Download presentation
Presentation is loading. Please wait.

1
Psychological Disorders
Chapter 14 Psychological Disorders

2
The system used by psychologists to classify psychological disorders is the:
APA Clinical Handbook b. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) c. Physician's Desk Reference (PDR) d. Encyclopedia of Psychological Disorders
 c. Physician s Desk Reference (PDR) d. Encyclopedia of Psychological Disorders.")
3
Posttraumatic stress disorder is characterized by
recurrent, sudden and unexpected attacks of overwhelming anxiety b. enduring psychological disturbances attributed to the experience of a major traumatic event c. a chronic high level of anxiety d. persistent and irrational fear of an object or situation

4
Your friend's mother is afraid of squirrels
Your friend's mother is afraid of squirrels. While she knows squirrels are basically harmless, she cannot control her anxiety when she sees either a real squirrel or a picture of a squirrel. She never took your friend to the local park when he was a child because of the numerous squirrels. Your friend's mother has: a. panic disorder b. conversion disorder c. generalized anxiety disorder d. phobic disorder

5
ANSWERS: B D

6
Rate this person using the following scale: 1= Basically OK Psychotherapy is not necessary 2=Mild Disturbance. Psychotherapy should be considered 3= Significant disturbance. Psychotherapy is definitely required 4= Severe disturbance. Hospitalize! Larry, a homosexual who has lived for three years with a man he met in graduate school, works as a psychologist in a large hospital. Although competent in his work, he often feels strained by the pressures of his demanding position. An added source of tension on the job is his not being able to confide in all his co workers about his private life. Most of his leisure activities are with good friends who belong to the gay subculture.

7
Rate this person using the following scale: 1= Basically OK Psychotherapy is not necessary 2=Mild Disturbance. Psychotherapy should be considered 3= Significant disturbance. Psychotherapy is definitely required 4= Severe disturbance. Hospitalize! Bob is a very intelligent, 25 year old member of a religious organization that is based on Buddhism. Bob’s working for this organization caused considerable conflict between him and his parents, who are devout Catholics. Recently Bob experiences acute spells of nausea and fatigue that prevent him from working and which have forced him to return home to live with his parents. Various medical tests are being conducted, but as yet no physical causes of his problems have been found.

8
Rate this person using the following scale: 1= Basically OK Psychotherapy is not necessary 2=Mild Disturbance. Psychotherapy should be considered 3= Significant disturbance. Psychotherapy is definitely required 4= Severe disturbance. Hospitalize! Jim was vice president of the freshman class at a local college and played on the school’s football team. Later that year he dropped out of these activities and gradually became more and more withdrawn from friends and family. Neglecting to shave and shower, he began to look dirty and unhealthy. He spent most of his time alone in his room and sometimes complained to his parents that he heard voices in the curtains and in the closet. In his sophomore year he dropped out of school entirely. With increasing anxiety and agitation, he began to worry that the “Nazis” were plotting to kill his family and kidnap him.

9
Rate this person using the following scale: 1= Basically OK Psychotherapy is not necessary 2=Mild Disturbance. Psychotherapy should be considered 3= Significant disturbance. Psychotherapy is definitely required 4= Severe disturbance. Hospitalize! Mary is a 30 year old musician who is very dedicated and successful in her work as a teacher in a local high school and as a part time member of local musical groups. Since her marriage five years ago, which ended in divorce after six months, she has dated very few men. She often worries that her time is “running out” for establishing a good relationship with a man, getting married, and raising a family. Her friends tell her that she gets way too anxious around men, and that she needs to relax a little in general.

10
Abnormal Behavior The medical model What is abnormal behavior?
3 criteria Deviant Maladaptive Causing personal distress A continuum of normal/abnormal diathesis-stress model genetic predisposition to a disorder, and poor environment (learning) in childhood, and severe stress explains causality for disorders The medical model proposes that it is useful to think of abnormal behavior as a disease…Thomas Szasz and others argue against this model, contending that psychological problems are “problems in living,”rather than psychological problems. In determining whether a behavior is abnormal, clinicians rely on the following criteria: 1. Is it deviant, or does it violate societal norms, 2. Is it maladaptive, that is, does it impair a person’s everyday behavior, and 3. Does it cause them personal distress? All three criteria do not have to be met for a person to be diagnosed with a psychological disorder…diagnoses involve value judgments. Antonyms such as normal vs. abnormal imply that people can be divided into two distinct groups, when in reality, it is hard to know when to draw the line.
 in childhood, and. severe stress. explains causality for disorders. The medical model proposes that it is useful to think of abnormal behavior as a disease…Thomas Szasz and others argue against this model, contending that psychological problems are problems in living, rather than psychological problems. In determining whether a behavior is abnormal, clinicians rely on the following criteria: 1. Is it deviant, or does it violate societal norms, 2. Is it maladaptive, that is, does it impair a person’s everyday behavior, and 3. Does it cause them personal distress All three criteria do not have to be met for a person to be diagnosed with a psychological disorder…diagnoses involve value judgments. Antonyms such as normal vs. abnormal imply that people can be divided into two distinct groups, when in reality, it is hard to know when to draw the line.")
12
Prevalence, Causes, and Course
Epidemiology - study of the distribution of mental or physical disorders in the population Prevalence Lifetime prevalence Diagnosis Etiology - refers to the apparent causation and developmental history of an illness Prognosis - is a forecast about the probable course of an illness Epidemiology is the study of the distribution of mental or physical disorders in the population. Prevalence refers to the percentage of a population that exhibits a disorder during a specified time period. Lifetime prevalence is the percentage of people who have been diagnosed with a specific disorder at any time in their lives. Current research suggests that about 44% of the adult population will have some sort of psychological disorder at some point in their lives. A diagnosis is a means of distinguishing one illness from another. Etiology refers to the apparent causation and developmental history of an illness, while prognosis is a forecast about the probable course of an illness.

14
Psychodiagnosis: The Classification of Disorders
American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders – 4th ed. (DSM - 4) Multiaxial system 5 axes or dimensions Axis I – Clinical Syndromes Axis II – Personality Disorders or Mental Retardation Axis III – General Medical Conditions Axis IV – Psychosocial and Environmental Problems Axis V – Global Assessment of Functioning A taxonomy of mental disorders was first published in 1952 by the American Psychiatric Association - the DSM. This classification scheme is now in its 4th revision, which uses a multiaxial system for classifying mental disorders. The diagnoses of disorders are made on Axes I and II, with most falling on Axis I. The remaining axes are used to record supplemental information. A person’s physical disorders are listed on Axis III, and the types of stress they have experienced in the past year on Axis IV. Axis V estimates the individual’s current level of adaptive functioning. The goal of this multiaxial system is to impart information beyond a traditional diagnostic label.
 Multiaxial system. 5 axes or dimensions. Axis I – Clinical Syndromes. Axis II – Personality Disorders or Mental Retardation. Axis III – General Medical Conditions. Axis IV – Psychosocial and Environmental Problems. Axis V – Global Assessment of Functioning. A taxonomy of mental disorders was first published in 1952 by the American Psychiatric Association - the DSM. This classification scheme is now in its 4th revision, which uses a multiaxial system for classifying mental disorders. The diagnoses of disorders are made on Axes I and II, with most falling on Axis I. The remaining axes are used to record supplemental information. A person’s physical disorders are listed on Axis III, and the types of stress they have experienced in the past year on Axis IV. Axis V estimates the individual’s current level of adaptive functioning. The goal of this multiaxial system is to impart information beyond a traditional diagnostic label.")
15
The DSM multiaxial system
Figure 14.4 – Example multiaxial evaluation

16
Axis I Clinical Syndromes Discussed in Text
Anxiety Disorders Somatoform Disorders Dissociative Disorders Mood Disorders Schizophrenic Disorders The clinical syndromes discussed at length in the text are listed on this slide as an overview and are covered individually on the following slides.

17
Clinical Syndromes: Anxiety Disorders
Generalized anxiety disorder “free-floating anxiety” Phobic disorder Specific focus of fear Panic disorder and agoraphobia Physical symptoms of anxiety/leading to agoraphobia Obsessive compulsive disorder Obsessions Compulsions The anxiety disorders are a class of disorders marked by feelings of excessive apprehension and anxiety. Generalized anxiety disorder is marked by a chronic, high level of anxiety that is not tied to any specific threat…”free-floating anxiety.” Phobic disorder is marked by a persistent an irrational fear of an object or situation that presents no realistic danger. Particularly common are acrophobia – fear of heights, claustrophobia – fear of small, enclosed places, brontophobia – fear of storms, hydrophobia – fear of water, and various animal and insect phobias. Panic disorder is characterized by recurrent attacks of overwhelming anxiety that usually occur suddenly and unexpectedly. These paralyzing attacks have physical symptoms. After a number of these attacks, victims may become so concerned about exhibiting panic in public that they may be afraid to leave home, developing agoraphobia or a fear of going out in public. Obsessive-compulsive disorder (OCD) is marked by persistent, uncontrollable intrusions of unwanted thoughts (obsessions) and urges to engage in senseless rituals (compulsions). Obsessions often center on inflicting harm on others, personal failures, suicide, or sexual acts. Common examples of compulsions include constant handwashing, repetitive cleaning of things that are already clean, and endless checking and rechecking of locks, etc.
 is marked by persistent, uncontrollable intrusions of unwanted thoughts (obsessions) and urges to engage in senseless rituals (compulsions). Obsessions often center on inflicting harm on others, personal failures, suicide, or sexual acts. Common examples of compulsions include constant handwashing, repetitive cleaning of things that are already clean, and endless checking and rechecking of locks, etc.")
18
Post-Traumatic Stress Disorder
Post-Traumatic Stress Disorder Traumatic stress (experiencing or witnessing severely threatening, uncontrollable events with a sense of fear, helplessness, or horror) can produce PTSD, symptoms of which include haunting memories and nightmares, numbed social withdrawal, jumpy anxiety, and insomnia.
 can produce PTSD, symptoms of which include haunting memories and nightmares, numbed social withdrawal, jumpy anxiety, and insomnia.")
20
Anxiety Disorders Common and uncommon fears

21
Anxiety Disorders

22
Anxiety Disorders PET Scan of brain of person with Obsessive/ Compulsive disorder High metabolic activity (red) in frontal lobe areas involved with directing attention
 in frontal lobe areas involved with directing attention.")
23
Etiology of Anxiety Disorders
Biological factors Genetic predisposition, anxiety sensitivity GABA circuits in the brain Conditioning and learning Acquired through classical conditioning or observational learning Maintained through operant conditioning Cognitive factors Judgments of perceived threat Personality Neuroticism Stress A precipitator Twin studies suggest a moderate genetic predisposition to anxiety disorders. They may be more likely in people who are especially sensitive to the physiological symptoms of anxiety. Abnormalities in neurotransmitter activity at GABA synapses have been implicated in some types of anxiety disorders, and abnormalities in serotonin synapses have been implicated in panic and obsessive-compulsive disorders. Many anxiety responses, especially phobias, may be caused by classical conditioning and maintained by operant conditioning. Parents who model anxiety may promote the development of these disorders through observational learning. Cognitive theories hold that certain styles of thinking, overinterpreting harmless situations as threatening, for example, make some people more vulnerable to anxiety disorders. The personality trait of neuroticism has been linked to anxiety disorders, and stress appears to precipitate the onset of anxiety disorders.

28
Somatoform disorders are a class of psychological disorders characterized by
emotional disturbances of varied kinds that may spill over to disrupt physical, perceptual, social, and thought processes b. delusions, hallucinations, disorganized speech, and deterioration of adaptive behavior c. physical ailments that cannot be fully explained by organic conditions d. feelings of excessive apprehension and worry

29
The psychological disorder that involves the coexistence in one person of
two or more largely complete, and usually very different, personalities is a. schizophrenic disorder b. dissociative identity disorder c. dissociative fugue d. dissociative amnesia

30
The psychological disorder characterized by separate episodes of
depression and mania is a. bipolar disorder b. posttraumatic stress disorder c. schizophrenic disorder d. major depressive disorder

31
ANSWERS: C B A

32
Clinical Syndromes: Somatoform Disorders
Somatization Disorder - is marked by a history of diverse physical complaints that appear to be psychological in origin. They occur mostly in women and often coexist with depression and anxiety disorders. Conversion Disorder - significant loss of physical function (with no apparent organic basis), usually in a single organ system…loss of vision, partial paralysis, mutism, etc…glove anesthesia, for example, is neurologically impossible. Hypochondriasis - excessive preoccupation with health concerns and incessant worry about developing physical illnesses. Etiology Reactive autonomic nervous system Personality factors Cognitive factors The sick role Somatoform disorders are physical ailments that cannot be explained by organic conditions. They are not psychosomatic diseases, which are real physical ailments caused in part by psychological factors. (Recall from chapter 13 that psychosomatic disease as a category has fallen into disuse). Individuals with somatoform disorders are not simply faking an illness, which would be termed malingering. Somatization disorder is marked by a history of diverse physical complaints that appear to be psychological in origin. They occur mostly in women and often coexist with depression and anxiety disorders. Conversion disorder is characterized by a significant loss of physical function (with no apparent organic basis), usually in a single organ system…loss of vision, partial paralysis, mutism, etc…glove anesthesia, for example, is neurologically impossible. Hypochondriasis is characterized by excessive preoccupation with health concerns and incessant worry about developing physical illnesses. Somatoform disorders often emerge in people with highly suggestible, histrionic personalities and in people who focus excess attention on their physiological processes. They may be learned avoidance strategies, reinforced by attention and sympathy.
, usually in a single organ system…loss of vision, partial paralysis, mutism, etc…glove anesthesia, for example, is neurologically impossible. Hypochondriasis - excessive preoccupation with health concerns and incessant worry about developing physical illnesses. Etiology. Reactive autonomic nervous system. Personality factors. Cognitive factors. The sick role. Somatoform disorders are physical ailments that cannot be explained by organic conditions. They are not psychosomatic diseases, which are real physical ailments caused in part by psychological factors. (Recall from chapter 13 that psychosomatic disease as a category has fallen into disuse). Individuals with somatoform disorders are not simply faking an illness, which would be termed malingering. Somatization disorder is marked by a history of diverse physical complaints that appear to be psychological in origin. They occur mostly in women and often coexist with depression and anxiety disorders. Conversion disorder is characterized by a significant loss of physical function (with no apparent organic basis), usually in a single organ system…loss of vision, partial paralysis, mutism, etc…glove anesthesia, for example, is neurologically impossible. Hypochondriasis is characterized by excessive preoccupation with health concerns and incessant worry about developing physical illnesses. Somatoform disorders often emerge in people with highly suggestible, histrionic personalities and in people who focus excess attention on their physiological processes. They may be learned avoidance strategies, reinforced by attention and sympathy.")
34
Clinical Syndromes: Dissociative Disorders
Dissociative amnesia - sudden loss of memory for important personal information that is too extensive to be due to normal forgetting. Memory loss may be for a single traumatic event or for an extended time period around the event Dissociative fugue - is when people lose their memory for their entire lives along with their sense of personal identity…forget their name, family, where they live, etc., but still know how to do math and drive a car Dissociative identity disorder Etiology severe emotional trauma during childhood Controversy Media creation? Dissociative disorders are a class of disorders in which people lose contact with portions of their consciousness or memory, resulting in disruptions in their sense of identity. Dissociative amnesia is a sudden loss of memory for important personal information that is too extensive to be due to normal forgetting. Memory loss may be for a single traumatic event or for an extended time period around the event. Dissociative fugue is when people lose their memory for their entire lives along with their sense of personal identity…forget their name, family, where they live, etc., but still know how to do math and drive a car. Dissociative identity disorder (formerly multiple personality disorder) involves the coexistence in one person of two or more largely complete, and usually very different, personalities. DID is related to severe emotional trauma that occurred in childhood, although this link is not unique to DID, as a history of child abuse elevates the likelihood of many disorders, especially among females. Some theorists believe that people with DID are engaging in intentional role playing to use an exotic mental illness as a face-saving excuse for their personal failings and that therapists may play a role in their development of this pattern of behavior, others argue to the contrary. In a recent survey, only ¼ of American psychiatrists in the sample indicated that they felt there was solid evidence for the scientific validity of DID.
 involves the coexistence in one person of two or more largely complete, and usually very different, personalities. DID is related to severe emotional trauma that occurred in childhood, although this link is not unique to DID, as a history of child abuse elevates the likelihood of many disorders, especially among females. Some theorists believe that people with DID are engaging in intentional role playing to use an exotic mental illness as a face-saving excuse for their personal failings and that therapists may play a role in their development of this pattern of behavior, others argue to the contrary. In a recent survey, only ¼ of American psychiatrists in the sample indicated that they felt there was solid evidence for the scientific validity of DID.")
35
Clinical Syndromes: Mood Disorders
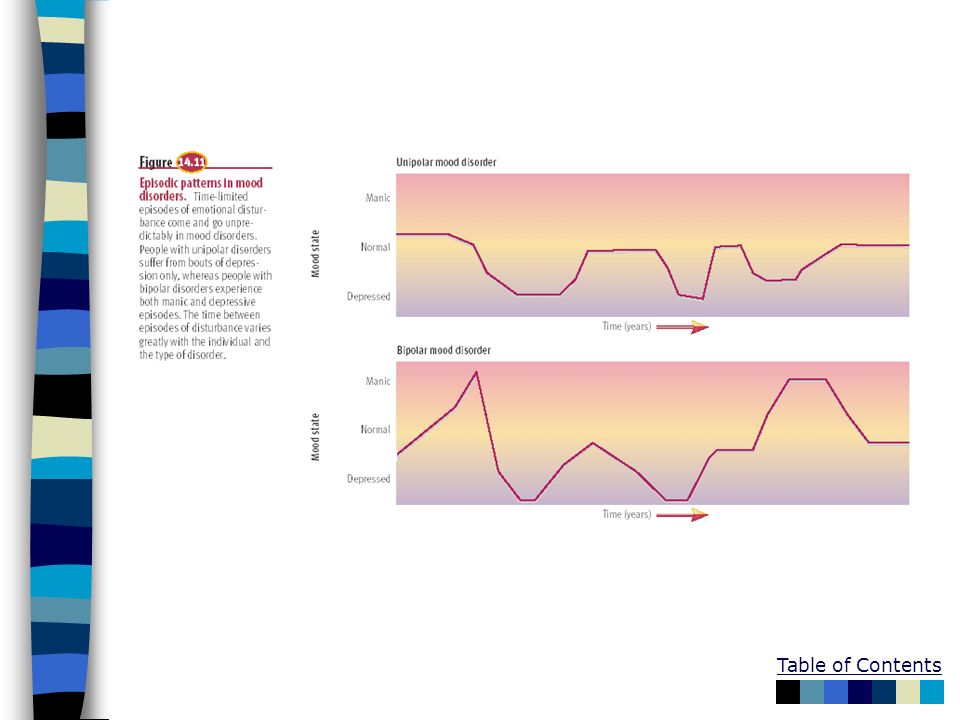
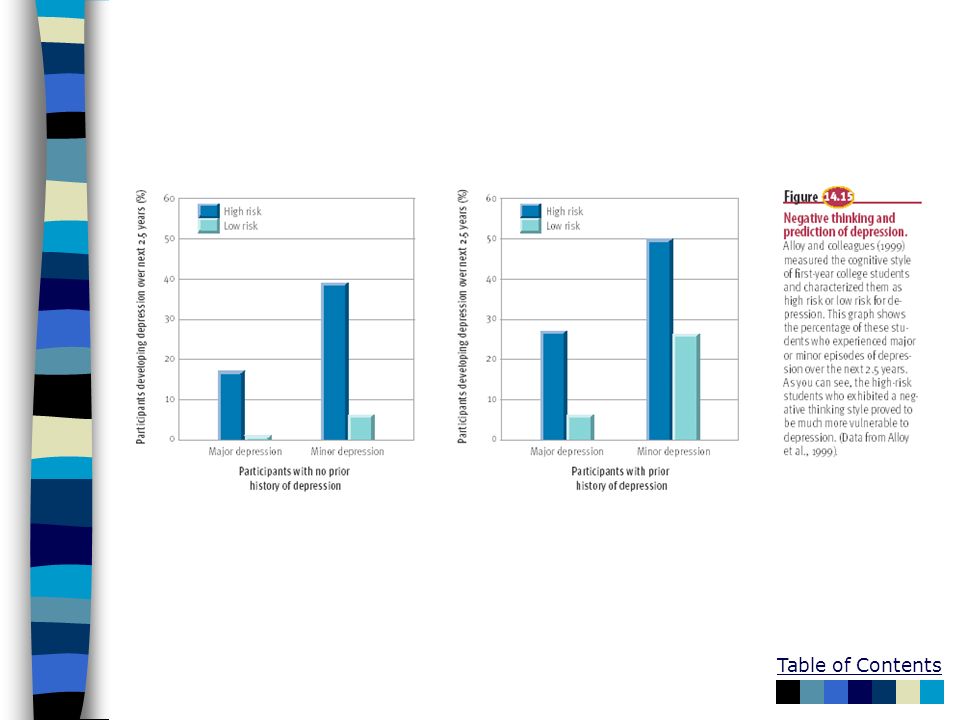
Major depressive disorder Dysthymic disorder Bipolar disorder (manic-depressive disorder) Cyclothymic disorder Etiology Genetic vulnerability Neurochemical factors - norepinephrine and serotonin synapses Cognitive factors - pessimistic explanatory Interpersonal roots - poor social skills Precipitating stress 2X as high in women Mood disorders are a class of disorders marked by emotional disturbances of varied kinds that may spill over to physical, perceptual, social, and thought processes. Major depressive disorder is marked by profound sadness, slowed thought processes, low self-esteem, and loss of interest in previous sources of pleasure. Major depression is also called unipolar depression. Research suggests that the lifetime prevalence rate of unipolar depression is between 7 and 18%. Evidence suggests that the prevalence of depression is increasing, particularly in more recent age cohorts, and that it is 2X as high in women as in men. Dysthymic disorder consists of chronic depression that is insufficient in severity to justify diagnosis of major depression. Bipolar disorder (formerly known as manic-depressive disorder) is characterized by the experience of one or more manic episodes usually accompanied by periods of depression. In a manic episode, a person’s mood becomes elevated to the point of euphoria. Bipolar disorder affects a little over 1%-2% of the population and is equally as common in males and females. People are given the diagnosis of cyclothymic disorder when they exhibit chronic but relatively mild symptoms of bipolar disturbance. Evidence suggests genetic vulnerability to mood disorders. These disorders are accompanied by changes in neurochemical activity in the brain, particularly at norepinephrine and serotonin synapses. Cognitive models suggest that negative thinking contributes to depression. Learned helplessness and a pessimistic explanatory style have been proposed by Martin Seligman as predisposing individuals to depression. Hopelessness theory, the most recent descendant of the learned helplessness model of depression, proposes a sense of hopelessness as the “final pathway” leading to depression…not just explanatory style, but also high stress, low self-esteem, and other factors combine in the development of depression. Current research also implicates ruminating over one’s problems as important in the maintenance of depression, extending and amplifying individuals’ episodes of depression. Interpersonal inadequacies and poor social skills may lead to a paucity of life’s reinforcers and frequent rejection. Stress has also been implicated in the development of depressive disorders.
 Cyclothymic disorder. Etiology. Genetic vulnerability. Neurochemical factors - norepinephrine and serotonin synapses. Cognitive factors - pessimistic explanatory. Interpersonal roots - poor social skills. Precipitating stress. 2X as high in women. Mood disorders are a class of disorders marked by emotional disturbances of varied kinds that may spill over to physical, perceptual, social, and thought processes. Major depressive disorder is marked by profound sadness, slowed thought processes, low self-esteem, and loss of interest in previous sources of pleasure. Major depression is also called unipolar depression. Research suggests that the lifetime prevalence rate of unipolar depression is between 7 and 18%. Evidence suggests that the prevalence of depression is increasing, particularly in more recent age cohorts, and that it is 2X as high in women as in men. Dysthymic disorder consists of chronic depression that is insufficient in severity to justify diagnosis of major depression. Bipolar disorder (formerly known as manic-depressive disorder) is characterized by the experience of one or more manic episodes usually accompanied by periods of depression. In a manic episode, a person’s mood becomes elevated to the point of euphoria. Bipolar disorder affects a little over 1%-2% of the population and is equally as common in males and females. People are given the diagnosis of cyclothymic disorder when they exhibit chronic but relatively mild symptoms of bipolar disturbance. Evidence suggests genetic vulnerability to mood disorders. These disorders are accompanied by changes in neurochemical activity in the brain, particularly at norepinephrine and serotonin synapses. Cognitive models suggest that negative thinking contributes to depression. Learned helplessness and a pessimistic explanatory style have been proposed by Martin Seligman as predisposing individuals to depression. Hopelessness theory, the most recent descendant of the learned helplessness model of depression, proposes a sense of hopelessness as the final pathway leading to depression…not just explanatory style, but also high stress, low self-esteem, and other factors combine in the development of depression. Current research also implicates ruminating over one’s problems as important in the maintenance of depression, extending and amplifying individuals’ episodes of depression. Interpersonal inadequacies and poor social skills may lead to a paucity of life’s reinforcers and frequent rejection. Stress has also been implicated in the development of depressive disorders.")
42
Larry frequently hears his daughter's stuffed animals talking about him when
he is in the hallway outside his daughter's bedroom; Larry is experiencing a. delusions b. hallucinations c. disturbed emotions d. irrational thought

43
The presence of structural abnormalities in the brain that are assumed
to reflect deterioration of brain tissue has been associated with a. mood disorders b. schizophrenic disorders c. anxiety disorders d. somatoform disorders

44
Which of the following has not been proposed as a factor associated
with the development of schizophrenic disorders? a. neurological damage during prenatal development b. excessive levels of the neurotransmitter dopamine c. structural abnormalities in the brain d. inadequate social skills

45
ANSWERS: B D

46
Clinical Syndromes: Schizophrenia
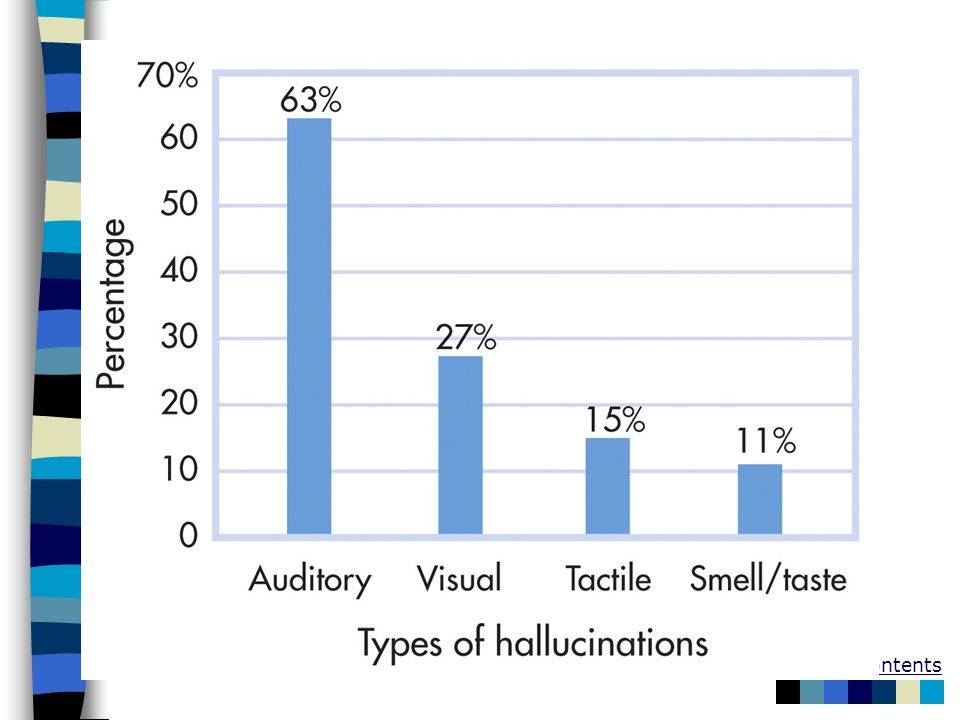
General symptoms Delusions and irrational thought Disorganized speech (word salad) and thinking Deterioration of adaptive behavior Hallucinations Disturbed emotions and reality Psychomotor disturbances (stupor, rigidity, waxy flexibility, posturing, ‘parroting’) Prognostic factors - A more favorable prognosis exists when the onset of the disorder is sudden and at a later age, the individual’s social and work adjustment was good prior to onset, the proportion of negative symptoms is low, and the patient has a good social support system Schizophrenic disorders are a class of disorders marked by delusions, hallucinations, disorganized speech, and disorganized behavior. Disturbed thought lies at the core of schizophrenia, whereas disturbed emotion lies at the core of mood disorders. Prevalence estimates suggest that schizophrenia occurs in about 1% of the population (several million people in the U.S.). General symptoms of schizophrenia include delusions, which are false beliefs that are maintained even though they clearly are out of touch with reality…belief that you a tiger, that private thoughts are being broadcasted to others, etc. Delusions of grandeur occur when people think they are famous or important. Chaotic thinking, or loose associations, is common in schizophrenia as well, where a person shifts topics in disjointed ways. Deterioration of adaptive behavior involves noticeable deficits in the quality of a person’s routine functioning in work, social relations, and personal care. Hallucinations are sensory perceptions that occur in the absence of a real, external stimulus or are gross distortions of perceptual input…hearing voices. Disturbed emotion may manifest as little emotional responsiveness (blunted or flat affect) or inappropriate emotional responses (laughing at a story of a child’s death). A more favorable prognosis exists when the onset of the disorder is sudden and at a later age, the individual’s social and work adjustment was good prior to onset, the proportion of negative symptoms is low, and the patient has a good social support system.
 and thinking. Deterioration of adaptive behavior. Hallucinations. Disturbed emotions and reality. Psychomotor disturbances (stupor, rigidity, waxy flexibility, posturing, ‘parroting’) Prognostic factors - A more favorable prognosis exists when the onset of the disorder is sudden and at a later age, the individual’s social and work adjustment was good prior to onset, the proportion of negative symptoms is low, and the patient has a good social support system. Schizophrenic disorders are a class of disorders marked by delusions, hallucinations, disorganized speech, and disorganized behavior. Disturbed thought lies at the core of schizophrenia, whereas disturbed emotion lies at the core of mood disorders. Prevalence estimates suggest that schizophrenia occurs in about 1% of the population (several million people in the U.S.). General symptoms of schizophrenia include delusions, which are false beliefs that are maintained even though they clearly are out of touch with reality…belief that you a tiger, that private thoughts are being broadcasted to others, etc. Delusions of grandeur occur when people think they are famous or important. Chaotic thinking, or loose associations, is common in schizophrenia as well, where a person shifts topics in disjointed ways. Deterioration of adaptive behavior involves noticeable deficits in the quality of a person’s routine functioning in work, social relations, and personal care. Hallucinations are sensory perceptions that occur in the absence of a real, external stimulus or are gross distortions of perceptual input…hearing voices. Disturbed emotion may manifest as little emotional responsiveness (blunted or flat affect) or inappropriate emotional responses (laughing at a story of a child’s death). A more favorable prognosis exists when the onset of the disorder is sudden and at a later age, the individual’s social and work adjustment was good prior to onset, the proportion of negative symptoms is low, and the patient has a good social support system.")
47
Subtyping of Schizophrenia
4 subtypes Paranoid type - delusions Catatonic type - muscular rigidity, random activity Disorganized type - incoherence, social withdrawal Undifferentiated type – doesn’t fit neatly in one of the above New model for classification Positive vs. negative symptoms Negative means taking away behaviors that were present ex. - no emotions (‘flat affect’), inappropriate emotions, ambivalence Positive means adding behaviors that were not already present ex..- hallucinations, delusions Currently, in the DSM-IV, there are 4 subtypes of schizophrenia. Paranoid schizophrenia is dominated by delusions of persecution, along with delusions of grandeur. Catatonic schizophrenia is marked by striking motor disturbances, ranging from muscular rigidity to random motor activity. In disorganized schizophrenia, a particularly severe deterioration of adaptive behavior is seen…incoherence, complete social withdrawal, delusions centering on bodily functions. People who clearly have schizophrenia, but cannot be placed in any of the above subtypes, are given the diagnosis of undifferentiated schizophrenia. There are many critics of the current subtyping system for schizophrenia. Some theorists argue that the disorder should be conceptualized along two categories, positive symptoms – behavioral excesses or peculiarities, such as hallucinations, delusions, bizarre behavior, and wild flights of ideas; and negative symptoms – behavioral deficits, such as flattened emotions, social withdrawal, apathy, impaired attention, and poverty of speech.
, inappropriate emotions, ambivalence. Positive means adding behaviors that were not already present. ex..- hallucinations, delusions. Currently, in the DSM-IV, there are 4 subtypes of schizophrenia. Paranoid schizophrenia is dominated by delusions of persecution, along with delusions of grandeur. Catatonic schizophrenia is marked by striking motor disturbances, ranging from muscular rigidity to random motor activity. In disorganized schizophrenia, a particularly severe deterioration of adaptive behavior is seen…incoherence, complete social withdrawal, delusions centering on bodily functions. People who clearly have schizophrenia, but cannot be placed in any of the above subtypes, are given the diagnosis of undifferentiated schizophrenia. There are many critics of the current subtyping system for schizophrenia. Some theorists argue that the disorder should be conceptualized along two categories, positive symptoms – behavioral excesses or peculiarities, such as hallucinations, delusions, bizarre behavior, and wild flights of ideas; and negative symptoms – behavioral deficits, such as flattened emotions, social withdrawal, apathy, impaired attention, and poverty of speech.")
48
Schizophrenia Delusions
false beliefs, often of persecution or grandeur, that may accompany psychotic disorders In a psychiatrist's waiting room two patients are having a conversation. One says to the other, "Why are you here?" The second answers, "I'm Napoleon, so the doctor told me to come here." The first is curious and asks, "How do you know that you're Napoleon?" The second responds, "God told me I was." At this point, a patient on the other side of the room shouts, "NO I DIDN'T!"

49
Symptoms of Schizophrenia
Delusions of persecution ‘they’re out to get me’ paranoia Delusions of grandeur “God” complex megalomania Delusions of being controlled the CIA is controlling my brain with a radio signal keywords: schizophrenia, symptoms, delusions

50
Etiology of Schizophrenia
Genetic vulnerability – high genetic predisposition - it runs in families - twin studies show high correlation for identical twins vs. fraternal Neurochemical factors – dopamine receptors are overactive which means an excess of dopamine Brain structure– enlarged ventricles The neurodevelopmental hypothesis - asserts that it is attributable to disruptions in maturational processes of the brain before or at the time of birth that are caused by prenatal viral infections or malnutrition, obstetrical complications, and other brain insults. Psychoactive medication – work by lowering levels of dopamine – prolonged use has side effects, ex. tremors, seizures, restlessness, weight gain, slow mental functioning, losing sense of self, blurred vision, or tardive dyskinesia - an incurable neurological disorder marked by involuntary writhing and ticklike movements of the mouth, tongue, face, hands, or feet. Research has linked schizophrenia to a genetic vulnerability and changes in neurotransmitter activity at dopamine, and perhaps serotonin, receptors. Structural abnormalities in the brain, such as enlarged ventricles, are associated with schizophrenia, as are metabolic abnormalities in the prefrontal and temporal lobes. Researchers theorize that positive symptoms are related to prefrontal abnormalities and negative symptoms to temporal abnormalities. The question remains to be answered re: whether these abnormalities are cause or consequence of schizophrenia. The neurodevelopmental hypothesis of schizophrenia asserts that it is attributable to disruptions in maturational processes of the brain before or at the time of birth that are caused by prenatal viral infections or malnutrition, obstetrical complications, and other brain insults. Studies of expressed emotion, or the degree to which a relative of a person with schizophrenia displays highly critical or emotionally overinvolved attitudes toward the patient, suggest that expressed emotion is a good predictor of the course of schizophrenic illness, negatively impacting prognosis. Precipitating stress and unhealthy family dynamics have also been shown to be related to schizophrenia.

51
Schizophrenia

52
Frequency of positive and negative symptoms in individuals at the time they were hospitalized for schizophrenia. Source: Based on data reported in Andreasen & Flaum, 1991.

54
Disorganized Thinking

56
Schizophrenia

59
Dissociative Identity Disorder
Originally known as “multiple personality disorder” 2 or more distinct personalities manifested by the same person at different times VERY rare and controversial disorder Examples include Sybil, Trudy Chase, Chris Sizemore (“Eve”) Has been tried as a criminal defense Nonpsychotic disorder, do not respond to meds memory loss keywords: dissociative identity disorder, symptoms
 Has been tried as a criminal defense. Nonpsychotic disorder, do not respond to meds. memory loss. keywords: dissociative identity disorder, symptoms.")
60
Dissociative Identity Disorder
Pattern typically starts prior to age 10 (childhood) Most people with disorder are women Most report recall of torture or sexual abuse as children and show symptoms of PTSD keywords: dissociative identity disorder, characteristics
 Most people with disorder are women. Most report recall of torture or sexual abuse as children and show symptoms of PTSD. keywords: dissociative identity disorder, characteristics.")
61
Causes of Dissociative Disorders?
Repeated, severe sexual or physical abuse. However, many abused people do not develop DID Combine abuse with biological predisposition toward dissociation? people with DID are easier to hypnotize than others may begin as series of hypnotic trances to cope with abusive situations keywords: causal theories of dissociative disorders

62
Some curious statistics
The DID Controversy Some curious statistics 1930–60: 2 cases per decade in USA 1980s: 20,000 cases reported many more cases in US than elsewhere varies by therapist—some see none, others see a lot Is DID the result of suggestion by therapist and acting by patient? keywords: dissociative identity disorder, controversy over Spanos asked college students to pretend they were accused murderers being examined by a psychiatrist. When given hypnotic therapy the students often expressed a second personality which claimed to be the murderer. This raises the question of whether DID might arise in some cases as a strategy or ploy by the patient, not just to avoid prosecution for crimes but perhaps to avoid other negative situations. It is not suggested that all DID cases arise in this way, but perhaps the large increase in diagnosis can be accounted for in this way. The increase in incidence in the 1980s was preceded by heightened awareness of the the stories of THE THREE FACES OF EVE and SYBIL which became known in the 1960’s

63
Personality Disorders
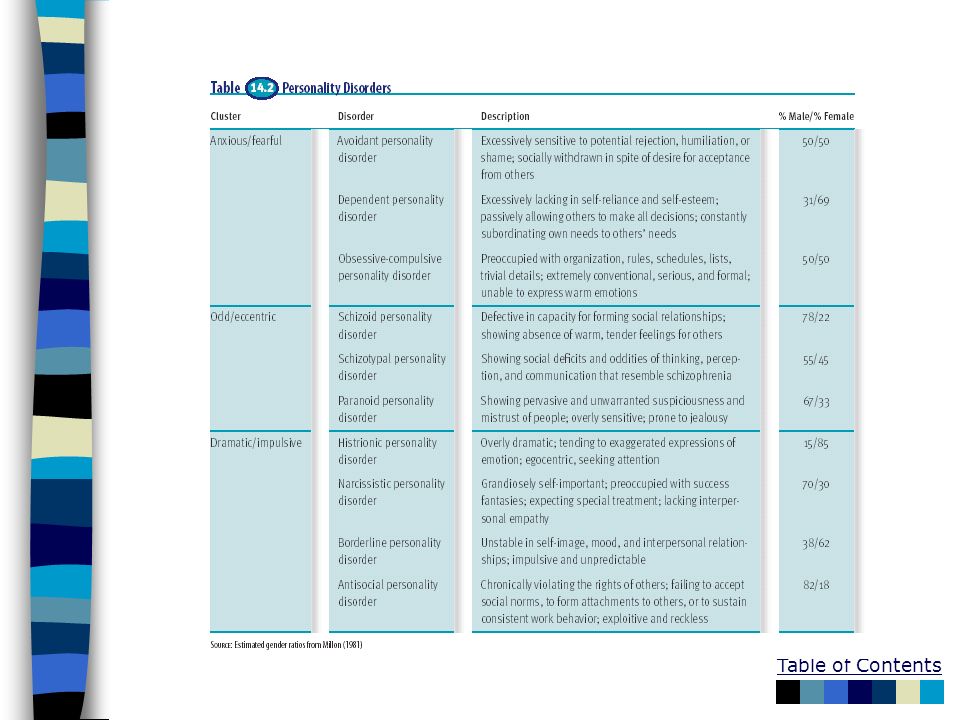
Anxious-fearful cluster Avoidant, dependent, obsessive-compulsive Dramatic-impulsive cluster Histrionic, narcissistic, borderline, antisocial Odd-eccentric cluster Schizoid, schizotypal, paranoid Etiology Genetic predispositions, inadequate socialization in dysfunctional families Personality disorders are a class of disorders marked by extreme, inflexible personality traits that cause subjective distress or impaired social and occupational functioning. Anxious-fearful cluster: Avoidant – excessively sensitive to potential rejection, humiliation or shame, Dependent – excessively lacking in self-reliance and self-esteem, Obsessive-compulsive – preoccupied with organization, rules, schedules, lists, and trivial details. Odd-eccentric cluster: Schizoid – defective in capacity for forming social relationships, Schizotypal – social deficits and oddities in thinking, perception, and communication, Paranoid – pervasive and unwarranted suspiciousness and mistrust. Dramatic-impulsive cluster: Histrionic – overly dramatic, tending to exaggerate expressions of emotion, Narcissistic – grandiosely self-important, lacking interpersonal empathy, Borderline – unstable in self-image, mood, and interpersonal relationships, Antisocial – chronically violating the rights of others, non-accepting of social norms, inability to form attachments. Specific personality disorders are poorly defined, and there is much overlap among them…some theorists propose replacing the current categorical approach with a dimensional one. Research on the etiology of personality disorders has been conducted primarily on antisocial personality disorder. Genetic vulnerability has been suggested, along with autonomic reactivity, inadequate socialization, and observational learning.

65
Psychological Disorders and the Law
Insanity M’naghten rule - mental disorder makes a person unable to distinguish right from wrong Involuntary commitment danger to self danger to others in need of treatment Insanity is not a diagnosis, it is a legal concept. Insanity is a legal status indicating that a person cannot be held responsible for his or her actions because of mental illness. The M’naghten rule holds that insanity exists when a mental disorder makes a person unable to distinguish right from wrong. Involuntary commitment occurs when people are hospitalized in psychiatric facilities against their will. Rules vary from state to state, but generally, people are subject to involuntary commitment when they are a danger to themselves or others or when they are in need of treatment (as in cases of severe disorientation). In emergency situations, psychiatrists and psychologists can authorize temporary commitment only for a period of hours. Long-term commitments must go through the courts and are usually set up for renewable six-month periods.
. In emergency situations, psychiatrists and psychologists can authorize temporary commitment only for a period of hours. Long-term commitments must go through the courts and are usually set up for renewable six-month periods.")
67
Culture and Pathology Cultural variations Culture bound disorders Koro
Windigo Anorexia nervosa The principal categories of psychological disturbance are identifiable in all cultures, but milder disorders may go unrecognized in some societies. Culture-bound disorders illustrate the diversity of abnormal behavior around the world, as well as cultural influence. Koro is an obsessive fear that one’s penis will withdraw into one’s abdomen, seen only in Malaya and other regions of southern Asia. Windigo involves intense craving for human flesh and fear that one will turn into a cannibal, seen only among Algonquin Indian cultures. Anorexia nervosa is an eating disorder characterized by intentional self-starvation, until recently seen only in affluent Western cultures.

Similar presentations
















>")


















