration, and joint position")
8
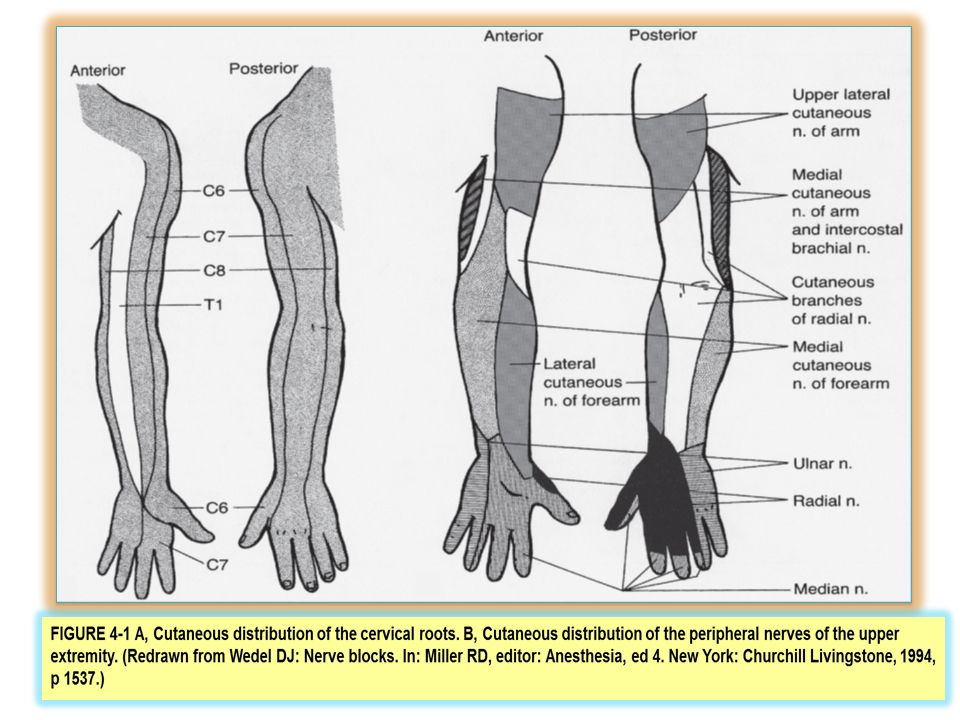
Sensory dissociation loss of fine touch and proprioception pain and temperature sensing are intact. Isolated decreased vibratory sense is an early sign of large-fiber (A-b) neuropathy, and if combined with position sense deficit indicates posterior column disease or peripheral nerve involvement. Posterior column disease (loss of graphesthesia) The inability to perceive isolated joint position is indicative of parietal lobe dysfunction or peripheral nerve lesion.1,2 Anatomically, lesions can be divided into central (brain and spinal cord), spinal nerve root (dermatomal), and peripheral nerve lesions.(Figs. 4-1 and 4-2) differentiate between central and peripheral lesions,(Table 4-1)
 neuropathy, and if combined with. position sense deficit indicates posterior column disease or. peripheral nerve involvement. Posterior column disease (loss of graphesthesia) The inability to perceive isolated joint position is indicative. of parietal lobe dysfunction or peripheral nerve lesion.1,2. Anatomically, lesions can be divided into central (brain and. spinal cord), spinal nerve root (dermatomal), and peripheral. nerve lesions.(Figs. 4-1 and 4-2) differentiate between central. and peripheral lesions,(Table 4-1)")
10
FIGURE 4-2 A, Cutaneous distribution of the lumbosacral nerves
FIGURE 4-2 A, Cutaneous distribution of the lumbosacral nerves. B, Cutaneous distribution of the peripheral nerves of the lower extremity. (Redrawn from Wedel DJ: Nerve blocks. In: Miller RD, editor: Anesthesia, ed 4. New York: Churchill Livingstone,1994, p 1547.)
")
11
TABLE 4–1 Sensory Innervation Landmarks by Dermatome
Dermatome Landmark C4 Shoulder C5 Lateral aspect of the elbow C6 Thumb C7 Middle finger C8 Little finger T1 Medial aspect of the elbow T2 Axilla T3–T11 Corresponding intercostal space T4 Nipple line T10 Umbilicus T12 Inguinal ligament at midline L1 Halfway between T12 and L2 L2 Mid-anterior thigh L3 Medial femoral condyle L4 Medial malleolus L5 Dorsum of foot S1 Lateral heel S2 Popliteal fossa at midline S3 Ischial tuberosity S4–S5 Perianal area

12
MOTOR EXAMINATION Palpation Tone
inspection (hypertrophy, atrophy and fasciculations, among other pathologies) Palpation identify pain generators, Tone Hypotonia, polyneuropathy, myopathy, and certain spinal cord lesions Hypertoni (spasticity and rigidity). Spasticity is commonly seen after brain and spinal cord injury and stroke and in multiple sclerosis. Rigidity, , is characteristic of extrapyramidal diseases, and is due to lesions in the nigrostriatal system.
 Palpation. identify pain generators, Tone. Hypotonia, polyneuropathy, myopathy, and certain spinal cord lesions. Hypertoni (spasticity and rigidity). Spasticity is commonly seen after brain and spinal. cord injury and stroke and in multiple sclerosis. Rigidity, , is characteristic of. extrapyramidal diseases, and is due to lesions in the nigrostriatal. system.")
13
isolated voluntary muscle strength
0 to 5 (normal strength) Greater proximal muscle weakness, indicates myopathy Greater distal muscle weakness,indicates polyneuropathy. Single innervation muscle weakness indicates a peripheral nerve lesion or a radiculopathy
 Greater proximal muscle weakness, indicates myopathy. Greater distal muscle weakness,indicates polyneuropathy. Single innervation muscle weakness indicates a peripheral nerve lesion. or a radiculopathy.")
14
TABLE 4–2 Standard Muscle Grading System
Grade Description No movement Trace movement, no joint movement Full range of motion with gravity eliminated Full range of motion against gravity Full range of motion against gravity and partial resistance 5 (normal) Full range of motion against gravity and full
 Full range of motion against gravity and full.")
15
REFLEXES AND COORDINATION
valuable guide to the anatomic localization of a lesion (Table 4-3.) Jendrassik’s maneuver Clonus may be indicative of an upper motor neuron disease. Plantar reflex testing. Babinski’s sign can be seen with many upper motor neuron diseases, and is also normal variant in children up until 12 to 18 months Hoffman’s sign indicative of an upper motor neuron disease. Coordination and gait testing Cerebellar function (finger-nose-finger and heel-knee-shin test.) Equilibrium observation of normal gait, heel-and-toe walk, and tandem gait testing (heel- totoe walking in a straight line). Romberg’s test (suggestive of mild lesions of the sensory, vestibular, or proprioceptive systems.)
 Jendrassik’s maneuver. Clonus may be indicative of an upper motor neuron disease. Plantar reflex testing. Babinski’s sign can be seen with many upper motor neuron diseases, and is also normal variant in children up until 12 to 18 months. Hoffman’s sign indicative of an upper motor neuron disease. Coordination and gait testing. Cerebellar function (finger-nose-finger and heel-knee-shin test.) Equilibrium. observation of normal gait, heel-and-toe walk, and tandem gait testing (heel- totoe walking in a straight line). Romberg’s test (suggestive of mild lesions of the sensory, vestibular, or. proprioceptive systems.)")
16
TABLE 4–3 Root Level Tested for Common Reflexes
Nerve Root Level Reflex S1–S2 Achilles reflex L3–L4 Patellar reflex C5–C6 Biceps reflex C7–C8 Triceps reflexve

17
TABLE 4–4 Deep-Tendon Reflex Grading System
Grade Description 0 No response 1+ Reduced, less than expected 2+ Normal 3+ Greater than expected, moderately hyperactive 4+ Hyperactive with clonus

18
DIRECTED PAIN EXAMINATION TEMPLATE
The goal is to develop a standardized and consistent examination. A standard template should include inspection, palpation, percussion, range of motion, motor examination, sensory examination, reflexes, and additional regional provocative tests if indicated. (Table 4-5) Inspection infection or rash, surgical or traumatic scars, sudomotor alterations, cutaneous discoloration, and abnormal hair growth edema and muscular atrophy or hypertrophy and masses cutaneous temperature should be measured sympathetically mediated pain.
 Inspection. infection or rash, surgical or traumatic scars, sudomotor alterations, cutaneous. discoloration, and abnormal hair growth. edema and muscular atrophy or hypertrophy and masses. cutaneous temperature should be measured. sympathetically mediated pain.")
19
TABLE 4–5 Directed Pain Examination Template
Examination Observation Inspection …………… Cutaneous landmarks, symmetry, temperature Palpation … Gross sensory changes, masses, trigger points, pulses Percussion …………………. Tinel’s sign, fractures Range of Motor …………….. Described in degrees, reason for motion limitation Innervation Graded 0–5, correlated with examination Sensory Reflexes ……………. Dermatomal distribution of changes, examination description of affected fibers, Graded 0–4 Provocative ………………… Description of concordant vs. tests disconcordant pain, appropriate for region

20
Palpation percussion Range of motion (ROM) Lymph nodes,
trigger points, lipomas Tenderness contralateral structure palpated percussion Pain on percussion of bony structures can indicate a fracture, abscess, or infection Pain on percussion over a sensory nerve, or Tinel’s sign(carpal tunnel syndrome occipital neuralgia) Range of motion (ROM) Joint, connective tissue, or ligamentous laxity can result in supranormal ROM, whereas pain and structural abnormalities (strictures, arthritis) can limit ROM.
 Range of motion (ROM) Joint, connective tissue, or ligamentous laxity can. result in supranormal ROM, whereas pain and structural. abnormalities (strictures, arthritis) can limit ROM.")
21
GENERAL OBSERVATIONS Observations mannerisms, coordination, interpersonal interactions, and gait obtaining vital signs MENTAL STATUS EXAMINATION (table 4-6) GAIT normal, antalgic, or abnormal
 GAIT. normal, antalgic, or abnormal.")
22
TABLE 4–6 Brief Mental Examination
Orientation to person and place, date .repetition Ability to name objects (e.g., pen, watch) Memory immediate at 1 min, and at 5 min; repeat the names of three objects Ability to calculate serial 7s, or if patient refuses have them spell “world” backward Signs of cognitive deficits, aphasia
 Memory immediate at 1 min, and at 5 min; repeat the names of three objects Ability to calculate serial 7s, or if patient refuses have them spell world backward Signs of cognitive deficits, aphasia")
23
EXAMINATION OF THE DIFFERENT REGIONS OF THE BODY
face, cervical region, thoracic region, lumbosacral region. FACE Inspection infection, herpetic lesions, sudomotor changes, and scarring (both traumatic and postherpetic). Oral inspection symmetry of the face; Facial palpation masses, sensory changes, and tenderness over the sinuses. Percussion (Chvostek’s test) (TMJ)
. Oral inspection. symmetry of the face; Facial palpation. masses, sensory changes, and tenderness. over the sinuses. Percussion (Chvostek’s test) (TMJ)")
24
Test Function Cranial Nerve
TABLE 4–7 Cranial Nerve Examination: Summary of Cranial Nerve Functions and Tests Test Function Cranial Nerve Use coffee, mint, and so on held to each nostril separately; consider basal frontal tumor in unilateral dysfunction Smell I. Olfactory Assess optic disc, visual acuity; name number of fingers in central and peripheral quadrants; direct and consensual pupil reflex; note Marcus-Gunn pupil (paradoxically dilating pupil) Vision II. Optic Pupil size; visually track objects in eight cardinal directions; note Horner’s pupil (miosis, ptosis, anhydrosis) Extraocular muscles III, IV, and VI. (Oculomotor, trochlear, and (abducen Cotton-tipped swab/pinprick to all three branches; recall bilateral forehead innervation (peripheral lesion spares forehead, central lesion affects forehead); note atrophy, jaw deviation to side of lesion Facial sensation, muscles of mastication V. Trigeminal: motor and sensory
 Vision. II. Optic. Pupil size; visually track objects in eight cardinal directions; note Horner’s pupil (miosis, ptosis, anhydrosis) Extraocular muscles. III, IV, and VI. (Oculomotor, trochlear, and (abducen. Cotton-tipped swab/pinprick to all three branches; recall bilateral forehead innervation (peripheral lesion spares forehead, central lesion affects forehead); note atrophy, jaw deviation to side of lesion. Facial sensation, muscles of mastication. V. Trigeminal: motor and. sensory.")
25
Test Function Cranial Nerve (acoustic)
TABLE 4–7 Cranial Nerve Examination: Summary of Cranial Nerve Functions and Tests Test Function Cranial Nerve Wrinkle forehead, close eyes tightly, smile, purse lips, puff cheeks; corneal reflex Muscles of facial expression VII. Facial Use timing fork, compare side to side; Rinne’s test for air conduction (AC) vs. bone conduction (BC) (BC . AC); Weber’s test for sensorineural hearing Hearing, equilibrium VIII. Vestibulocochlear (acoustic) Palate elevates away from the lesion; check gag reflex Palate elevation; taste to posterior third of tongue; sensation to posterior tongue, pharynx, middle ear, and dura IX. Glossopharyngeal Check for vocal cord paralysis, hoarse or nasal voice Muscles of pharynx, larynx X. Vagus Shoulder shrug, sternocleidomastoid strength Muscles of larynx, sternocleidomastoid,trapezius XI. Accessory Protrusion of tongue; deviates toward lesion Intrinsic tongue muscles XII. Hypoglossal
 vs. bone conduction (BC) (BC . AC); Weber’s test for sensorineural hearing. Hearing, equilibrium. VIII. Vestibulocochlear. (acoustic) Palate elevates away from the lesion; check gag reflex. Palate elevation; taste to posterior third of tongue; sensation to posterior tongue, pharynx, middle ear, and dura. IX. Glossopharyngeal. Check for vocal cord paralysis, hoarse or nasal voice. Muscles of pharynx, larynx. X. Vagus. Shoulder shrug, sternocleidomastoid strength. Muscles of larynx, sternocleidomastoid,trapezius. XI. Accessory. Protrusion of tongue; deviates toward lesion. Intrinsic tongue muscles. XII. Hypoglossal.")
26
symmetry, muscle condition, and the position of the head, shoulder,
CERVICAL AND THORACIC REGIONS AND UPPER EXTREMITIES symmetry, muscle condition, and the position of the head, shoulder, and upper extremity at rest. upper extremities for sudomotor changes Palpation can identify muscle spasms, myofascial trigger points, enlarged lymph nodes, occipital nerve entrapment, and pain over the bony posterior spine The normal cervical ROMs are flexion, 0 to 60°; extension, 0 to 25°; bilateral lateral flexion, 0 to 25°; and bilateral lateral rotation, 0 to 80°. TABLE 4-8

27
TABLE 4–8 / Cervical Region Nerve Root Testing
Reflex Sensory Action Position Muscle(s) Tested Nerve Level Root None Shoulders Shoulder shrug Sitting Levator scapulae Dorsal scapular C4 Biceps Lateral forearm, first and second finger Patient attempts further flexion against resistance Forearm fully supinated, elbow flexed 90° Musculocutaneous lateral arm (C5–6) C5 Brachioradialis Middle finger Maintain extension Elbow flexed at 45°, wrist extended Extensor carpi, radialis, longus, and brevis Radial (C5–6) C6 Triceps Extend forearm against gravity Shoulder slightly abducted, elbow slightly flexed Radial (C6–8) C7 Fourth, fifth finger medial forearm Finger flexion of middle finger Flexor digitorum profundus Anterior interosseous (median) (C7–8) C8 Medial arm Examiner pushes patient’s fingers together, patient resists Patient extends and spreads all fingers Dorsal interossei Ulnar, deep branch (C8–T1) T1
 Tested. Nerve. Level. Root. None. Shoulders. Shoulder shrug. Sitting. Levator scapulae. Dorsal scapular. C4. Biceps. Lateral forearm, first and second. finger. Patient attempts. further flexion. against resistance. Forearm fully. supinated, elbow. flexed 90° Musculocutaneous. lateral arm (C5–6) C5. Brachioradialis. Middle finger. Maintain extension. Elbow flexed at. 45°, wrist extended. Extensor carpi, radialis, longus, and brevis. Radial (C5–6) C6. Triceps. Extend forearm. against gravity. Shoulder slightly. abducted, elbow. slightly flexed. Radial (C6–8) C7. Fourth, fifth finger medial forearm. Finger flexion of. middle finger. Flexor digitorum. profundus. Anterior interosseous. (median) (C7–8) C8. Medial arm. Examiner pushes. patient’s fingers. together, patient. resists. Patient extends and. spreads all fingers. Dorsal interossei. Ulnar, deep branch. (C8–T1) T1.")
28
Provocative Tests distraction test cervical compression test
Spurling’s (neck compression) Valsalva maneuver drop-arm test shoulder ROM testing Yergason test (biceps tendon) tennis elbow test.( lateral epicondylitis) ulnar Tinel’s sign median nerve Tinel’s sign Phalen’s sign
 Valsalva maneuver. drop-arm test. shoulder ROM testing. Yergason test (biceps tendon) tennis elbow test.( lateral epicondylitis) ulnar Tinel’s sign. median nerve Tinel’s sign. Phalen’s sign.")
29
THORACIC REGION Thoracic spine pathology can result in pain in the thorax, abdomen, and back. Inspection should focus on cutaneous landmarks and the presence of herpetic lesions, ecchymotic lesions, or masses. thoracic spine, rib cage, and sternum kyphosis or scoliosis Thoracic palpation abdominal aortic aneurysm There are no true ROM, motor, or reflex examinations truly specific to the thoracic region

30
LUMBOSACRAL REGION is the most common location of pain most potential pain-generating structures. inspection of the patient’s gait and posture degree of spinal curvature. postsurgical scars Lower extremity inspection Common bony structure pain generators include the facet joints, sacroiliac joints, and the coccyx. The normal lumbar spine ROMs are flexion, 0 to 90°; extension, 0 to 30°; bilateral lateral flexion, 0 to 25° ; and bilateral lateral rotation, 0 to 60°. pain on flexion hints at a possible disc lesion, whereas pain on extension can indicate a facet arthropathy or myofascial pain generator. two complementary tests are heel walk (dorsiflexion), which tests L4–L5 function, and toe walk (plantar flexion), which tests S1–S2 integrity The majority of tests are directed toward pathology in the disc and nerve roots,
, which tests L4–L5 function, and toe walk (plantar flexion), which tests S1–S2 integrity. The majority of tests. are directed toward pathology in the disc and nerve roots,")
31
TABLE 4–9 Lumbar Region Nerve Root Testing
Reflex Sensory Action Position Muscle(s) Tested Nerve BOT LEV Patellar Anterior upper thigh Hip and knee, upper thigh flexed at 90° Hip and knee flexed at 90° Psoas, iliacus Femoral (L2–L4) L2 Anterior lower Extend knee against resistance Supine, hip flexed, knee flexed at 90° Quadriceps femoris L3 Knee walk Maintain extension against resistance Ankle dorsiflexed, peroneal anterior heel walk Tibialis Deep anterior (L4–L5) L4 Medial hamstring Web between big and second toe Dorsum of foot Great toe extended Foot everted Extensor hallucis longus Deep lateral calf, peroneal hamstring Superficial peroneal L5 Achilles Foot (except medial aspect) Maintain flexion Prone, knee flexed toe walk Hamstrings Sciatic (L5–S2) S1
 Tested. Nerve. BOT LEV. Patellar. Anterior upper. thigh. Hip and knee, upper. thigh flexed at 90° Hip and knee. flexed at 90° Psoas, iliacus. Femoral (L2–L4) L2. Anterior lower. Extend knee against. resistance. Supine, hip flexed, knee flexed at 90° Quadriceps femoris. L3. Knee walk. Maintain extension. against resistance. Ankle dorsiflexed, peroneal anterior. heel walk. Tibialis. Deep anterior. (L4–L5) L4. Medial. hamstring. Web between big. and second toe. Dorsum of foot. Great toe extended. Foot everted. Extensor hallucis. longus. Deep lateral calf, peroneal hamstring. Superficial peroneal. L5. Achilles. Foot (except. medial aspect) Maintain flexion. Prone, knee flexed. toe walk. Hamstrings. Sciatic (L5–S2) S1.")
32
joints, sacroiliac joint, hip, and piriformis muscle.
straight leg raise slumped-seat test Patrick Faber test, Gaenslen’s test, Yeoman’s test, posterior shear test are tests for sacroiliac joint dysfunction General tests for intrathecal lesions (Kernig test, the Valsalva, Milgram test) The Hoover test confirm the presence of malingering paralysis of the legs Waddell’s signs (non organic) The five signs or tests are tenderness, simulation testing, distraction testing, regional disturbances, and overreaction.
 The Hoover test confirm the presence of malingering paralysis of the legs. Waddell’s signs (non organic) The five signs or. tests are tenderness, simulation testing, distraction testing, regional disturbances, and overreaction.")
33
CONCLUSION The physical examination is secondary in importance only to the pain history. Costly imaging studies and painful invasive testing can be avoided by performing a simple yet thorough physical exam. Following a brief global assessment of the patient’s health, the pain examination should be focused toward the affected region and consistently performed in a structured pattern using templates and standard “normal” charts and maps. physical examination that fulfills these criteria is an invaluable component in establishing the correct diagnosis in a pain patient.

Similar presentations











 Cranial nerve function Motor function Sensory function Cerebellar function Reflex.>")

 and passes through foramina of skull There are 12 pairs of cranial nerves They have both name.>")






