Download presentation
Presentation is loading. Please wait.

1
N BME REVIEW. G. I : ANATOMY. By Dr Abiodun Mark Akanmode.

2
INTRODUCTION: S URFACE ANATOMY. The abdomen is the region of the trunk that lies between the diaphragm above and the inlet of the pelvis below.

3
M USCLES AND FASCIA OF ANTERIOR BODY WALL. 1.Skin 2. Superficial fascia a. Camper (fatty) b. Scarpa (fibrous) 3. External oblique 4. Internal oblique 5. Transversus abdominis 6. Transversalis fascia 7. Extra peritoneal 8.Parietal peritoneum
 b. Scarpa (fibrous) 3. External oblique 4. Internal oblique 5. Transversus abdominis 6. Transversalis fascia 7. Extra peritoneal 8.Parietal peritoneum.")
4
L ONGITUDINAL SECTION OF THE ABDOMINAL LAYERS.

5
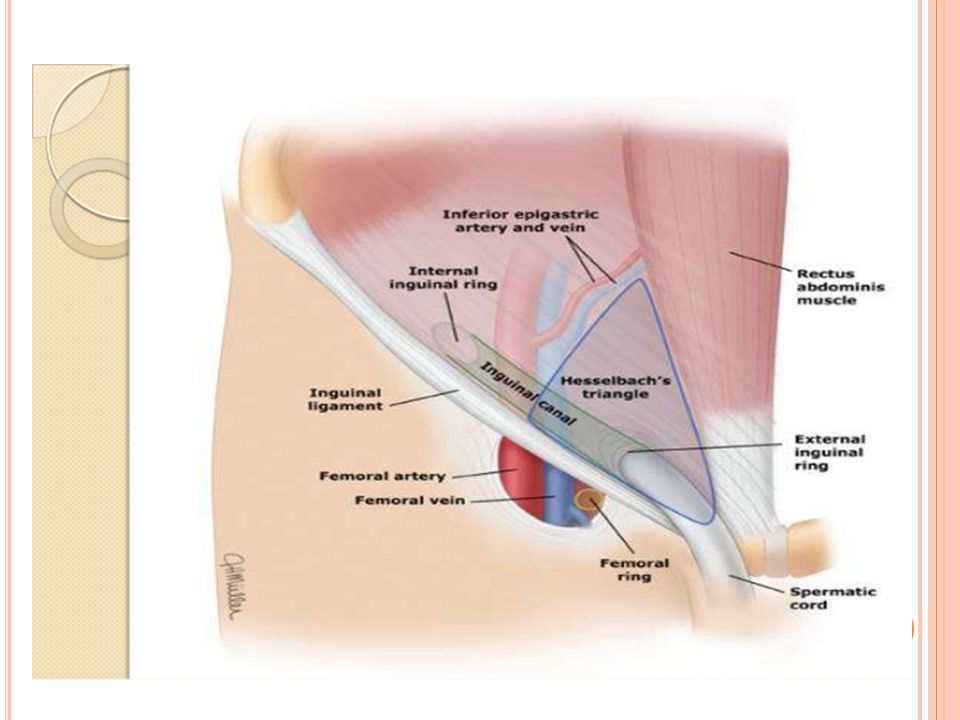
I NGUINAL REGION & CANAL. The inguinal canal is the oblique passage way (approximately 4 cm long) in the lower aspect of the anterior abdominal wall. Clinically, the inguinal region is important because it is the area where inguinal hernias occur. The entrance of the canal is via the superficial inguinal ring and the deep inguinal ring, located just lateral to the inferior epigastric vessel. The superficial inguinal ring is the medial opening of the canal superior to the pubic tubercle
 in the lower aspect of the anterior abdominal wall. Clinically, the inguinal region is important because it is the area where inguinal hernias occur. The entrance of the canal is via the superficial inguinal ring and the deep inguinal ring, located just lateral to the inferior epigastric vessel. The superficial inguinal ring is the medial opening of the canal superior to the pubic tubercle.")
6
B OUNDARIES OF THE INGUINAL CANAL. Roof :Formed by muscle fibers of the internal abdominal oblique and the transverse abdominis muscles. Anterior wall: Formed by aponeurosis of the external abdominal oblique and the internal abdominal oblique muscle laterally. Floor: Formed by inguinal ligament and the lacunar ligament at the medial end. Posterior wall : The posterior wall is divided into lateral and medial areas a)medial area: formed by conjoint tendon. b)lateral area: formed by transversalis muscle.
medial area: formed by conjoint tendon. b)lateral area: formed by transversalis muscle..")
7
C ONTENT OF THE INGUINAL CANAL. Female inguinal canal: a) Round ligament of the uterus b) Ilioinguinal nerve l1. Male inguinal canal: a) Ilioinguinal nerve L1. b) Spermatic cord: T esticular artery. P ampiniform plexus. V as deferens. A utonomic nerves. L ymphatics.
 Round ligament of the uterus b) Ilioinguinal nerve l1. Male inguinal canal: a) Ilioinguinal nerve L1. b) Spermatic cord: T esticular artery. P ampiniform plexus. V as deferens. A utonomic nerves. L ymphatics..")
8
I NGUINAL HERNIA. Hernia is a protrusion of peritoneum through an opening, usually a site of weakness. Inguinal hernias are the most common of the abdominal hernias and occur more frequently in males due to the inherent weakness of the male inguinal canal. Indirect inguinal hernia : goes through the deep, superficial inguinal ring into the scrotum and its covered by all 3 layers of the spematic fascia. It enters the deep inguinal ring lateral to the epigastric vessels. Direct inguinal hernia: goes through the inguinal triangle and superficial inguinal ring only. Its covered only by the external spermatic fascia.

10
F ASCIA LAYER OF THE SPERMATIC CORD. There are 3 fascia components derived from the layers of the abdomen that surround the spermatic cord. External spermatic fascia is formed by the aponeuroses of the external abdominal oblique muscle at the superficial ring. Middle or cremasteric muscle and fascia are formed by fibers of the internal abdominal oblique within the inguinal canal. Internal spermatic fascia is formed by the transversalis fascia at the deep ring.

11
T ESTICULAR DESCENT. The testis develops from the mesoderm of the urogenital ridge. During the last trimester, the testis descends the posterior abdominal wall inferiorly toward the deep inguinal ring guided by the fibrous gubernaculum. An evagination of the parietal peritoneum and the peritoneal cavity extends into the inguinal canal called the processus vaginalis The open connection of the processus vaginalis with the peritoneal cavity closes before birth. A portion of the processus vaginalis remains patent in the scrotum and surrounds the testis as the tunica vaginalis.

14
P ERITONEUM. The peritoneum is the serous membrane related to the viscera of the abdominal cavity. It is divided into 2 layers: parietal and visceral. Parietal Layer: The parietal layer lines the body wall and covers the retroperitoneal organs on one surface. Visceral Layer: The visceral layer encloses the surfaces of the intraperitoneal organs.

15
PERITONEAL CAVITY The peritoneal cavity is the potential space located between the parietal and visceral peritoneal layers. It is filled with thin serous fluid secreted by mesothelial cells. The lesser sac (omental bursa) is a cul-de-sac formed posterior to the stomach and the lesser omentum. The greater sac is formed by the larger area of the remaining peritoneal cavity. The only communication between the lesser sac and the greater sac is the epiploic foramen (of Winslow).
 is a cul-de-sac formed posterior to the stomach and the lesser omentum. The greater sac is formed by the larger area of the remaining peritoneal cavity. The only communication between the lesser sac and the greater sac is the epiploic foramen (of Winslow)..")
16
I NTRAPERITONEAL VS RETROPERITONEAL ORGANS. Intraperitoneal organs are suspended by a mesentery and are almost completely enclosed in visceral peritoneum. These organs are mobile. Retroperitoneal organs are partially covered on one side with parietal peritoneum and are immobile or fixed organs

17
P ERITONEAL ORGANS. Stomach Liver and gallbladder Spleen Duodenum, 1st part Tail of pancreas Jejunum Ileum Appendix Transverse colon Sigmoid colon Kidneys Adrenal glands Ureters Aorta lnferior vena cava Lower rectum Anal canal. Pancreas(H,N &B) Intraperitoneal organs.Retroperitoneal organs.
 Intraperitoneal organs.Retroperitoneal organs..")
18
EPILOIC FORAMEN OF WINSLOW. The epiploic foramen is the opening between lesser sac and greater peritoneal sac. The boundaries are made up of: Anteriorly: Hepatoduodenal ligament and the hepatic portal vein Posteriorly: Inferior vena cava Superiorly: Caudate lobe of the liver Inferiorly: First part of the duodenum

20
ABDOMINAL VISCERALS : L IVER. The liver has 2 surfaces: a superior or diaphragmatic surface and an inferior or a visceral surface. lt lies mostly in the right aspect of the abdominal cavity and is protected by the rib cage. The liver is traditionally divided into 2 lobes of unequal sizes as viewed from the front (diaphragmatic) surface. The visceral surface shows it to be divided into four lobes and includes the caudate and quadrate lobes The liver has a central hilus, or porta hepatis, which receives venous blood from the portal vein and arterial blood from the hepatic artery.
 surface. The visceral surface shows it to be divided into four lobes and includes the caudate and quadrate lobes The liver has a central hilus, or porta hepatis, which receives venous blood from the portal vein and arterial blood from the hepatic artery..")
23
ABDOMINAL VISCERALS : GALLBLADDER : The gallbladder lies in a fossa on the visceral surface of the liver to the right of the quadrate lobe. It stores and concentrates bile, which enters and leaves through the cystic duct.

24
ABDOMINAL VISCERALS : PANCREAS. The pancreas horizontally crosses the posterior abdominal wall at approximately at the level of the transpyloric plane. The gland consists of 4 parts: head, neck, body, and tail. The head of the pancreas receives its blood supply from the superior and inferior pancreaticoduodenal branches. The neck, body, and tail of the pancreas receive their blood supply from the splenic artery.

25
ABDOMINAL VISCERALS The stomach has a right lesser curvature, which is connected to the porta hepatis of the liver by the lesser omentum (hepatogastric ligament) The left greater curvature from which the greater omentum is suspended The spleen is a peritoneal organ in the upper left quadrant that is deep to the left 9th, 10th, and 1 1th ribs. The visceral surface of the spleen is in contact with the left colic flexure, stomach, and left kidney. STOMACHSPLEEN.

26
ABDOMINAL VISCERALS : SMALL INTESTINE. The duodenum is C- shaped. The duodenum is a hollow jointed tube about 25–38 cm (10–15 inches) long connecting the stomach to the jejunum.
 long connecting the stomach to the jejunum..")
27
ABDOMINAL VISCERALS : SMALL INTESTINE. The jejunum begins at the duodenojejunal junction and comprises 2/5 of the remaining small intestine. The beginning of the ileum is not dearly demarcated; it consists of the distal 3/5 of the small bowel.

28
ABDOMINAL VISCERALS : COLON. The colon or large intestine is made up of the following parts: Cecum. Ascending colon. Transverse colon. Descending colon. Sigmoid colon. Rectum.

29
A NAL CANAL : The anal canal is about 1.5 inches long and opens distally at the anus. The anal canal is divided in an upper and lower parts separated by the pectinate line. The internal anal sphincter is circular smooth muscle that surrounds the anal canal. The external anal sphincter is circular voluntary skeletal muscle

31
C OMPARISON OF F EATURES A BOVE AND B ELOW THE P ECTINATE L INE Visceral (ANS) sensory innervation. Portal venous drainage. Internal hemorrhoids (pain less) Endoderm. Drain to iliac lymph nodes Somatic sensory innervation. Caval venous drainage. External hemorrhoids (painful) Ectoderm. Drain to superficial inguinal nodes ABOVEBELOW
 Endoderm. Drain to iliac lymph nodes Somatic sensory innervation. Caval venous drainage. External hemorrhoids (painful) Ectoderm. Drain to superficial inguinal nodes ABOVEBELOW.")
32
A RTERIAL SUPPLY TO THE ABDOMINAL VISCERALS. The blood supply to the abdominal viscera and the body wall is provided by branches of the abdominal aorta

35
I MAGING STUDIES OF THE G. I

Similar presentations