Download presentation
Presentation is loading. Please wait.

1
Communicable Diseases and Human Security
Kelechi Ohiri MD MPH MS Health, Nutrition, Population Human Development Network World Bank Review the choice of the title

2
Outline of Presentation
Part 1 – Overview of Communicable Diseases (CDs) Introduction and Definition Importance of CDs Selected CDs of Public Health Concern Part 2- Mounting a Global Response Approaches to intervention Key elements of a global response World Bank’s role and involvement Introduction and Definition Definition: Modes of transmission Examples of CDs Common Infectious diseases Neglected diseases History of Communicable Diseases Burden of Disease Global burden of disease and communicable diseases, by region, gender and income levels Importance of CDs Sheer Burden Economic impact Rate of spread Recurrence of diseases Security and CDs Interventions Why intervene? Why should policy makers care about CDs? History of interventions and policy issues What is needed for effective control of CDs Global Approaches Global responsibility International law Partnerships and collaboration Financial support World Bank’s role and involvement Total lending in health Special programs the Bank is involved in. Conclusions and Way forward
 Introduction and Definition. Importance of CDs. Selected CDs of Public Health Concern. Part 2- Mounting a Global Response. Approaches to intervention. Key elements of a global response. World Bank’s role and involvement. Introduction and Definition. Definition: Modes of transmission. Examples of CDs. Common Infectious diseases. Neglected diseases. History of Communicable Diseases. Burden of Disease. Global burden of disease and communicable diseases, by region, gender and income levels. Importance of CDs. Sheer Burden. Economic impact. Rate of spread. Recurrence of diseases. Security and CDs. Interventions. Why intervene Why should policy makers care about CDs History of interventions and policy issues. What is needed for effective control of CDs. Global Approaches. Global responsibility. International law. Partnerships and collaboration. Financial support. World Bank’s role and involvement. Total lending in health. Special programs the Bank is involved in. Conclusions and Way forward.")
3
Human Security in a globalized world
The changing role of policy makers in an increasingly globalized world Shared space = Shared Destiny Local actions have global consequences Global interventions can achieve positive local impact As long as human interactions exist, Communicable diseases will remain an issue.

4
Communicable Diseases: Definition
Defined as “any condition which is transmitted directly or indirectly to a person from an infected person or animal through the agency of an intermediate animal, host, or vector, or through the inanimate environment”. Transmission is facilitated by the following (IOM) more frequent human contact due to Increase in the volume and means of transportation (affordable international air travel), globalization (increased trade and contact) Microbial adaptation and change Breakdown of public health capacity at various levels Change in human demographics and behavior Economic development and land use patterns These have become more important given the modern means of transportation and increased interaction across countries that makes it easy for an infectious pathogen to spread from one part of the world to another
 more frequent human contact due to. Increase in the volume and means of transportation (affordable international air travel), globalization (increased trade and contact) Microbial adaptation and change. Breakdown of public health capacity at various levels. Change in human demographics and behavior. Economic development and land use patterns. These have become more important given the modern means of transportation and increased interaction across countries that makes it easy for an infectious pathogen to spread from one part of the world to another.")
5
CD- Modes of transmission
Direct Blood-borne or sexual – HIV, Hepatitis B,C Inhalation – Tuberculosis, influenza, anthrax Food-borne – E.coli, Salmonella, Contaminated water- Cholera, rotavirus, Hepatitis A Indirect Vector-borne- malaria, onchocerciasis, trypanosomiasis Formites Zoonotic diseases – animal handling and feeding practices (Mad cow disease, Avian Influenza)
")
6
Importance of Communicable Diseases
Significant burden of disease especially in low and middle income countries Social impact Economic impact Potential for rapid spread Human security concerns Intentional use

7
Communicable Diseases account for a significant global disease burden
In 2005, CDs accounted for about 30% of the global BoD and 60% of the BoD in Africa. CDs typically affect LIC and MICs disproportionately. Account for 40% of the disease burden in low and middle income countries Most communicable diseases are preventable or treatable. Even with the projected rise in the burden of NCDs, CDs are expected to account for 26% of the BoD in 2015 globally, and 56% in Africa. (Global Burden of Disease

8
Communicable Disease Burden Varies Widely Among Continents

9
Communicable disease burden in Europe

10
Causes of Death Vary Greatly by Country Income Level
In Sierra Leone most deaths occur in the U5 age group, whereas in Denmark it is among those over 65.

11
CDs have a significant social impact
Disruption of family and social networks Child-headed households, social exclusion Widespread stigma and discrimination TB, HIV/AIDS, Leprosy Discrimination in employment, schools, migration policies Orphans and vulnerable children Loss of primary care givers Susceptibility to exploitation and trafficking Interventions such as quarantine measures may aggravate the social disruption Global importance of Communicable Diseases Enormous burden and impact globally Economic impact Constrain health and development of infants and children and affect their schooling Stigma and discrimination against people with certain communicable diseases such as HIV/AIDS, TB. Leprosy Disruption of social networks and family structure e.g. with Orphans and other vulnerable children who have lost their parents or other care gives due to HIV/AIDS TB- Malaria HIV/AIDS etc

12
CDs have a significant economic impact in affected countries
At the macro level Reduction in revenue for the country (e.g. tourism) Estimated cost of SARS epidemic to Asian countries: $20 billion (2003) or $2 million per case. Drop in international travel to affected countries by 50-70% Malaria causes an average loss of 1.3% annual GDP in countries with intense transmission The plague outbreak in India cost the economy over $1 billion from travel restrictions and embargoes At the household level Poorer households are disproportionately affected Substantial loss in productivity and income for the infirmed and caregiver Catastrophic costs of treating illness Reduction in revenue for the country India example during the bubonic plague outbreak Substantial loss in productivity and income In Tanzania, men with AIDS lost an average of 197 days of work over an 18 month period. Catastrophic costs of treating illness
 Estimated cost of SARS epidemic to Asian countries: $20 billion (2003) or $2 million per case. Drop in international travel to affected countries by 50-70% Malaria causes an average loss of 1.3% annual GDP in countries with intense transmission. The plague outbreak in India cost the economy over $1 billion from travel restrictions and embargoes. At the household level. Poorer households are disproportionately affected. Substantial loss in productivity and income for the infirmed and caregiver. Catastrophic costs of treating illness. Reduction in revenue for the country. India example during the bubonic plague outbreak. Substantial loss in productivity and income. In Tanzania, men with AIDS lost an average of 197 days of work over an 18 month period. Catastrophic costs of treating illness.")
13
International boundaries are disappearing
Borders are not very effective at stopping communicable diseases. With increasing globalization interdependence of countries – more trade and human/animal interactions The rise in international traffic and commerce makes challenges even more daunting Other global issues affect or are affected by communicable diseases. climate change migration Change in biodiversity In history, attempts at stopping communicable diseases from entering a country often proved ineffective

14
Human Security concerns
Potential magnitude and rapid spread of outbreaks/pandemics. e.g. SARS outbreak No country or region can contain a full blown outbreak of Avian influenza Bioterrorism and intentional outbreaks Anthrax, Small pox New and re-emerging diseases Ebola, TB (MDR-TB and XDR-TB), HPAI, Rift valley fever.
, HPAI, Rift valley fever.")
15
Select Communicable Diseases

16
Tuberculosis 2 billion people infected with microbes that cause TB.
Not everyone develops active disease A person is infected every second globally 22 countries account for 80% of TB cases. >50% cases in Asia, 28% in Africa (which also has the highest per capita prevalence) In 2005, there were 8.8 million new TB cases; 1.6 million deaths from TB (about 4400 a day) Highly stigmatizing disease Two billion people – one third of the world’s total population–are infected with the microbes that cause TB. Of these, 10% will become sick with active TB in their lifetime. Risks are higher in those with HIV infection. A total of 1.6 million people died from TB in 2005, equal to about 4400 deaths a day. TB is a disease of poverty, affecting mostly young adults in their most productive years. The vast majority of TB deaths are in the developing world, with more than half occurring in Asia TB/HIV- About people with HIV die from TB every year, most of them in Africa. TB is a worldwide pandemic. Although the highest rates per capita are in Africa (28% of all TB cases), half of all new cases are in six Asian countries (Bangladesh, China, India, Indonesia, Pakistan and the Philippines). Multidrug-resistant TB (MDR-TB) is a form of TB that does not respond to the standard treatments using first-line drugs. MDR-TB is present in virtually all countries recently surveyed by WHO and its partners. About new MDR-TB cases are estimated to occur every year. The highest occurrence rates of MDR-TB are in China and the countries of the former Soviet Union. Extensively drug-resistant TB (XDR-TB) occurs when resistance to second-line drugs develops. It is extremely difficult to treat and cases have been confirmed in South Africa and worldwide. WHO’s Stop TB Strategy aims to reach all patients and achieve the target under the Millennium Development Goals (MDG): to reduce by 2015 the prevalence of and deaths due to TB by 50% relative to 1990 and reverse the trend in incidence. The Global Plan to Stop TB , launched January 2006, aims to achieve the MDG target with an investment of US$ 56 billion. This represents a three-fold increase in investment from The estimated funding gap is US$ 31 billion.
 In 2005, there were 8.8 million new TB cases; 1.6 million deaths from TB (about 4400 a day) Highly stigmatizing disease. Two billion people – one third of the world’s total population–are infected with the microbes that cause TB. Of these, 10% will become sick with active TB in their lifetime. Risks are higher in those with HIV infection. A total of 1.6 million people died from TB in 2005, equal to about 4400 deaths a day. TB is a disease of poverty, affecting mostly young adults in their most productive years. The vast majority of TB deaths are in the developing world, with more than half occurring in Asia. TB/HIV- About people with HIV die from TB every year, most of them in Africa. TB is a worldwide pandemic. Although the highest rates per capita are in Africa (28% of all TB cases), half of all new cases are in six Asian countries (Bangladesh, China, India, Indonesia, Pakistan and the Philippines). Multidrug-resistant TB (MDR-TB) is a form of TB that does not respond to the standard treatments using first-line drugs. MDR-TB is present in virtually all countries recently surveyed by WHO and its partners. About new MDR-TB cases are estimated to occur every year. The highest occurrence rates of MDR-TB are in China and the countries of the former Soviet Union. Extensively drug-resistant TB (XDR-TB) occurs when resistance to second-line drugs develops. It is extremely difficult to treat and cases have been confirmed in South Africa and worldwide. WHO’s Stop TB Strategy aims to reach all patients and achieve the target under the Millennium Development Goals (MDG): to reduce by 2015 the prevalence of and deaths due to TB by 50% relative to 1990 and reverse the trend in incidence. The Global Plan to Stop TB , launched January 2006, aims to achieve the MDG target with an investment of US$ 56 billion. This represents a three-fold increase in investment from The estimated funding gap is US$ 31 billion.")
17
Tuberculosis and HIV A third of those living with HIV are co-infected with TB About 200,000 people with HIV die annually from TB. Most common opportunistic infection in Africa 70% of TB patients are co-infected with HIV in some countries in Africa Impact of HIV on TB TB is harder to diagnose in HIV-positive people. TB progresses faster in HIV-infected people. TB in HIV-positive people is almost certain to be fatal if undiagnosed or left untreated. TB occurs earlier in the course of HIV infection than many other opportunistic infections. Most cases of XDR-TB were in HIV infected individuals.

18
Global Prevalence of TB cases (WHO)
")
19
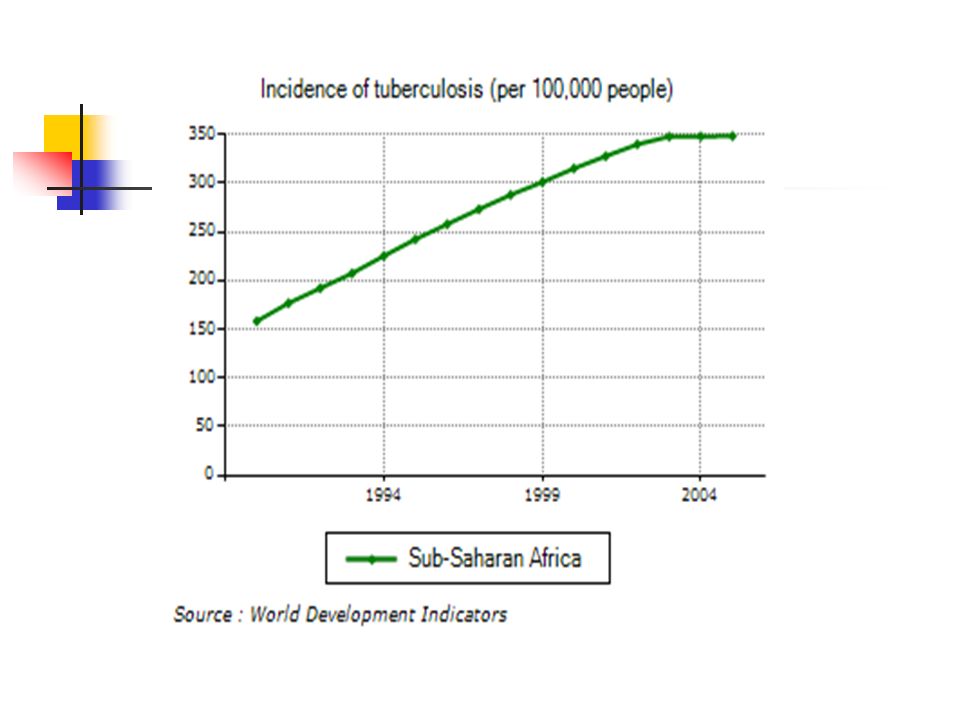
Tuberculosis

21
Tuberculosis Control Challenges for tuberculosis control
MDR-TB - In most countries. About new cases annually. XDR-TB cases confirmed in South Africa. Weak health systems TB and HIV The Global Plan to Stop TB an investment of US$ 56 billion, a three-fold increase from The estimated funding gap is US$ 31 billion. Six step strategy: Expanding DOTS treatment; Health Systems Strengthening; Engaging all care providers; Empowering patients and communities; Addressing MDR TB, Supporting research

22
Malaria Every year, 500 million people become severely ill with malaria causes 30% of Low birth weight in newborns Globally. >1 million people die of malaria every year. One child dies from it every 30 seconds 40% of the world’s population is at risk of malaria. Most cases and deaths occur in SSA. Malaria is the 9th leading cause of death in LICs and MICs 11% of childhood deaths worldwide attributable to malaria SSA children account for 82% of malaria deaths worldwide More than one million people die of malaria every year, mostly infants, young children and pregnant women and most of them in Africa Approximately, 40% of the world’s population, mostly those living in the world’s poorest countries, are at risk of malaria. Every year, more than 500 million people become severely ill with malaria. Most cases and deaths are in sub-Saharan Africa.

23
Annual Reported Malaria Cases by Country (WHO 2003)
")
24
Global malaria prevalence

25
Malaria Control Malaria control Challenges in malaria control
Early diagnosis and prompt treatment to cure patients and reduce parasite reservoir Vector control: Indoor residual spraying Long lasting Insecticide treated bed nets Intermittent preventive treatment of pregnant women Challenges in malaria control Widespread resistance to conventional anti-malaria drugs Malaria and HIV Health Systems Constraints Access to services Coverage of prevention interventions With full LLITN coverage, child mortality from all causes is reduced by 18%

26
HIV/AIDS In 2005, 38.6 million people worldwide were living with HIV, of which 24.7 million (two-thirds) lived in SSA 4.1 million people worldwide became newly infected 2.8 million people lost their lives to AIDS New infections occur predominantly among the age group. Previously unknown about 25 years ago. Has affected over 60 million people so far. One of the most devastating conditions of the 21st century An estimated 38.6 million [33.4 million–46.0 million] people worldwide were living with HIV in An estimated 4.1 million [3.4 million–6.2 million] became newly infected with HIV and an estimated 2.8 million [2.4 million–3.3 million] lost their lives to AIDS.

27
HIV Co-infections Impact of TB on HIV HIV and Malaria
TB considerably shortens the survival of people with HIV/AIDS. TB kills up to half of all AIDS patients worldwide. TB bacteria accelerate the progress of AIDS infection in the patient HIV and Malaria Diseases of poverty HIV infected adults are at risk of developing severe malaria Acute malaria episodes temporarily increase HIV viral load Adults with low CD4 count more susceptible to treatment failure Growing body of evidence on the interactions between both conditions Both are diseases of poverty

28
Global HIV Burden

29
HIV/AIDS Interventions depend on Elements of an effective intervention
Epidemiology – mode of transmission, age group Stage of epidemic –concentrated vs. generalized Elements of an effective intervention Strong political support and enabling environment. Linking prevention to care and access to care and treatment Integrate it into poverty reduction and address gender inequality Effective monitoring and evaluation Strengthening the health system and Multisectoral approaches Challenges in prevention and scaling up treatment globally include Constraints to access to care and treatment Stigma and discrimination Inadequate prevention measures. Co-infections (TB, Malaria)
")
30
Avian Influenza Seasonal influenza causes severe illness in 3-5 million people and – deaths yearly 1st H5N1 avian influenza case in Hong Kong in 1997. By October 2007 – 331 human cases, 202 deaths.

31
Avian Influenza Control depends on the phase of the epidemic
Pre-Pandemic Phase Reduce opportunity for human infection Strengthen early warning system Emergence of Pandemic virus Contain and/or delay the spread at source Pandemic Declared Reduce mortality, morbidity and social disruption Conduct research to guide response measures Antiviral medications – Oseltamivir, Amantadine Vaccine – still experimental under development. Can only be produced in significant quantity after an outbreak Limited evidence suggests that some antiviral drugs, notably oseltamivir (commercially known as Tamiflu), can reduce the duration of viral replication and improve prospects of survival, provided they are administered within 48 hours following symptom onset.
, can reduce the duration of viral replication and improve prospects of survival, provided they are administered within 48 hours following symptom onset.")
32
Confirmed human cases of HPAI

33
Migratory pathway for birds and Avian influenza

34
Neglected diseases Cause over 500,000 deaths and 57 million DALYs annually. Include the following Helminthic infections Hookworm (Ascaris, trichuris), lymphatic filariasis, onchocerciasis, schistosomiasis, dracunculiasis Protozoan infections Leishmaniasis, African trypanosomiasis, Chagas disease Bacterial infections Leprosy, trachoma, buruli ulcer
, lymphatic filariasis, onchocerciasis, schistosomiasis, dracunculiasis. Protozoan infections. Leishmaniasis, African trypanosomiasis, Chagas disease. Bacterial infections. Leprosy, trachoma, buruli ulcer.")
35
Communicable Disease and Human Security
Part 2 - Mounting an Effective Global Response

36
Approaches to Interventions
Personal Responsibility and action Utilitarian Approaches – “Greatest good for the greatest number” Including non Health Systems Interventions. Regulations and Laws Partnerships and Collaboration Enlightened Self Interest

37
Personal Responsibility and action
Improved hygiene and sanitation Hand washing, proper waste disposal, food preparation and handling. Information, education and behavior change Changing harmful household practices Livestock handling, knowledge about contagion Cultural and social norms Self reporting of illnesses and compliance with interventions and treatment. Improved hygiene and sanitation Hand washing, proper waste disposal, sewage system, cooking methods and boiling water Information, education and behavior change including household practices Livestock handling, knowledge about contagion, Cultural norms Poultry and farming methods, ….. Self reporting of illnesses and compliance with interventions and treatment Unexplained fevers, ARI symptoms, etc Compliance with medications to reduce potential for drug resistance. – hasn’t always worked - DOTS

38
Utilitarian Approaches – “Greatest good for the greatest number”
Reliance on personal responsibility not always the optimal option given different knowledge levels and values. Public good nature of the interventions Social Isolation and Quarantine measures Home treatment; Isolation Mass vaccination programs and campaigns Polio, small pox, DPT, Hepatitis, Yellow fever Mass treatment programs – Onchocerciasis, de-worming programs. For some CDs, intervention in other sectors is required Environmental health – elimination of breeding sites, spraying Agricultural practices such as poultry handling and exposure to soil pathogens during farming. Utilitarian Approaches – “Greatest good for the greatest number” – Sort of cost benefit analyses, where the benefits of the intervention such as the lives saved or years of live gained, etc, exceed the costs which could range from just the prick of a needle to a minority developing side effects of the vaccine. Social Isolation and Quarantine measures Home treatment Isolation Mass Vaccination programs Polio in Nigeira

39
Regulations and Laws National response remains the bedrock of intervention National laws and capacities vary. International Regulations and laws introduced 1851 – International Sanitary regulations in Europe following cholera outbreak 1951- international sanitary regulation by WHO. 1969- Replaced by the International Health regulation Minor changes in 1973 and 1981 cholera, plague, yellow fever, smallpox, relapsing fever and typhus 2005 – Revised International Health Regulation Challenge of enforceability of international agreements. Regulations and Laws- Challenge of enforceability, as it often relies on international cooperation and pressure

40
Regulation and laws – WHO 2005 International health regulation
IHR (2005) is a legally binding agreement among member states of WHO to cooperate on a set of defined areas of public health importance. Arrived at by consensus of all member countries of WHO, with clear arbitration mechanisms Its elements include Notification: National IHR Focal Points and WHO IHR Contact Points Requirements for national core capacities Recommended measures External advice regarding the IHR (2005) Notification - The IHR (2005) require States to notify WHO of all events that may constitute a public health emergency of international concern and to respond to requests for verification of information regarding such events. Under the WHO Constitution, all WHO Member States are automatically bound by the new IHR (2005) unless they affirmatively opt out within a limited time period, namely by 15 December No WHO Member State has completely opted out, and only a very small number made reservations.
 is a legally binding agreement among member states of WHO to cooperate on a set of defined areas of public health importance. Arrived at by consensus of all member countries of WHO, with clear arbitration mechanisms. Its elements include. Notification: National IHR Focal Points and WHO IHR Contact Points. Requirements for national core capacities. Recommended measures. External advice regarding the IHR (2005) Notification - The IHR (2005) require States to notify WHO of all events that may constitute a public health emergency of international concern and to respond to requests for verification of information regarding such events. Under the WHO Constitution, all WHO Member States are automatically bound by the new IHR (2005) unless they affirmatively opt out within a limited time period, namely by 15 December No WHO Member State has completely opted out, and only a very small number made reservations.")
41
Partnerships and Collaboration
Collaboration vs. coercion Importance of partnerships – MDG 8: “Develop global partnerships for development” Comparative advantage of partners Inclusiveness Examples of partnerships Over 70 Global health partnerships available Examples include the Stop-TB program, GFATM, RBM, UNAIDS, GAVI, Global Outbreak Alert and Response Network, GAIN, bilateral and multilateral organizations. Effectiveness of global response is based on the principle of collaboration The Global Outbreak Alert and Response Network (GOARN) is a technical collaboration of existing institutions and networks who pool human and technical resources for the rapid identification, confirmation and response to outbreaks of international importance.
 is a technical collaboration of existing institutions and networks who pool human and technical resources for the rapid identification, confirmation and response to outbreaks of international importance.")
42
Isn’t Donor Collaboration Wonderful?
WHO INT NGO CIDA 3/5 UNAIDS GTZ RNE UNICEF Norad WB Sida USAID T-MAP MOF UNTG PMO CF DAC GFCCP PRSP PEPFAR HSSP GFATM MOEC MOH SWAP CCM NCTP CTU CCAIDS NACP LOCALGVT CIVIL SOCIETY PRIVATE SECTOR Source: WHO: Mbewe

43
A paradigm shift - Enlightened Self interest
Communicable diseases have no borders. Predominantly affect the poor, and poor countries Also affect richer households and countries. Interventions are non-rival, non-exclusive and have positive externalities. Elimination and control of certain communicable diseases increases global health security. Limited financial incentives for the market to drive needed innovation in research and drug development Mismatch between global health need and health spending Global health security is therefore inextricably tied to the effective control of CDs in developing world. The need to move beyond charity-model. Non-rival –The benefits from the Interventions can be enjoyed simultaneously by all in the community. Lack of access to TB drugs may fuel resistance and the development of MDR-TB

44
Global Mismatch Between Disease Burden and Health Spending

45
Global Mismatch Between Disease Burden and Health Spending

46
Future Population Growth Will be in LICs and MICs
Therefore by the percentage of the global population susceptible to CDs will increase significantly.

47
Key principles of an Effective Global Response
Respect for the value of each life Behind every statistic is an individual Understanding of the social context that govern individual decision making Disease Surveillance and reporting Management and containment of outbreaks Strong legal and regulatory framework Sustained and predictable financing Building national health systems Respect for the value of each life – Behind the numbers of those affected by CDs are individuals, with hopes dashed and who make complex decisions, the context of which we are not very familiar with. The person who refuses an HIV test, against the background of stigma The mother in northern Nigeria who prevents her child from accessing polio vaccines because of the outbreak of vaccine-derived polio

48
World Bank’s involvement
Relevance to our mandate CDs disproportionately affect the poor and LICs and MICs Enormous economic consequences Major constraint to achieving the MDGs Major source of financing for poor countries This position is rapidly changing with the entrance of newer players in DAH such as Gates foundation, Bilaterals, multilaterals. Call for innovative financing schemes

49
World Bank $430 million committed to malaria booster projects in Africa By 2008, 21 million bed nets and 42 million ACT doses would have been distributed. As of June 2007, the World Bank had approved financing of $377 million for 40 projects in 45 countries in all six geographic regions to combat Avian influenza Cumulative WB commitment to HIV/AIDS is over $2.5 billion more than 21 million LLINs and over 42 million doses of ACT will be distributed under projects in the Booster Program’s first phase ending in 2008.

50
Sources of Development Assistance for Health
Source: Michaud 2006

51
The World Bank’s new HNP strategy
Five broad strategic directions of the World bank Focus on HNP Results Strengthening health systems Ensuring synergies between Health Systems strengthening and priority disease interventions Intersectoral approach to HNP results Increase strategic and selective engagement with development partners.

52
Thank You. The World Bank has committed more than $430 million to Booster projects. A nine-fold increase in IDA funding for malaria control in Africa.

Similar presentations