Download presentation
Presentation is loading. Please wait.

2
GOLD Update 2011 Rabab A. El Wahsh, MD. Lecturer of Chest Diseases and Tuberculosis Minoufiya University REVISED 2011

3
Global Initiative for chronic obstructive pulmonary disease (GOLD) Immediately following the release of the first GOLD report in 2001, the GOLD board of directors appointed a science committee, charged with keeping the GOLD documents up to date. The first update to the GOLD report was in 2003, then annual updated documents were prepared and released on the GOLD website. A comprehensively updated version was released in 2006, then in 2010 and lastly in 2011.

4
What`s new in GOLD 2011? The definition of COPD was not significantly modified but has been reworded for clarity. Assessment of COPD is based on the patient`s level of symptoms, future risk of exacerbations, the severity of spirometric abnormlity, and the identification of comorbidities. Management of stable COPD is based, not only on level of FEV1 but on disease impact and future risk of disease progression. More focusing on comorbidities.

5
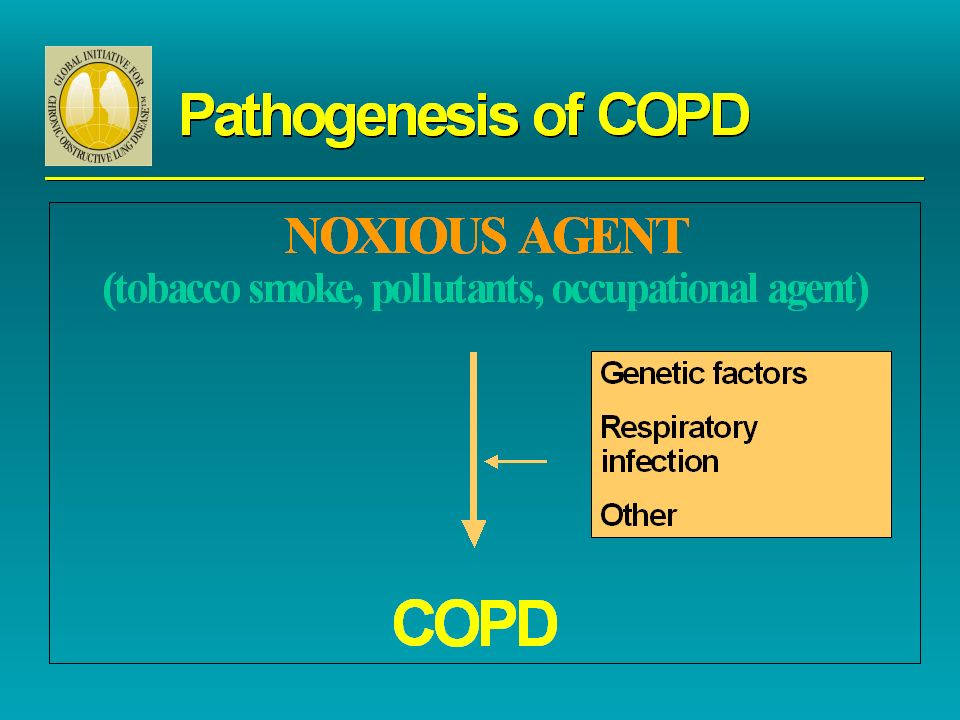
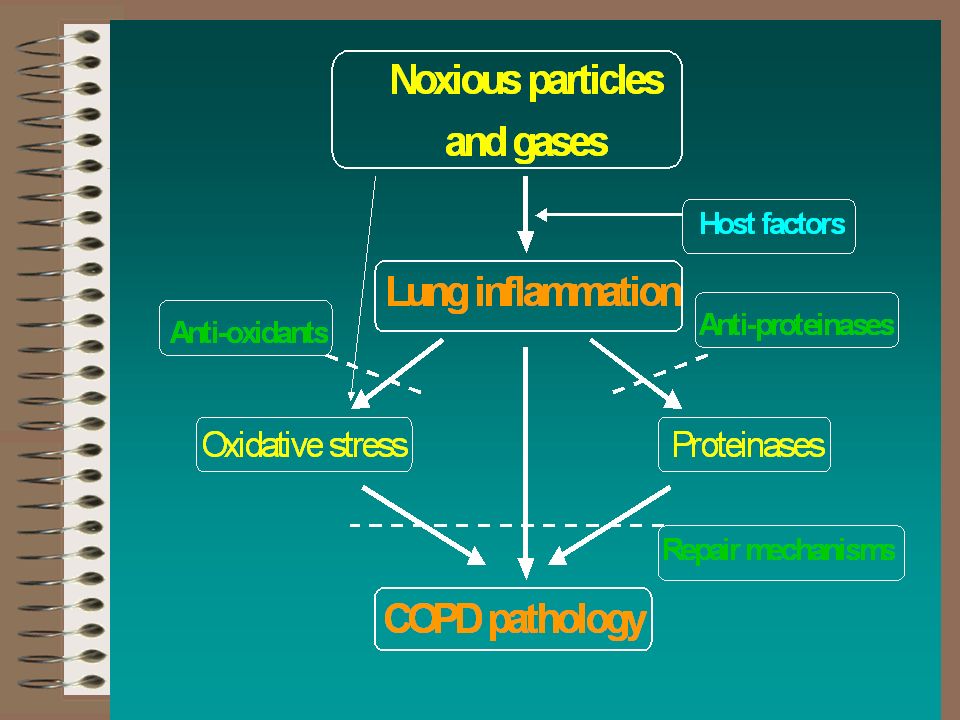
COPD Definition GOLD 2010 Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease with some significant extrapulmonary effects that may contribute to the severity in individual patients. Its pulmonary component is characterized by airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases. GOLD 2011 Chronic obstructive pulmonary disease (COPD), a common preventable and treatable disease is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients.
, a common preventable and treatable disease is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients..")
6
Risk Factors for COPD Genes Infections Socio-economic status Aging Populations

10
Diagnosis and Assessment of COPD GOLD 2010GOLD 2011

11
While post-bronchodilator spirometry is required for the diagnosis and assessment of severity of COPD, the degree of reversibility of airflow limitation is no longer recommended. The degree of reversibility has never been shown to add to the diagnosis, differential diagnosis with asthma, or to predicting the response to long-term treatment with bronchodilators or corticosteroids. The use of a fixed ratio FEV1/FVC to define airflow limitation will result in more frequent diagnosis of COPD in the elderly, and less frequent diagnosis in adults younger than 45 years, especially of mild disease, compared to using a cutoff based on the lower limit of normal values for FEV1/FVC. From a scientific perspective it is difficult to determine which of these criteria is correct to diagnose COPD. Diagnosis and Assessment of COPD

12
SYMPTOMS chronic cough shortness of breath EXPOSURE TO RISK FACTORS tobacco occupation indoor/outdoor pollution SPIROMETRY: Required to establish diagnosis Diagnosis of COPD sputum

13
Assessment of GOLD stage using spirometry (GOLD 2010) In patients with FEV 1 /FVC < 0.70: GOLD 1: Mild FEV 1 > 80% predicted GOLD 2: Moderate 50% < FEV 1 < 80% predicted GOLD 3: Severe 30% < FEV 1 < 50% predicted GOLD 4: Very Severe FEV 1 < 30% predicted *Based on Post-Bronchodilator FEV 1
 In patients with FEV 1 /FVC < 0.70: GOLD 1: Mild FEV 1 > 80% predicted GOLD 2: Moderate 50% < FEV 1 < 80% predicted GOLD 3: Severe 30% < FEV 1 < 50% predicted GOLD 4: Very Severe FEV 1 < 30% predicted *Based on Post-Bronchodilator FEV 1")
14
Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities Combined Assessment of COPD (GOLD 2011)
")
15
COPD Assessment Test (CAT): An 8-item measure of health status impairment in COPD. Breathlessness Measurement using the Modified British Medical Research Council (mMRC) Questionnaire: relates well to other measures of health status and predicts future mortality risk. Assessment of Symptoms
 Questionnaire: relates well to other measures of health status and predicts future mortality risk. Assessment of Symptoms.")
16
Modified MRC (mMRC)Questionnaire
Questionnaire")
17
COPD Assessment Test (CAT):
:")
18
Assessment of degree of airflow limitation using spirometry In patients with FEV 1 /FVC < 0.70: GOLD 1: Mild FEV 1 > 80% predicted GOLD 2: Moderate 50% < FEV 1 < 80% predicted GOLD 3: Severe 30% < FEV 1 < 50% predicted GOLD 4: Very Severe FEV 1 < 30% predicted *Based on Post-Bronchodilator FEV 1

19
Assessment of risk of exacerbations An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient`s respiratory symptoms that is beyond normal day-to-day variations and leads to change in medication. Two exacerbations or more within the last year or an FEV1 < 50 % of predicted value are indicators of high risk of future exacerbations.

20
Combined Assessment of COPD Risk (GOLD Classification of Airflow Limitation) Risk (Exacerbation history) > 2 1 0 (C) (D) (A) (B) mMRC 0-1 CAT < 10 4 3 2 1 mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score)) Patient is now in one of four categories: A: Less symptoms, low risk B: More symtoms, low risk C: Less symptoms, high risk D: More Symtoms, high risk
 Risk (Exacerbation history) > (C) (D) (A) (B) mMRC 0-1 CAT < mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score)) Patient is now in one of four categories: A: Less symptoms, low risk B: More symtoms, low risk C: Less symptoms, high risk D: More Symtoms, high risk")
21
Assessment of COPD Comorbidities COPD patients are at increased risk for: Cardiovascular diseases Osteoporosis Respiratory infections Anxiety and Depression Diabetes Lung cancer These comorbid conditions may influence mortality and hospitalizations and should be looked for routinely, and treated appropriately.

22
Goals for treatment of stable COPD Reduce symptoms by: Relieving symptoms Improving exercise tolerence Improving health status Reduce risk by: Preventing disease progression Preventing and treatment of exacerbation Reduction of mortality

23
Management of stable COPD 2010

24
Initial pharmacologic management of COPD (2011) Patient groupFirst choiceSecond choiceAlternative choice AShort acting anticholinergic Or Short acting B2 agonist Long acting anticholinergic Or Long acting B2 agonist Or Short acting B2 agonist and Short acting anticholinergic Theophylline BLong acting Anticholinergic Or Long acting B2 agonist Long acting Anticholinergic and Long acting B2 agonist Short acting B2 agonist and/ or Short acting anticholinergic Theophylline CInhaled corticosteroid + Long acting B2 agonist Or Long acting anticholinergic Long acting Anticholinergic and Long acting B2 agonist Phospodiesterase-4 inhibitor Short acting B2 agonist and/ or Short acting anticholinergic Theophylline DInhaled corticosteroid + Long acting B2 agonist Or Long acting anticholinergic Inhaled corticosteroid and Long acting Anticholinergic Or inhaled corticosteroid+ Long acting B2 agonist and long acting anticholinergic Or Inhaled corticosteroid + Long acting B2 agonist and phosphodiesterse-4 inhibitor Or Long acting Anticholinergic and long acting B2 agonist Or Long acting anticholinergic and phosphodiesterase-4 inhibitor Carbocysteine Short acting B2 agonist And/or Short acting anticholinergic theophylline
 Patient groupFirst choiceSecond choiceAlternative choice AShort acting anticholinergic Or Short acting B2 agonist Long acting anticholinergic Or Long acting B2 agonist Or Short acting B2 agonist and Short acting anticholinergic Theophylline BLong acting Anticholinergic Or Long acting B2 agonist Long acting Anticholinergic and Long acting B2 agonist Short acting B2 agonist and/ or Short acting anticholinergic Theophylline CInhaled corticosteroid + Long acting B2 agonist Or Long acting anticholinergic Long acting Anticholinergic and Long acting B2 agonist Phospodiesterase-4 inhibitor Short acting B2 agonist and/ or Short acting anticholinergic Theophylline DInhaled corticosteroid + Long acting B2 agonist Or Long acting anticholinergic Inhaled corticosteroid and Long acting Anticholinergic Or inhaled corticosteroid+ Long acting B2 agonist and long acting anticholinergic Or Inhaled corticosteroid + Long acting B2 agonist and phosphodiesterse-4 inhibitor Or Long acting Anticholinergic and long acting B2 agonist Or Long acting anticholinergic and phosphodiesterase-4 inhibitor Carbocysteine Short acting B2 agonist And/or Short acting anticholinergic theophylline")
25
Non-pharmacologic management of COPD (2011) Patient groupEssentialRecommendedDepending on local guidelines ASmoking cessation Physical activityFlu vaccine Pneumococcal vaccine B-DSmoking cessation Pulmonary rehabilitation Physical activityFlu vaccine Pneumococcal vaccine
 Patient groupEssentialRecommendedDepending on local guidelines ASmoking cessation Physical activityFlu vaccine Pneumococcal vaccine B-DSmoking cessation Pulmonary rehabilitation Physical activityFlu vaccine Pneumococcal vaccine")
Similar presentations




>")
:880-887. Beta-blockers may reduce.>")





 Diagnosis of COPD in primary care Educational slides based on the CKS topic.>")


 By Chris Callan 23 April 2008.>")


>")



 as:*>")
