Download presentation
Presentation is loading. Please wait.

2
By: E. Salehifar Clinical Pharmacist
COPD By: E. Salehifar Clinical Pharmacist

4
WHAT IS COPD? COPD is a preventable and treatable disease with some significant extrapulmonary effects Airflow limitation that is not fully reversible Usually progressive and associated with an abnormal inflammatory response of the lung to noxious particles or gases

5
Attention! This definition does not use the terms chronic bronchitis and emphysema and excludes asthma (reversible airflow limitation). Chronic bronchitis Cough and sputum production for at least 3 months in each of 2 consecutive years Is not necessarily associated with airflow limitation Emphysema Destruction of the alveoli, is a pathological term that is sometimes (incorrectly) used clinically and describes only one of several structural abnormalities present in patients with COPD.
 used clinically and describes only one of several structural abnormalities present in patients with COPD.")
6
Symptoms of COPD include:
Cough Sputum production Dyspnea on exertion

7
RISK FACTORS: WHAT CAUSES COPD?

8
Risk Factors Worldwide, cigarette smoking is the most commonly risk factor for COPD Total burden of inhaled particles a person encounters The genetic risk factor: severe hereditary deficiency of alpha-1 antitrypsin Occupational dusts and chemicals Indoor air pollution from biomass fuel Outdoor air pollution ( small effect in causing COPD) ↓lung growth during gestation and childhood (low birth weight, respiratory infections, etc.)
 ↓lung growth during gestation and childhood (low birth weight, respiratory infections, etc.)")
9
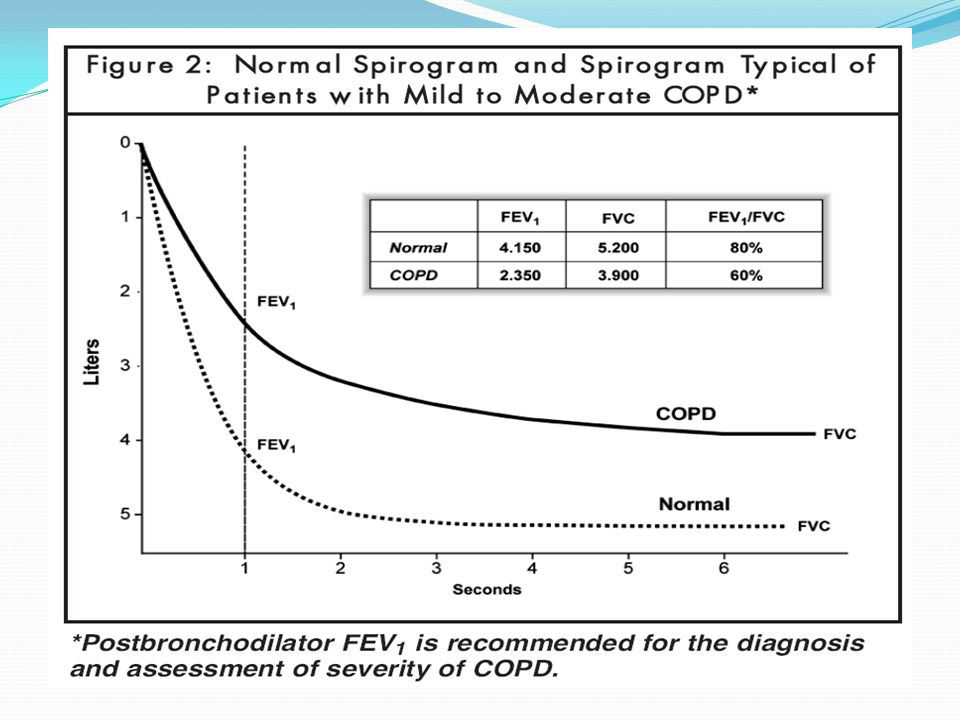
DIAGNOSING COPD Dyspnea chronic cough or sputum production
and/or a history of exposure to risk factors for the disease, especially cigarette smoking The diagnosis should be confirmed by spirometry

12
Stages of COPD Stage I: Mild COPD
FEV1/FVC < 70% ; FEV1 ≥ 80% predicted Chronic cough and sputum production May not be aware that his or her lung function is abnormal Stage II: Moderate COPD FEV1/FVC < 70%; 50% ≤ FEV1 < 80% predicted Shortness of breath typically developing on exertion Seek medical attention

13
Stages of COPD (cont.) Stage III: Severe COPD
FEV1/FVC < 70%; 30% ≤ FEV1 < 50% predicted Greater shortness of breath, reduced exercise capacity, and repeated exacerbations which have an impact on patients’ quality of life Stage IV: Very Severe COPD FEV1/FVC < 70%; FEV1 < 30% predicted or FEV1 < 50% predicted plus chronic respiratory failure Quality of life is very appreciably impaired and exacerbations may be life-threatening

16
COPD Management

17
The goals of COPD management include:
Relieve symptoms Prevent disease progression Improve exercise tolerance Improve health status Prevent and treat complications Prevent and treat exacerbations Reduce mortality Prevent or minimize side effects from treatment Cessation of cigarette smoking should be included as a goal throughout the management program

18
FOUR COMPONENTS 1. Assess and Monitor Disease 2. Reduce Risk Factors
3. Manage Stable COPD 4. Manage Exacerbations

19
Assessment Spirometry
Bronchodilator reversibility testing (to rule out asthma) Chest X – ray (TB, CHF) ABG (if FEV1 < 50% predicted or with clinical signs suggestive of respiratory failure or right heart failure) The major clinical sign of respiratory failure is cyanosis Clinical signs of right heart failure include ankle edema and an increase in the jugular venous pressure Respiratory failure: PaO2 < 60 mm Hg, with or without PaCO2 > 50 mm Hg Alpha- 1 antitrypsin (for Caucasian under 45 years or with a strong family history of COPD)
 Chest X – ray (TB, CHF) ABG (if FEV1 < 50% predicted or with clinical signs suggestive of respiratory failure or right heart failure) The major clinical sign of respiratory failure is cyanosis. Clinical signs of right heart failure include ankle edema and an increase in the jugular venous pressure. Respiratory failure: PaO2 < 60 mm Hg, with or without PaCO2 > 50 mm Hg. Alpha- 1 antitrypsin (for Caucasian under 45 years or with a strong family history of COPD)")
20
Component 2: Reduce Risk Factors
Smoking cessation Most effective and cost-effective intervention Pharmacotherapy (nicotine replacement, buproprion/nortryptiline) Cautions of pharmacotherapy: Fewer than 10 cigarettes per day Pregnant women Adolescents Medical contraindications (unstable coronary artery disease, untreated peptic ulcer, and recent MI or stroke) History of seizures for buproprion
 Cautions of pharmacotherapy: Fewer than 10 cigarettes per day. Pregnant women. Adolescents. Medical contraindications (unstable coronary artery disease, untreated peptic ulcer, and recent MI or stroke) History of seizures for buproprion.")
21
Component 3: Manage Stable COPD

22
Bronchodilators Are central to symptom management in COPD
Inhaled therapy (esp. long-acting bronchodilators) Give “as needed” to relieve intermittent or worsening symptoms, and on a regular basis to prevent or reduce persistent symptoms Beta 2-agonists, anti-cholinergics, methylxanthines, and combination therapy Combining bronchodilators Improve efficacy ↓ side effects compared to increasing the dose of a single bronchodilator
 Give as needed to relieve intermittent or worsening symptoms, and on a regular basis to prevent or reduce persistent symptoms. Beta 2-agonists, anti-cholinergics, methylxanthines, and combination therapy. Combining bronchodilators. Improve efficacy. ↓ side effects compared to increasing the dose of a single bronchodilator.")
25
Symbicort®

26
Glucocorticosteroids:
Inhaled glucocorticosteroids only for patients with FEV1 < 50% of predicted Repeated exacerbations (for example, 3 in the last three years) This treatment: ↓ frequency of exacerbations and thus improve health status Does not modify the long-term decline in FEV1 ↑ pneumonia and does not reduce overall mortality An inhaled glucocorticosteroid combined with a long-acting β2-agonist is more effective on pulmonary function test Combination therapy increases the likelihood of pneumonia and has no significant effects on mortality Long-term treatment with oral glucocorticosteroids is not recommended
 This treatment: ↓ frequency of exacerbations and thus improve health status. Does not modify the long-term decline in FEV1. ↑ pneumonia and does not reduce overall mortality. An inhaled glucocorticosteroid combined with a long-acting β2-agonist is more effective on pulmonary function test. Combination therapy increases the likelihood of pneumonia and has no significant effects on mortality. Long-term treatment with oral glucocorticosteroids is not recommended.")
27
Vaccines: Influenza vaccines Pneumococcal polysaccharide vaccine
↓ serious illness and death in COPD patients by 50% should be given once each year Pneumococcal polysaccharide vaccine Recommended for ≥ 65 years old ↓ community-acquired pneumonia in those under age 65 with FEV1 < 40% predicted

28
Antibiotics Antitussives Mucolytic Agents
Not recommended except for treatment of infectious exacerbations and other bacterial infections Antitussives Regular use contraindicated in stable COPD Mucolytic Agents Patients with viscous sputum may benefit from mucolytics, but overall benefits are very small, Use is not recommended

29
Non-Pharmacologic Treatment
Exercise training All stages of disease benefit from exercise training programs The minimum length to be effective: 6 weeks Oxygen therapy Surgical interventions

30
Oxygen Therapy: For satge IV (very severe) >15 hours per day Goal:
↑ baseline PaO2 (at least 60 mm Hg) and/or produce SaO2 at least 90%, ↑ survival Beneficial effects on pulmonary hemodynamics, hematologic characteristics, exercise capacity, lung mechanics, and mental state
 and/or produce SaO2 at least 90%, ↑ survival. Beneficial effects on pulmonary hemodynamics, hematologic characteristics, exercise capacity, lung mechanics, and mental state.")
31
Surgical Treatments Bullectomy and lung transplantation
For carefully selected patients with Stage IV No sufficient evidence that would support the widespread use of lung volume reduction surgery (LVRS)
")
33
Component 4: Manage Exacerbations

34
Exacerbation of COPD Change in the patient’s baseline dyspnea, cough, and/or sputum that is beyond normal day-o- day variations Acute in onset May warrant a change in regular medication

35
Causes The most common: Infection of the tracheobronchial tree
Air pollution But the cause of about one-third of severe exacerbations cannot be identified

36
Assessment the Severity of an Exacerbation
ABG: PaO2 < 60 mm Hg; SaO2 < 90% with or without PaCO2 > 50 mmHg Chest X-ray ECG Other laboratory tests: Sputum culture and antibiogram to identify infection if there is no response to initial antibiotic treatment Biochemical tests to detect electrolyte disturbances, diabetes, and poor nutrition Whole blood count can identify polycythemia or bleeding

38
Antibiotics Should be given to patients: ↑ Dyspnea
↑ increased sputum volume, ↑ sputum purulence Who require mechanical ventilation

39
Visit the GOLD Website at www.goldcopd.org
Where to find more detailed in formation on spirometry 1. American Thoracic Society 2. Australian/New Zealand Thoracic Society 3. British Thoracic Society

Similar presentations









>")








 By Chris Callan 23 April 2008.>")

>")






 Professor Bill MacNee>")