Download presentation
Presentation is loading. Please wait.

1
On Field Management: Athletic Emergencies
Jim Ellis, MD, FACEP Faculty, Primary Care Sports Medicine Fellowship Program Steadman Hawkins Clinic of the Carolinas

2
Why we do what we do On October 24, 1971 Chuck Hughes of the Detroit Lions went across the middle on a pass play and collapsed. Legendary LB Dick Butkus frantically waved to the sideline for help. Despite the efforts of the training staff, he died of a “heart attack” and remains the only on field death in the history of the NFL.

4
Objectives Know the risks of the sport you cover
Know your specific role/responsibility Know your players’ illnesses Know what equipment to have Know the Emergency Action Plan

6
ATLS, ACLS, “ASLS” Advanced Sports Life Support
Airway Breathing Cardiac Circulation Cervical Spine Concussion Conditions/Environment Crisis Management/Disaster Diabetes

8
Airway Problems Direct Trauma Anterior neck trauma Indirect Trauma
Severe concussion can lead to unprotected airway High cervical spine injury

10
Airway Evaluation Is the player talking? Is he tachypneic or agonal?
What is the pulse ox? EMS bring pulse ox!

11
Airway - Maintainable Supplemental oxygen
Chin lift or jaw thrust (for c-spine) Nasal or oral airway Bag-valve-mask/pocket mask/barrier
 Nasal or oral airway. Bag-valve-mask/pocket mask/barrier.")
12
Airway Evaluation Unmaintainable
Airway is inadequate with basic support Procedural intervention is required Must remove facemask to have unencumbered access to the airway on anyone immobilized Need Advanced Life Support EMS unit at high risk events

13
Endotracheal Intubation
The right person The right equipment The right drugs The right plan for the difficult airway

14
Anatomy

15
Airway Adjuncts Intubating Stylet Lighted Stylet
LMA *great tool for the airway novice Intubating LMA Levitan Fiberoptic Scope

17
LMA and Intubating LMA

19
Surgical Airway Unsuccessful endotracheal intubation
Mandibular fracture Anterior neck trauma Laryngeal fracture Stridor

20
Surgical Airway Know the anatomy Know the equipment Know the procedure

21
2002 Super Bowl Kurt Warner played with a laryngeal fracture – sideline cricothyrotomy kit

22
2004 Al Lucas Arena League player went down headfirst on a kick-off
Evaluated by MD and ATC on FOP While being loaded into the ambulance, stopped breathing (within 10 minutes of injury) Died from airway compromise due to C1/C2 fracture and concussion despite using an LMA for airway
 Died from airway compromise due to C1/C2 fracture and concussion despite using an LMA for airway.")
24
1997 Reggie Brown Lions linebacker injured vs Jets
C1/C2 fracture with CHI Airway compromise from above On field mouth to mouth and BVM Response saved his life and had remarkable post op recovery

26
Breathing Problems Massive Hemothorax Tension Pneumothorax
Load and Go! Tension Pneumothorax Use pulse oximetry for help Large bore IV catheter(14 gauge) 2nd intercostal space, midclavicular line LEAVE IT IN!
 2nd intercostal space, midclavicular line. LEAVE IT IN!")
27
2001 Drew Bledsoe Patriots QB was driven into the ground on the sideline Was short of breath after the game Taken to Mass General Hospital and had a chest tube inserted to reinflate his lung and an autotransfusion Tom Brady became the starter

29
2008 Lauren Chang Cheerleader accidently kicked in the chest
Had collapsed lungs - bilateral Died from tension pneumothorax

31
Breathing Problems Asthma Know your players
Nebulizer vs inhaler (use a spacer) Keep an extra MDI (inhaler) Make sure EMS gives the right Epi dose SQ/IM (1:1000) vs IV (1:10,000) Can use Epi-Pen if needed (same dose as allergic reaction 0.3cc) Peak Flow Meter (know their baseline)
 Keep an extra MDI (inhaler) Make sure EMS gives the right Epi dose SQ/IM (1:1000) vs IV (1:10,000) Can use Epi-Pen if needed (same dose as allergic reaction 0.3cc) Peak Flow Meter (know their baseline)")
32
2001 Rashidi Wheeler Northwestern football player
Died secondary to asthma Known asthmatic in difficult workout ?Complicated by ephedra use

34
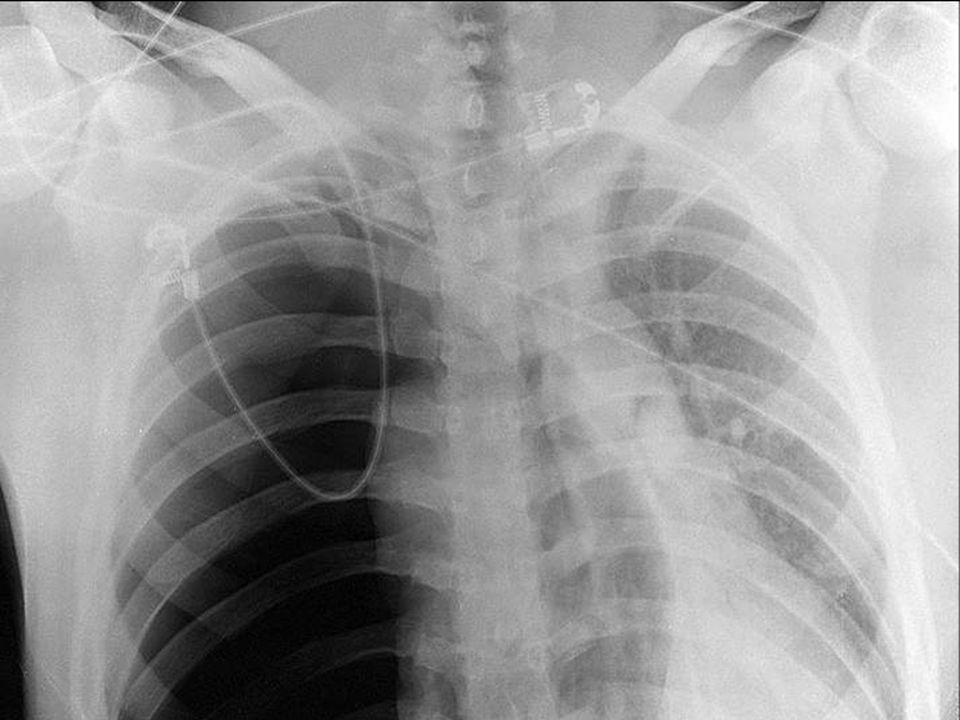
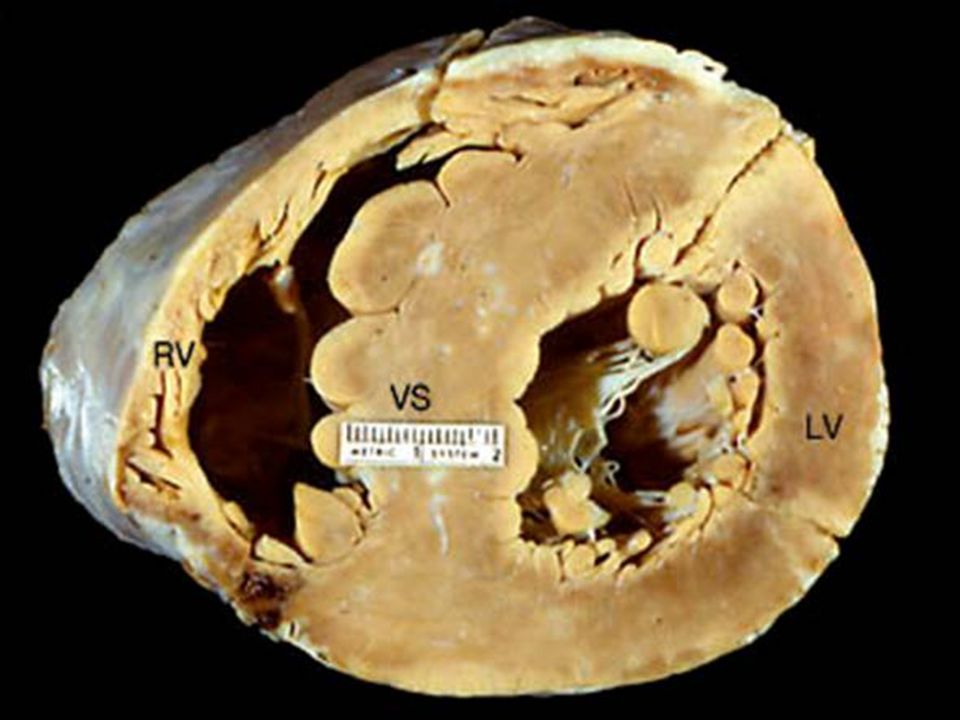
Cardiac Problems Cardiac Etiology Sudden cardiac death
Arrhythmia of unknown etiology Hypertrophic cardiomyopathy Commotio cordis/cardiac concussion (hockey and baseball) Coronary artery disease in coaches and referees*
 Coronary artery disease in coaches and referees*")
36
Cardiac Interventions
CPR if AED is not right there AED – know where it is at all times and have nearby at events Practice run getting the AED Trauma scissors Manual defibrillator (EMS) Time to shock is critical!
 Time to shock is critical!")
37
Cardiac Interventions
Every minute that passes, there is a 10% decrease in chance of survival. 90% chance of survival at 1 minute 50% chance at 5 minutes 10% chance of survival if the initial shock is delivered 9 minutes after the cardiac arrest occurred Don’t wait for EMS

39
2005 Jiri Fisher Collapsed on the ice Saved with CPR and AED
Key was a rapid response to a true life threatening emergency Etiology was underlying arrhythmia

41
1996 Polish Chef de Mission Opening Ceremony 1996 Olympic Games
Cardiac arrest on the field of play 10,000 athletes / worldwide TV audience Defibrillated on the FOP and intubated Transported with return of vital signs Subsequent death in the hospital

43
2011 Al Schmidt at UGA Mississippi State track official Known CAD
At SEC Track meet on UGA campus Witnessed cardiac arrest Well practiced EAP AED on site in 2 minutes Survived to discharge neuro intact

45
Other serious cardiac events
1988 – Pete Maravich(NBA) congenital coronary artery 1990 – Hank Gathers(NCAA) HCM 1993 – Reggie Lewis(NBA) HCM 1998 – Chris Pronger(NHL) commotio 2003 – Marc Vivien-Foe(soccer) SCD 2004 – Sergei Zholtok(NHL) HCM
 congenital coronary artery – Hank Gathers(NCAA) HCM – Reggie Lewis(NBA) HCM – Chris Pronger(NHL) commotio – Marc Vivien-Foe(soccer) SCD – Sergei Zholtok(NHL) HCM.")
46
Other serious cardiac events
2005 – Jaxon Logan(NCAA) commotio 2005 – Thomas Herrion(NFL) HCM/CAD 2007 – Damien Nash(NFL) arrhythmia of unknown etiology 2007 – Antonio Puerta(soccer) SCD 2011 – Wes Leonard(BB) SCD/?HCM
 commotio – Thomas Herrion(NFL) HCM/CAD – Damien Nash(NFL) arrhythmia of unknown etiology – Antonio Puerta(soccer) SCD – Wes Leonard(BB) SCD/ HCM.")
47
Circulation Problems Abdominal Trauma/Hemorrhage
Splenic or liver injury Don’t confuse with dehydration High index of suspicion Life/limb threatening hemorrhage Two large bore IV’s Load and go (nearest appropriate facility)
")
48
2006 Chris Simms September game vs Panthers Multiple hard hits
No specific complaint of LUQ pain Treated for dehydration Ruptured spleen Surgery at St. Joe’s Hospital (< 1 mile)
")
50
1989 Clint Malarchuk NHL goalie with skate to the neck
Life threatening hemorrhage Direct pressure and rapid transport Went directly to OR for vascular surgery and survived

52
Circulation Problems Sickle Cell Trait
- easy to diagnosis with a simple screening blood test - 10 known deaths since 2000 - 8-10% of black population - NATA policy statement - NCAA ?mandatory testing

53
Circulation Problems Sickle Cell Trait - Identify high risk activities
- common in off- or pre-season - monitor first few workouts - ease into preseason conditioning - SCT muscle pain and weakness - dehydration cramps/”locking up”

54
2008 Ereck Plancher Collegiate athlete with known sickle cell trait
Off-season program Strenuous workout Exhibited difficulty Died on the field

55
Sickle Cell Trait - deaths
Preston Birdsong –TTU 2000 DeVaughn Darling – FSU 2001 Aaron Richardson – BGU 2004 Aaron O’Neal – Missouri 2005 Dale Lloyd – Rice 2006 Chad Wiley – NC A&T 2008 Ja'Quayvin Smalls – 2009 WCU Bennie Abram – 2010 Ole Miss

56
Cervical Spine Injury

57
Cervical Spine Immobilization
Clinical decision Standardize approach and procedure Have unencumbered airway access Don’t assume that EMS knows what to do – you teach them how you want it done and practice before the season (NATA video)
")
59
Spinal Cord Injury Treatment “Options”
High dose steroids – methylprednisolone 30 mg/kg bolus Maintenance dose – 5.4 mg/kg/hr (needs to be started at hospital within 3-8 hours) Hypothermia – 30 cc/kg of LR cooled to degrees F should drop temp to around 95. Ideal temp between Kevin Everett case
 Hypothermia – 30 cc/kg of LR cooled to degrees F should drop temp to around 95. Ideal temp between Kevin Everett case.")
60
2007 Kevin Everett Made a tackle on the kickoff with his head down
Received cold IV fluids and steroids The real key to his recovery was going to the appropriate hospital and being in surgery within 2 hours

62
Concussion Dr. Sease concussion update
Clinical judgment determines if severity of head injury negates the validity of the c-spine exam Always fear the concussion when paired with the C1/C2 fracture – axial load with flexion If immobilizing, remove the facemask even if awake and talking

64
2006 and 2007 Trent Green Concussions while playing with Chiefs (2006) and Dolphins (2007) Both were significant and had prolonged recovery periods Was able to return to play after evaluation and clearance

67
2000 Blaine Bishop Titans DB in Super Bowl
Brief LOC / neck pain / L arm numbness Spinal immobilization Transport to hospital Final diagnosis – concussion/cervical strain Comprehensive pregame planning

69
Conditions/Environment
Heat illness Heat cramps/exhaustion/stroke 33 heat related deaths in football since 1995 Korey Stringer of the Minnesota Vikings Steve Belcher of the Baltimore Orioles

70
Conditions/Environment
Lightning – approximately people die per year in the US from lightning In 2006, 5 people died at one event during a storm (softball) Rosbin Yuman and Lester Marrioquin soccer players killed in 2001 Tend to the unconscious first – they usually need more electricity (AED)!
 Rosbin Yuman and Lester Marrioquin soccer players killed in Tend to the unconscious first – they usually need more electricity (AED)!")
71
Crisis Management/Disaster Planning
Know the disaster plan/EAP Have a written Emergency Action Plan for every venue including practice Practice the EAP – docs, ATC’s, coaches Is there an evacuation plan? Be familiar with the Rally Point Take care of the visiting team Have a roster for roll call

73
Diabetes Know your athletes Either high or low when they are sick
Urine dipstick is quick and easy High – dipstick + for glucose and maybe ketones if DKA (Rx with NS) Low – dipstick may have ketones from starvation but not spilling glucose (Rx with D50W or glucagon emergency kit) Usually need to call EMS in either situation
 Low – dipstick may have ketones from starvation but not spilling glucose (Rx with D50W or glucagon emergency kit) Usually need to call EMS in either situation.")
74
Diabetic Athletes Jay Cutler Arthur Ashe Ty Cobb Scott Verplank
Jackie Robinson Joe Frazier Billie Jean King Joe Gibbs

75
What EMS should have: Airway equipment and supplies
Portable pulse oximeter End tidal CO2 detector Manual defibrillator/cardiac monitor ACLS drugs RSI drugs if trained MD or state allows EMS to use Steroids if you use them for SCI ?Oversize backboard for football Don’t assume that they have things!

77
What you should have Airway plan – LMA, #11 blade, curved hemostats
Breathing plan – 14 gauge angiocath, extra inhaler, Flow Meter, Epi(1:1000) Cardiac plan – know how to use AED Disaster plan – be familiar with EAP Procedure plan – know who should and who can do what procedure Transport plan – appropriate facility
 Cardiac plan – know how to use AED. Disaster plan – be familiar with EAP. Procedure plan – know who should and who can do what procedure. Transport plan – appropriate facility.")
78
EMS Relationship Work closely with them
Preseason practice of scenarios Let them know what is expected of them, when to come out, what to do Demand consistency in staffing Require their best trained personnel

80
Who should do what Paramedics can intubate
Only physicians can do surgical airway Only physicians can needle decompress tension pneumothorax ATC’s, MD’s, coaches, anyone with training can use AED EMT-Basic has limited training and experience in the life threatening situations

85
Questions Life threatening athlete situations exist in almost every sport Always know who is in charge Always know who is best trained for a particular incident Always be prepared and be resourceful if unusual situations arise

Similar presentations








































 Muscular organ (fist size) Functions like a pump Functions like a pump Protected.>")







, Chief Medical Officer Pop Warner Football, Medical.>")
