Download presentation
Presentation is loading. Please wait.

1
The Knee: Anatomy and Injuries

3
2 Joints at the Knee Tibiofemoral Joint – formed between tibia and femur A HINGE JOINT Patellofemoral joint – formed between the patella and the femur A GLIDING JOINT

5
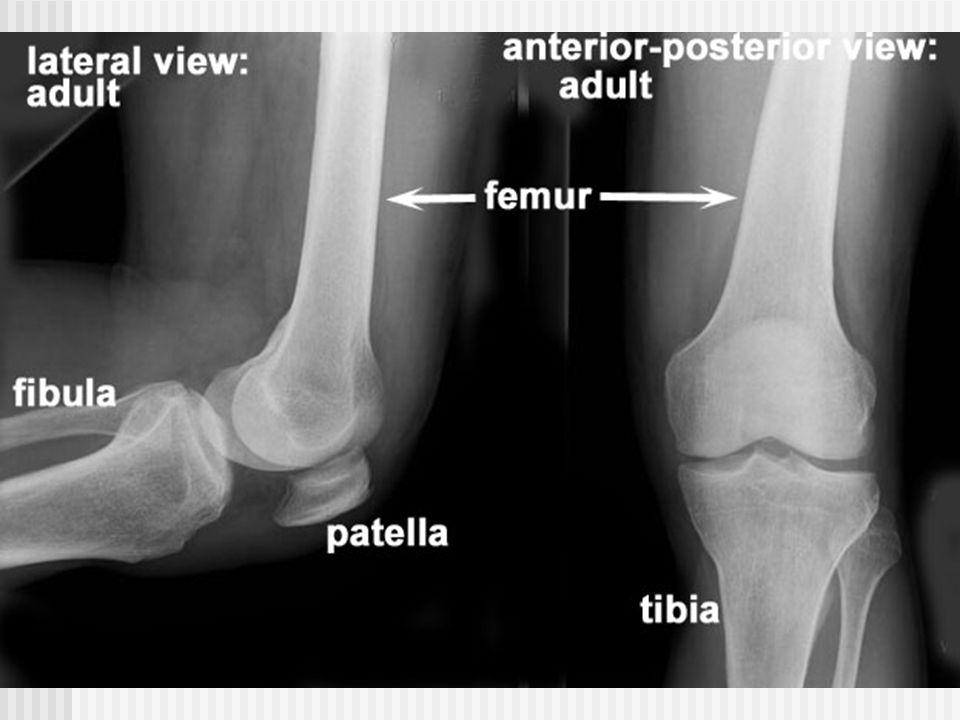
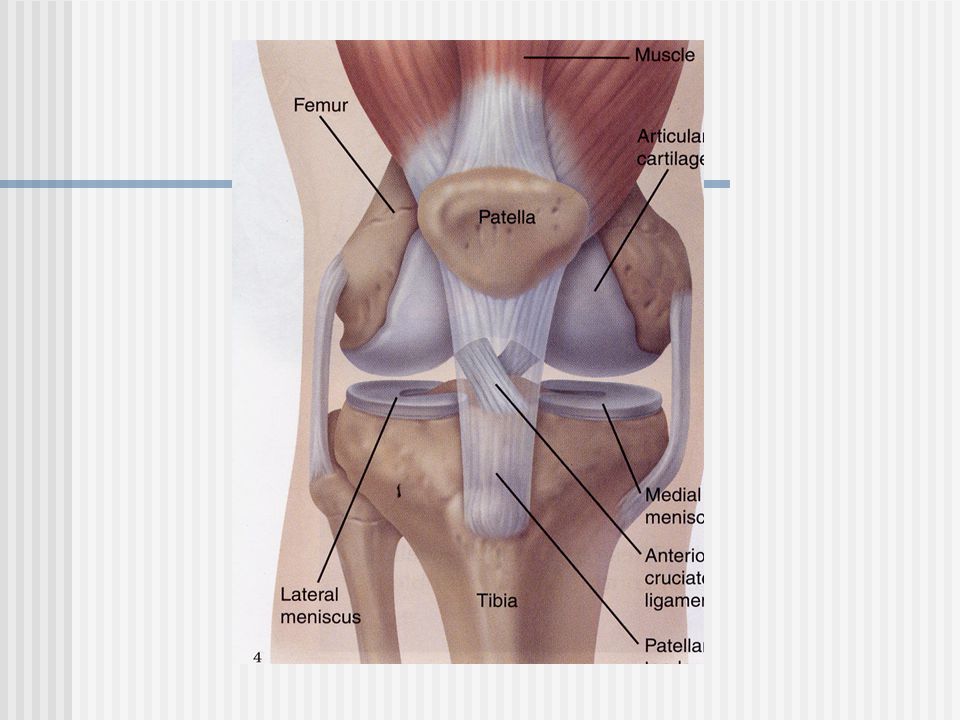
Skeletal Anatomy Femur
proximal – head and neck of femur, greater trochanter distal – medial and lateral condyles and epicondyles

6
Patella – largest sesamoid bone in body
Tibia – tibial plateau forms knee joint with femur The fibula is not a part of the knee joint

8
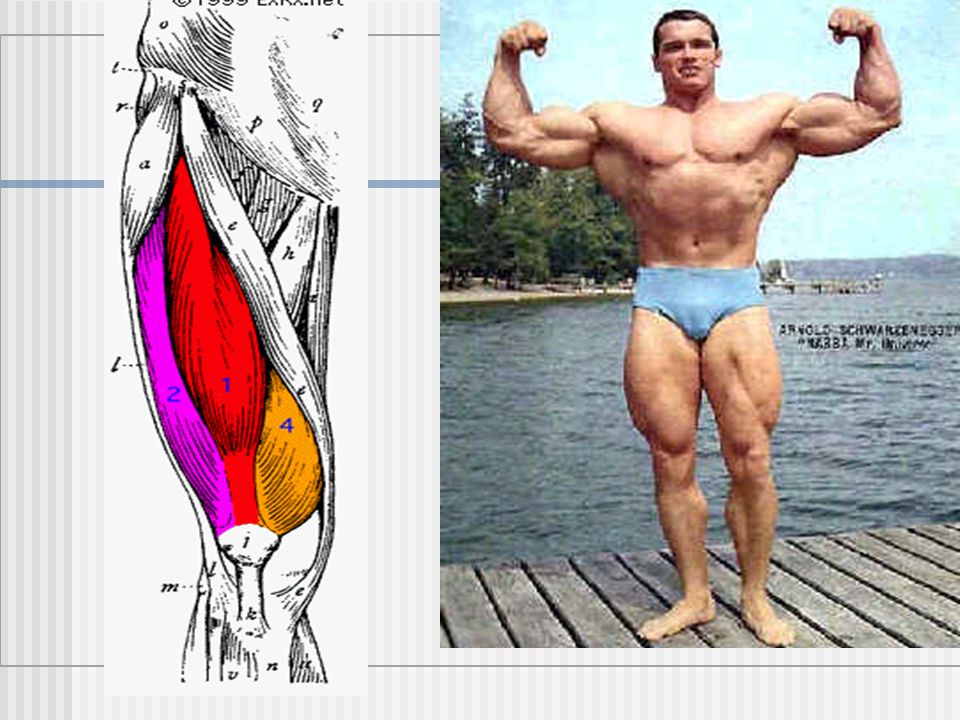
Muscles that move the knee and thigh
The Quadriceps – Knee Extension 1. Vastus Medialis 2. Vastus Lateralis 3. Vastus Intermedius 4. Rectus Femoris – 2 joint muscle that also acts as a hip flexor

11
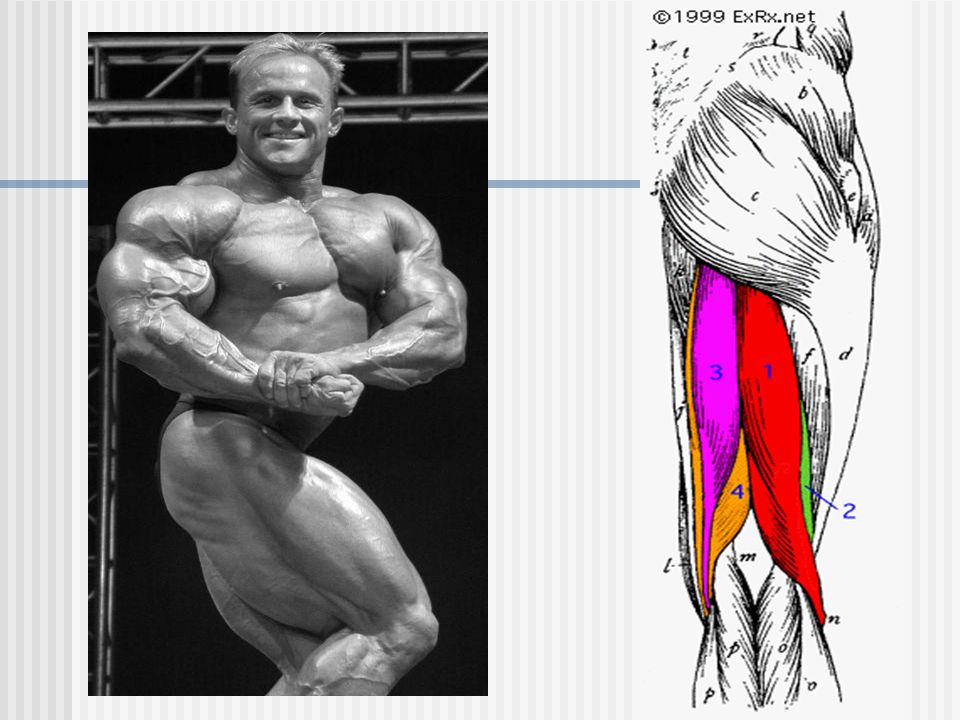
The Hamstrings- knee flexion 3 muscles: 1. Biceps Femoris
2. Semimembranosus 3. Semitendinosus

14
The Adductors (Groin) Adduct the thigh 1. Adductor Longus
2. Adductor Magnus 3. Adductor Brevis 4. Gracilis

15
The Sartorius: - flexes, abducts, and laterally rotates thigh - longest muscle in the body, “tailor’s muscle” - Crosses hip and knee joint

16
The Iliotibial Tract (IT Band) - neither a muscle or tendon, but a long, thick band of tissue that inserts into the lateral tibia (Gerdy’s Tubercle)
")
17
What muscles can you identify?

19
The Major Knee Ligaments
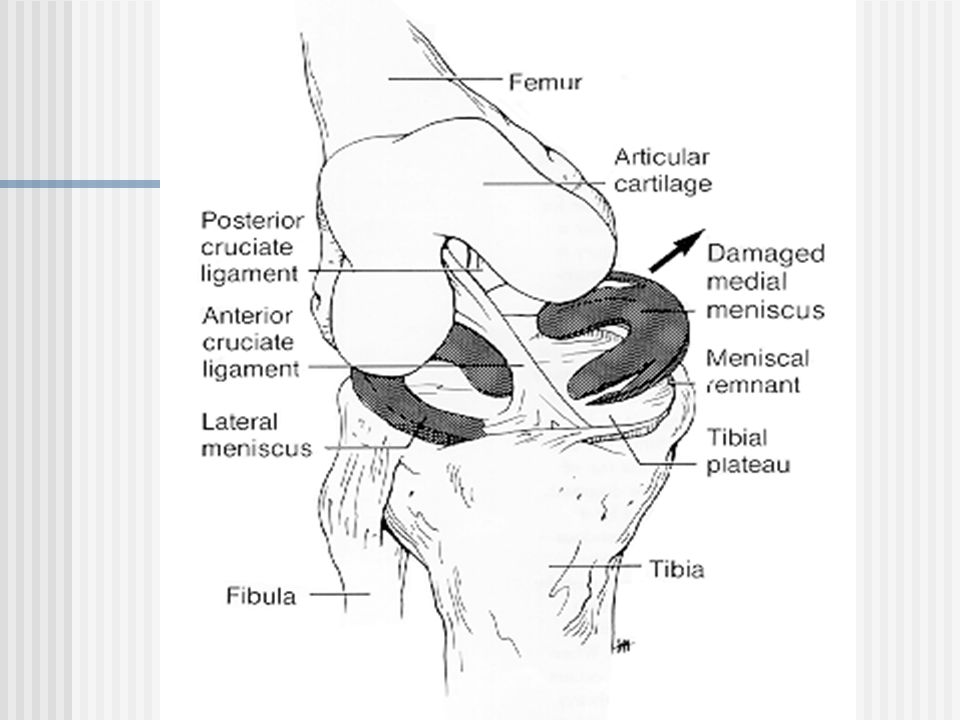
1. ACL – Anterior Cruciate Ligament prevents anterior motion of tibia 2. PCL – Posterior Cruciate Ligament prevents posterior motion of tibia 3. MCL – Medial Collateral Ligament 4. LCL – Lateral Collateral Ligament

20
ACL and PCL run from femur to tibia and form an X inside the knee

21
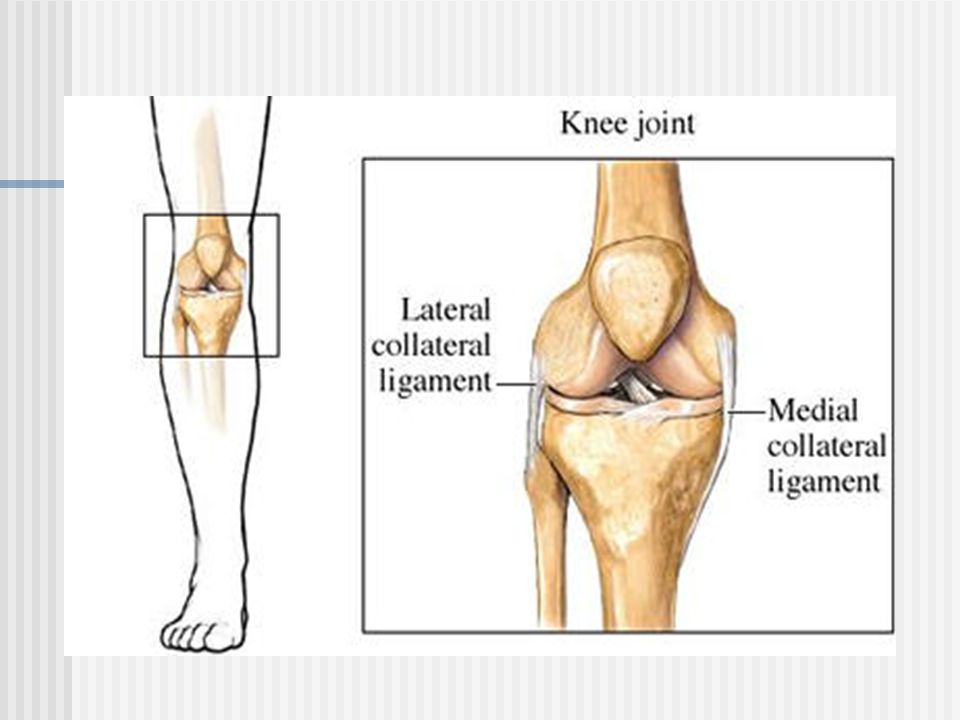
The Collateral Ligaments
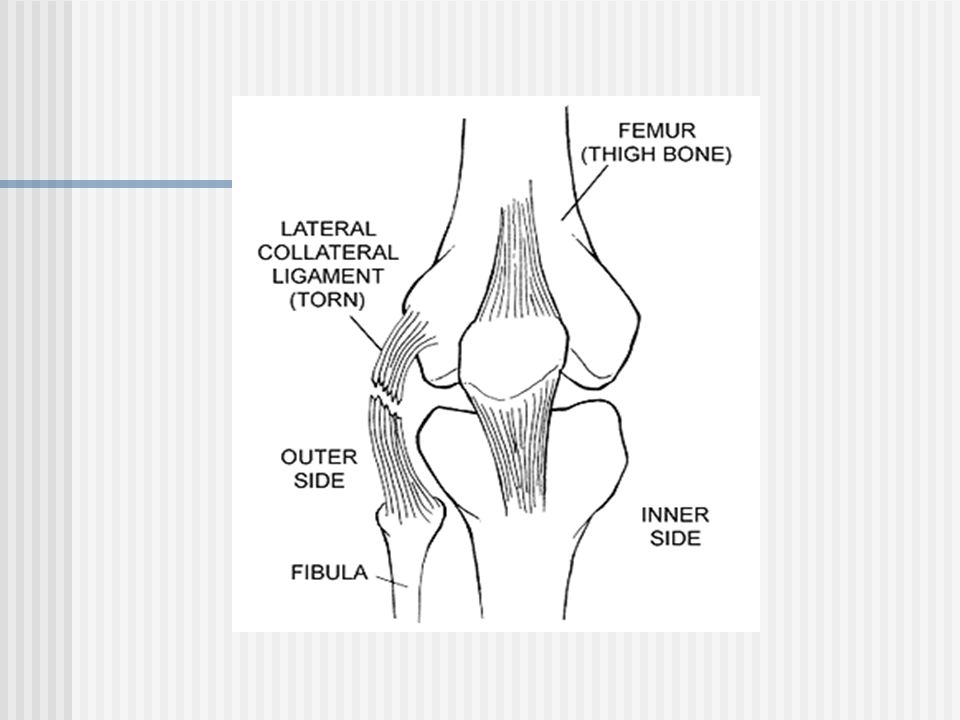
MCL: Medial Collateral Ligament Runs from medial femur to medial tibia LCL: Lateral Collateral Ligament Runs from lateral femur to head of fibula

23
The Meniscus A “c”-shaped piece of fibrocartilage located in the knee joint between the femur and attached to the top of the tibia Cartilage = meniscus

26
Differences between medial and lateral
- larger and more C-shaped - more firmly attached to tibia - has attachments to MCL Lateral - smaller and more round or O-shaped - not firmly attached to tibia and LCL

27
Blood Supply to the Meniscus
Mostly avascular – little or no blood supply Only the outer 20% has a blood supply * Does not have the ability to heal itself unless there is a small tear in the outer 20%

28
Functions of Meniscus Stability Shock absorption
Lubrication and nutrition Allows adequate weight distribution

29
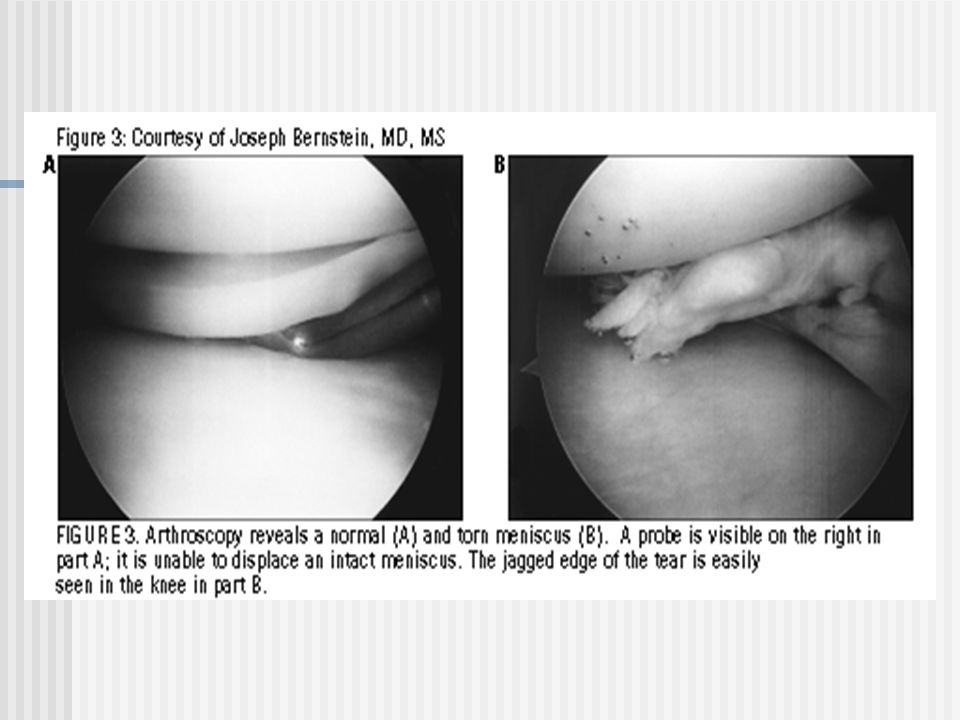
Normal Torn

31
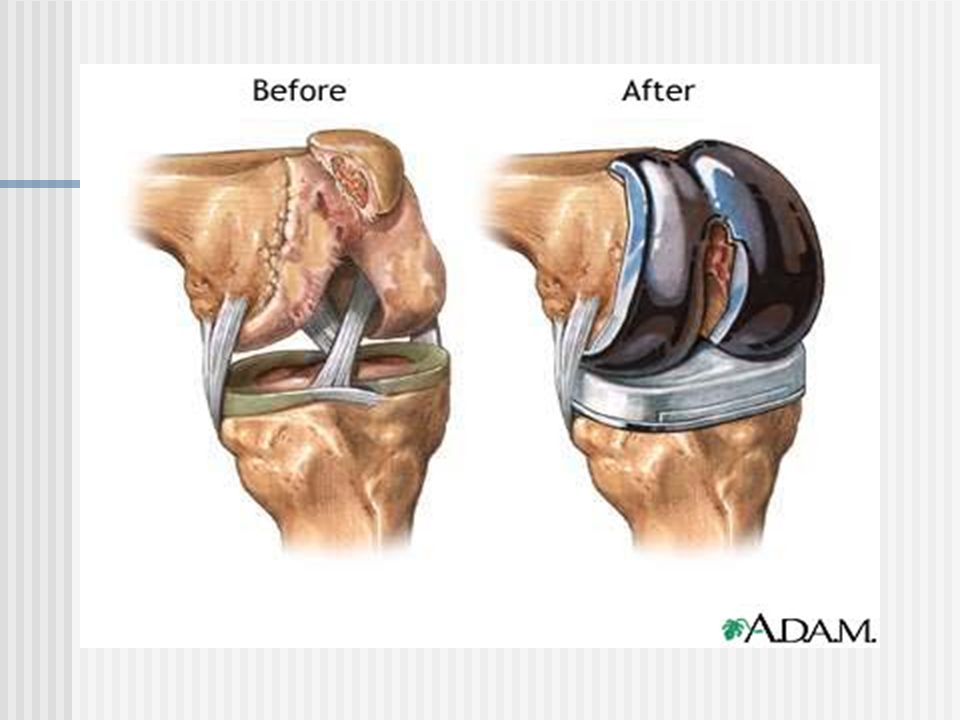
Total Knee Joint Replacement
Surgery to replace a painful damaged or diseased knee joint with an artificial joint (prosthesis) Artificial hip invented 1962 1969 – first artificial knee in USA
 Artificial hip invented – first artificial knee in USA.")
32
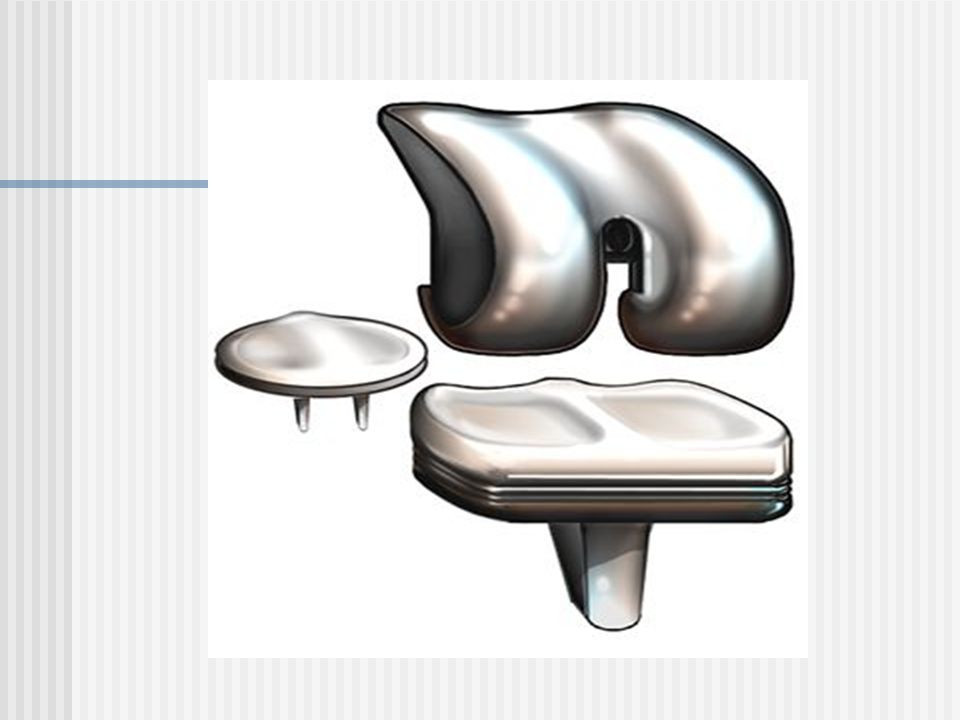
The Knee Surgery Thin layer of bone removed from femur – thin metal replaces it Upper layer of tibia replaced with plastic Back of patella replaced with plastic Parts fastened with “bone cement”

33
Risks of Knee Joint Replacement
Blood clots in large veins Infection Stiffness Implant Loosening/Failure - more of a problem in younger patients

37
Knee Injuries and Conditions

38
Genu Valgum: “knock knees”

39
Genu Varum: “bowlegs”

40
Genu Recurvatum: hyperextension of the knee joint

41
Patellofemoral Disorders
Problems with patella – most common cause of knee pain Anatomy: - Patella is a sesamoid bone formed in Quad tendon - Patellofemoral joint – patella and femur - Compression forces – <body weight during walking 2.5 x body weight during stairs

42
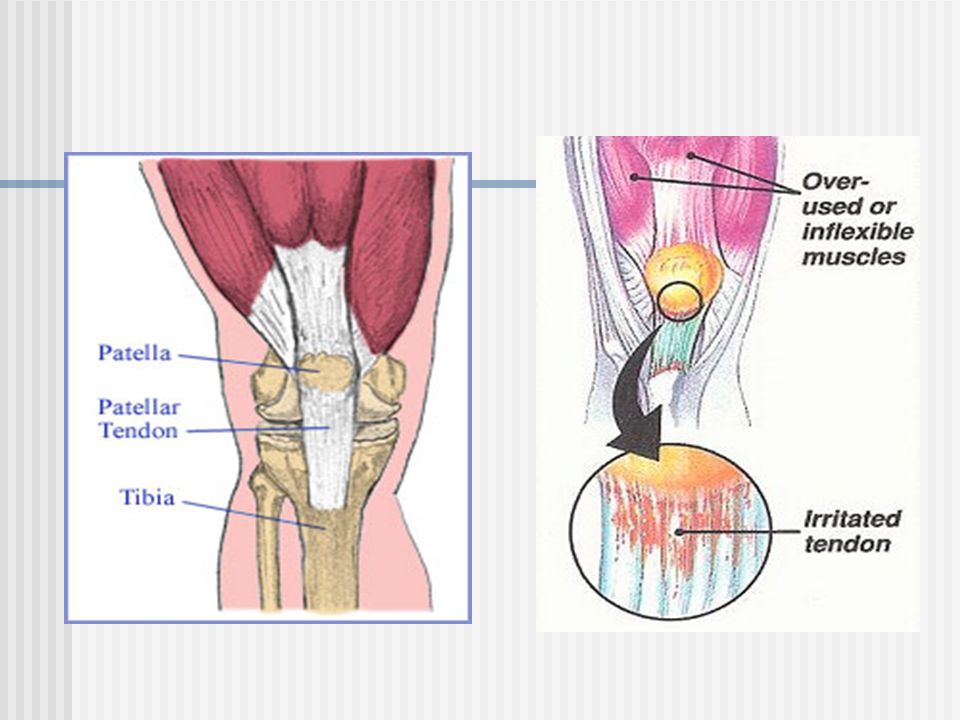
Patellar Tendonitis “Jumper’s Knee”
Inflammation and degeneration of the tendon that connects the kneecap (Patella) to the shin bone (Tibia).
 to the shin bone (Tibia).")
44
Chondromalacia Damage to the cartilage under the kneecap
Causes: abnormal patellar tracking Most Common Symptom: Knee pain when walking up and down stairs Prevention: strengthen quads Minimize squats, downhill running, biking with low seat

45
Chondromalacia

46
Patellar Dislocation Involves the patella sliding out of its position on the knee. Caused by direct blow or abnormal twisting of the knee Usually lateral

47
Osgood-Schlatter Disease
1. Painful swelling over tibial tuberosity (patellar tendon insertion) 2. Usually occurs between 9-13 years of age 3. Pain increases with activity
 2. Usually occurs between 9-13 years of age. 3. Pain increases with activity.")
49
The Chopat Strap

50
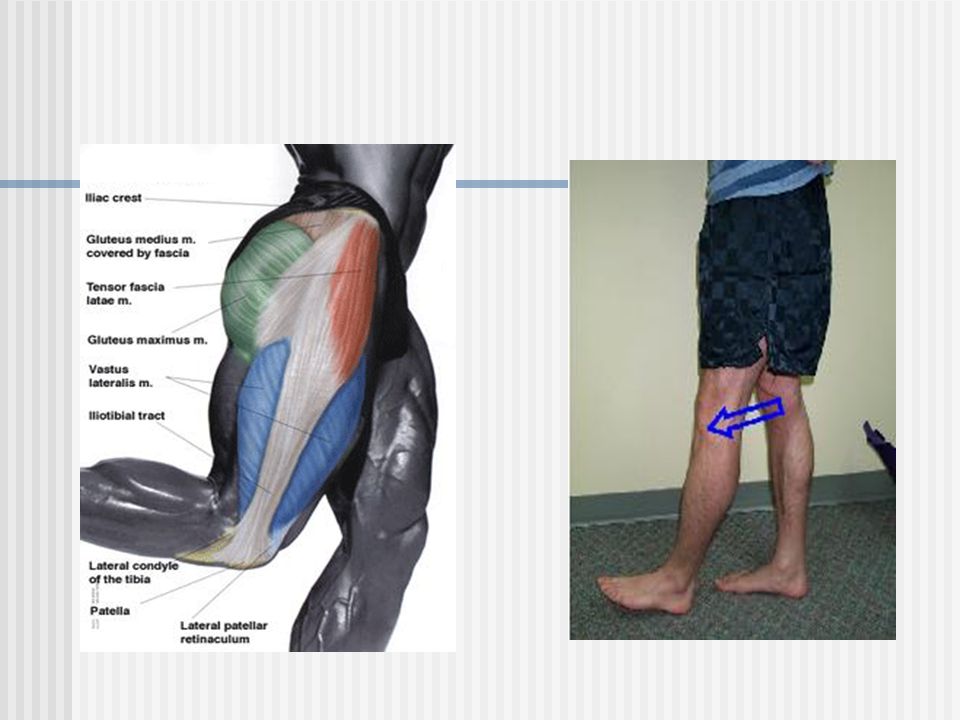
Iliotibial Band Friction Syndrome
Occurs where IT Band rubs over femur at the knee joint Common in running (esp. downhill) or any activity with repetitive flexion Hills or stairs increase pain Lots of IT Band stretching
 or any activity with repetitive flexion. Hills or stairs increase pain. Lots of IT Band stretching.")
52
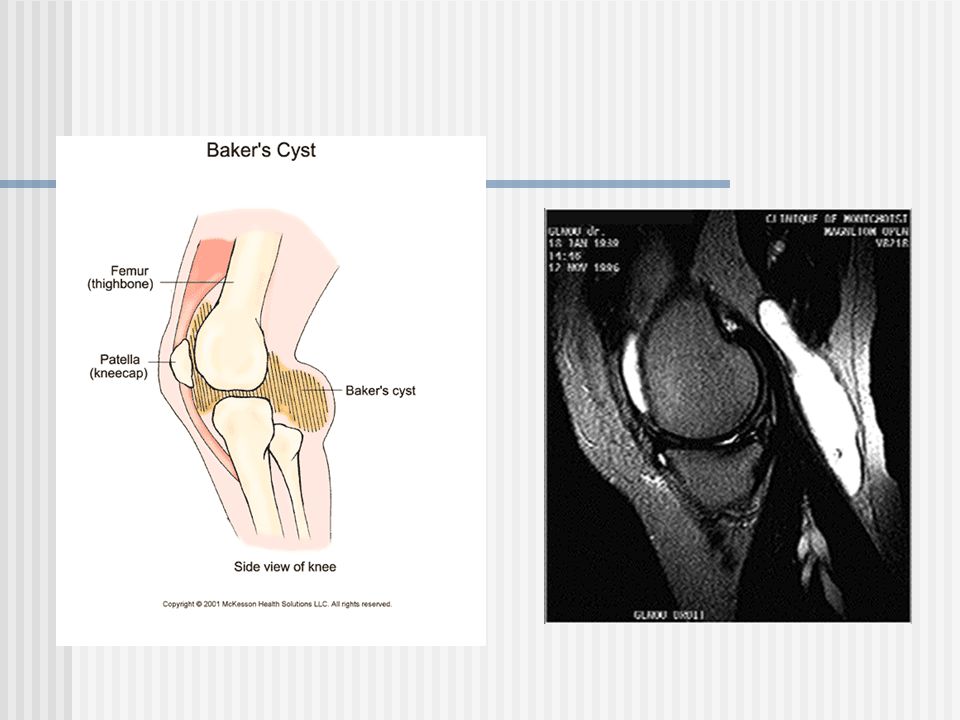
Popliteal Cyst “Baker’s Cyst”
Fluid accumulation in posterior knee (popliteal space) Patient usually complains of a mass behind the knee
 Patient usually complains of a mass behind the knee.")
54
Prepatellar Bursitis “Housemaid’s Knee”
Tender swelling over the kneecap (prepatellar bursa)
")
55
Pes Anserine Bursitis Inflammation of a bursa in your knee. The pes anserine bursa is located on the inner side of the knee just below the knee joint. Tendons of three muscles attach to the shin bone (tibia) over this bursa SGT: Sartorius, Semitendinosis, Gracilis
 over this bursa. SGT: Sartorius, Semitendinosis, Gracilis.")
56
Knee Sprains

57
ACL Sprain >200,000 injuries/year >100,000 reconstructions/year
Higher incidence in females Males = contact Females = noncontact

58
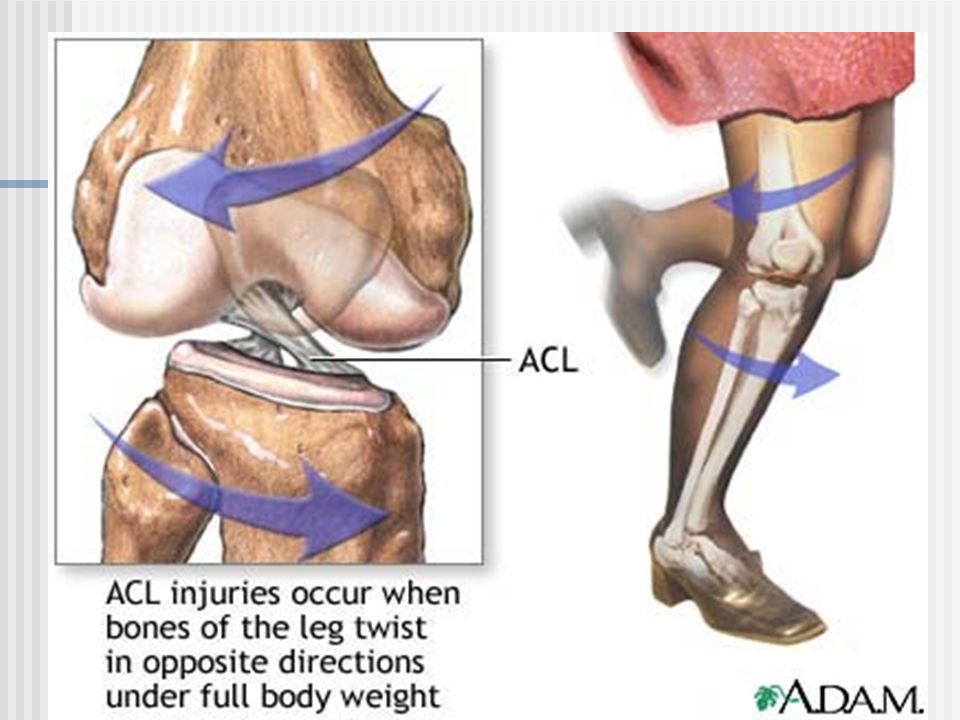
ACL Sprain 1. MOI: twisting of knee forced hyperextension
lateral blow to knee *foot must be firmly anchored to playing surface 2. 50% of people describe a “pop” in knee 3. Knee fills with blood quickly Hemarthrosis 4. Usually immediate loss of motion Knee feels unstable

60
Anterior Drawer Test: examiner attempts to slide the tibia forward which may indicate a torn ACL ligament

61
ACL Sprain Who needs surgery? - Activity level? - Level of Competition
- Age?

62
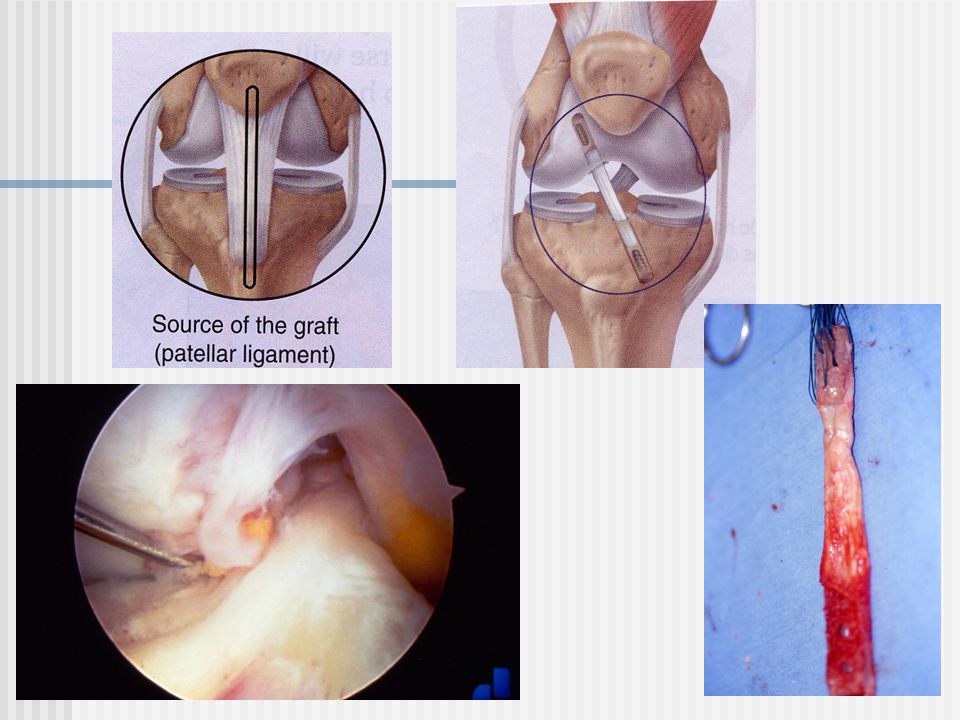
ACL Surgery Arthroscopic Graft options Patellar Tendon Semitendinosus
Gracilis Cadaver Synthetic

64
PCL Sprain MOI: excessive hyperextension hyperflexion
tibia forced posteriorly (blow to front of knee) “dashboard knee” Possibly 90% of all PCL injuries due to motor vehicle accidents?
 dashboard knee Possibly 90% of all PCL injuries due to motor vehicle accidents")
65
Mild hemarthrosis Posterior knee pain Walk with knee slightly flexed, avoid full extension Posterior sag of tibia Surgery?

66
MCL Sprain MOI: Blow to the outside of the knee = Valgus Force
Possible overuse – breaststroke in swimmers Commonly associated with meniscal injuries – attached to medial meniscus No surgery

67
MCL Sprain

68
Valgus Stress Test: tests for injury to the MCL ligament

69
LCL Sprain MOI: Blow to inside of the knee – Varus force
Grade III tear may require surgery

71
Varus Stress Test: tests for injury to the LCL ligament

72
Injuries to the Meniscus
MOI: Rotation of the knee as the knee extends during rapid cutting or pivoting

73
Signs and Symptoms: - pain - joint line tenderness - catching or locking - knee buckling or giving way - swelling - incomplete flexion - clicking on stair climbing

74
Surgery? Meniscectomy: removal of the meniscus - Total meniscectomy = osteoarthritis Depends on location of tear, type of tear, and blood supply

75
Types of Meniscal Tears
bucket handle Flap tear Transverse tear Horn tear

77
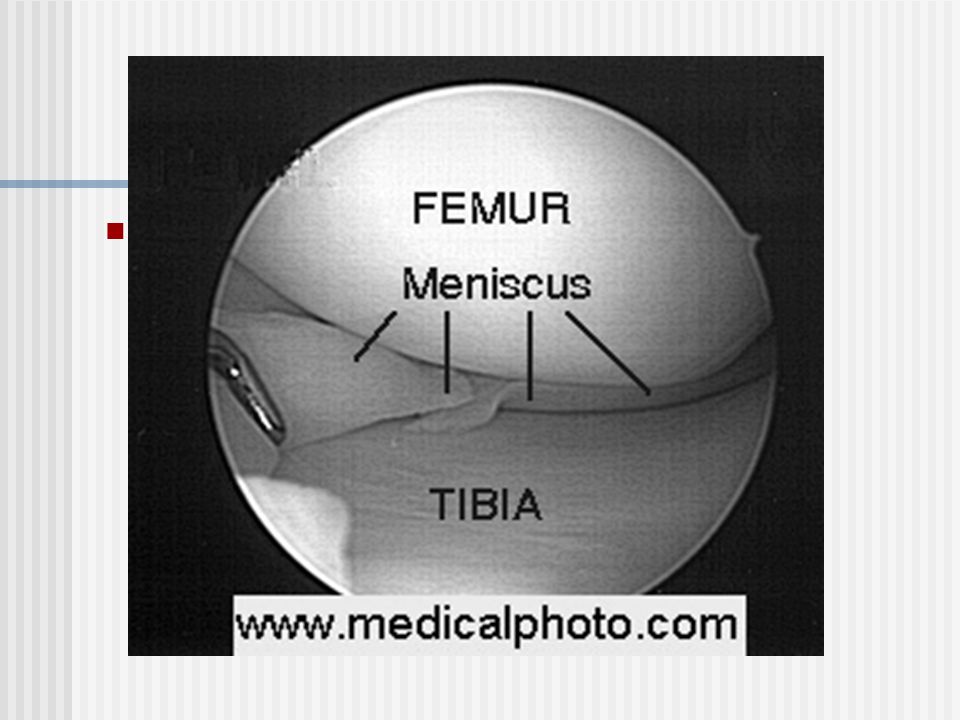
Tests for Meniscal Tears
Apley’s Compression

78
“The Unhappy Triad” Tear of the medial meniscus, anterior cruciate ligament (ACL), and medial collateral ligament (MCL)
, and medial collateral ligament (MCL)")
Similar presentations











 articulating with 2 concave surfaces (tibia) Poor bony stability Stability increased.>")








>")




