Download presentation
Presentation is loading. Please wait.

1
Child and Adolescent Health
The Promise of Preconception Care in Prevention of Birth Defects and Preterm Births Footer to be added with mtg name date and WHO logo Dr Neena Raina Regional Advisor Child and Adolescent Health WHO - SEARO WHO-SEARO

2
Structure of presentation
What is Pre-conception Care Do we have evidence based interventions Why is it important in SEAR Opportunities for introducing it in SEAR “Healthy Transitions” for Adolescents Way forward WHO-SEARO

3
1.What is Pre-conception Care
WHO-SEARO

4
Pre-pregnancy health status and health behaviors have direct or indirect implications for maternal and neonatal outcomes Intervening after a woman is pregnant has limited impact: First few weeks after conception are critical for fetal development Week 5: brain, spinal cord, heart begin to form Week 6: Neural tube closes; the heart is pumping Week 7: Brain and face are rapidly developing Most women do not seek prenatal advice/care before 12 weeks when it is too late to modify many risks Intervening during pregnancy is too late for many interventions Many health risk behaviours are initiated during adolescence WHO-SEARO

5
Modifiable risk factors are common to several “congenital conditions”
Malformations Preterm Birth IUGR Developm. disability Nutrition status X Insufficient folic acid/vitamin Smoking Alcohol use / abuse Illicit drugs Obesity Diabetes - getsational Infectious diseases Selected medications Psycho-social stressors Environment and working activity ICBDSR presentation in Regional Meeting 2012 WHO-SEARO

6
Many risk factors are initiated during adolescence
Modifiable risks for birth defects and prematurity that need to be addressed before conception Undernutrition and anaemia Folic Acid insufficiency Obesity Diabetes Hypertension Epilepsy Alcohol use Age at pregnancy Too close and too many pregnancies Infections: TORCH Use of medications during early pregnancy Exposure to toxins Exposure to tobacco WHO-SEARO Many risk factors are initiated during adolescence

7
Pre-Conception Care Preconception care is the provision of biomedical, behavioral and social health interventions to women and couples before conception occurs. Aims: Improving health status and reducing behaviors and individual and environmental factors to improve maternal and child health outcomes. Boundary: the period before pregnancy may be divided into a proximal and a distal period: Proximal period immediately preceding pregnancy Distal adolescence (10-19 years) WHO-SEARO
 WHO-SEARO.")
8
Life course – when to intervene?

9
2.Do we have evidence based interventions
WHO-SEARO

10
Gathering evidence: Global consultation
Global consultation in WHO Headquarters, Geneva - February 2012 Meeting to develop a global consensus on preconception care to reduce maternal and childhood mortality and morbidity In 2012, WHO organized a meeting to develop global consensus on preconception care to reduce maternal and childhood mortality and morbidity The meeting gathered three groups: Representatives from groups who have led reviews and research within preconception care Individuals with experience in carrying out preconception care Organizations looking to move forward the preconception area, including WHO and other UN organizations, Bill and Melinda Gates Foundation, March of Dimes and Preparing for Life Initiative

11
Three questions were answered:
What are the health problems, risk behaviours and risk factors contributing to maternal and childhood mortality and morbidity? What are the effective interventions to address them? What are the effective means of delivering these interventions? Why the health problems/risk behaviours/risk factors were chosen – how they contribute to maternal and childhood mortality and morbidity Effective interventions to address them Effective and existing delivery mechanisms to deliver them in middle and low income countries

12
Gathering evidence: Existing reviews
Using existing evidence and reviews from: The Centers for Disease Control and Prevention Erasmus University Aga Khan University Health Council of the Netherlands

13
Evidence for Pre-Conception Care
Recommendations to Improve Preconception Health – United States by the Centers for Disease Control and Prevention (2006) Systematic Review of Preconception Evidence by the Aga Khan University in Karachi, Pakistan (2011) WHO-SEARO
 Systematic Review of Preconception Evidence by the Aga Khan University in Karachi, Pakistan. (2011) WHO-SEARO.")
14
Gathering evidence: WHO departments
Consultation with various relevant WHO departments: Maternal, Newborn, Child and Adolescent Health Reproductive Health and Research Nutrition for Health and Development HIV Mental Health and Substance Abuse Immunization, Vaccine and Biologicals Public Health and Environment Tobacco-Free Initiative Violence and Injury Prevention Partnership for Maternal, Newborn and Child Health

15
Strength of evidence There is growing experience in implementing preconception care initiatives: In high-income countries, such as Italy, the Netherlands and the United States In low- and middle-income countries, such as Bangladesh, the Philippines and Sri Lanka There is growing experience in implementing preconception care initiatives both in high, middle and low income countries. Countries with particular experience are Italy, the Netherlands, United States, Bangladesh, the Philippines and Sri Lanka In the next two presentations… Weak evidence of how to deliver preconconception care: this is where the focus need to be

16
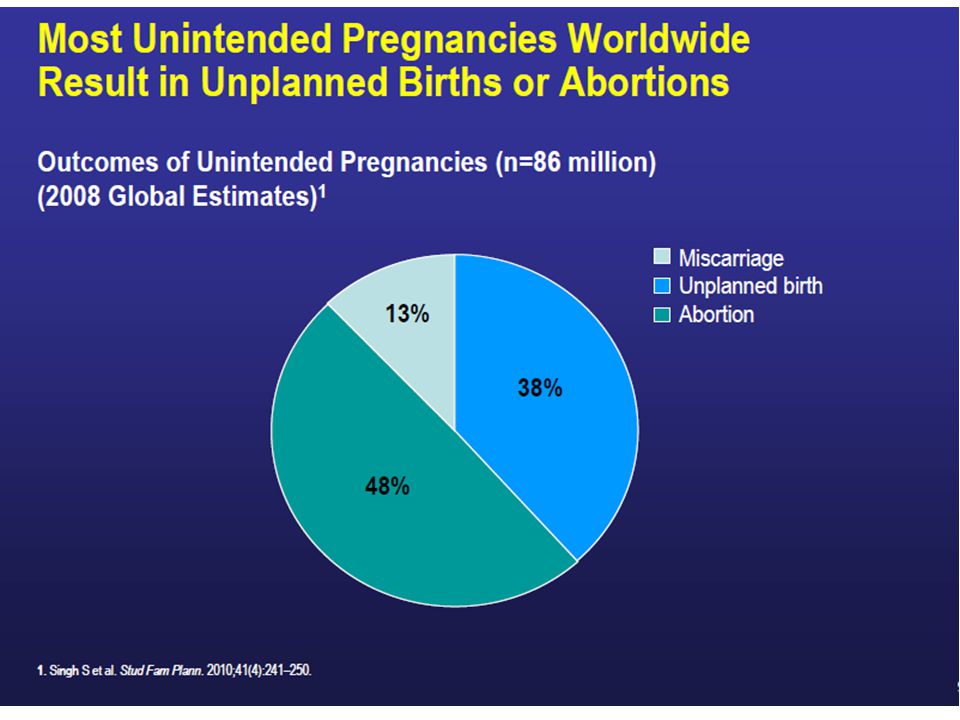
Preconception care has a positive effect on a range of health outcomes
child mortality maternal mortality birth defects Reduced too early pregnancy preterm birth Reduced abortion congenital and neonatal infections Improved mental health cretinism Improved mother nutritional status macrosomia Preconception care has a positive effect on a range of health outcomes. Among others, preconception care can: Reduce maternal and child mortality Prevent unintended pregnancies Prevent complications during pregnancy and delivery Prevent stillbirths, preterm birth and low birth weight Prevent birth defects Prevent neonatal infections Prevent underweight and stunting Prevent vertical transmission of HIV/STIs Lower the risk of some forms of childhood cancers Lower the risk of type 2 diabetes and cardiovascular disease later in life childhood cancers Low birth weight vertical transmission of HIV/STIs Underweight and stunting hypothyroidism diarrhoea

17
Tobacco use and youth health: a potential for Healthy Transitions
5 million deaths in 2005 10 million deaths in 2020 20 y.o. 90% of adult smokers are estimated to have started smoking before age 20 years

18
Exposure to environmental toxins in early life and its long term effect
cigarette smoking during pregnancy reduced birth weight or increased risk of lower birth weight offspring obesity eliminating smoking before or during pregnancy could avoid 5–7% of preterm related deaths and 23–24% of cases of sudden infant death syndrome eliminating smoking before or during pregnancy could avoid 5–7% of preterm related deaths and 23–24% of cases of sudden infant death syndrome

19
Areas addressed by preconception care package
However, the report most importantly provides the evidence based 'package of interventions' addressing 13 various areas: Nutritional conditions; vaccine preventable diseases; genetic conditions; environmental health; infertility/subfertility; female genital mutilation; too early, unwanted and rapid successive pregnancies; sexually transmitted infections; HIV; interpersonal violence; mental health; psychoactive substance abuse; and tobacco use WHO-SEARO

20
Evidence-based interventions: Selected examples
Area addressed by the preconception care package Evidence-based interventions Nutritional conditions Screening for anemia Supplementing iron and folic acid Information, education and counselling Monitoring nutritional status Supplementing energy- and nutrient-dense food Screening for diabetes mellitus Management of diabetes mellitus Counselling people with diabetes mellitus Monitoring blood glucose (also in pregnancy) Promoting exercise Salt iodization I will go through three examples of areas; that is nutritional conditions; genetic conditions; and too early, unwanted and rapid successive pregnancies "Read the evidence-based interventions" WHO-SEARO
 Promoting exercise. Salt iodization. I will go through three examples of areas; that is nutritional conditions; genetic conditions; and too early, unwanted and rapid successive pregnancies. Read the evidence-based interventions WHO-SEARO.")
21
Evidence-based interventions: Selected examples
Areas addressed by the preconception care package Evidence-based interventions Genetic conditions Screening for anemia Taking a thorough family history Family planning Genetic counselling Carrier screening and testing Appropriate treatment Providing community-based education Community-wide or national screening among populations at high risk Population-wide screening "Read the evidence-based interventions" WHO-SEARO

22
Evidence-based interventions: Selected examples
Areas addressed by the preconception care package Evidence-based interventions Keeping girls in school Influencing cultural norms that support early marriage and coerced sex Creating visible, high-level support for pregnancy prevention programmes Educating girls and boys about sexuality, reproductive health and contraceptive use Building community support for preventing early pregnancy and for contraceptive provision to adolescents Enabling adolescents to obtain contraceptive services Empowering girls to resist coerced sex Engaging men and boys to critically assess norms and practices regarding gender-based violence and coerced sex Educating women and couples about the dangers to the baby and mother of short birth intervals Providing contraceptives Too-early, unwanted and rapid successive pregnancy "Read the evidence-based interventions" WHO-SEARO

23
3.Why Preconception care is important in SEAR
WHO-SEARO

24
MDG 5 Indicators-SEAR Countries
MMR (per live births) SBA (%) CPR (%) Unmet Need for family planning (%) ANC (%) Births by caesarean section (%) Post natal within 2 days of child birth (%) 1990 2000 2010 At least 1 visit Atleast 4 visits BAN 800 400 240 31 61 12 50 26 17 27 BHU 1000 430 180 58 66 74 77 KRD 97 120 81 100 94 13 IND 600 390 200 55 21 75 8 48 INO 340 220 80 93 82 7 70 MAV 830 190 60 95 35 29 99 85 32 67 MMR 520 300 71 46 83 43 NEP 770 360 170 36 5 45 SRL 68 24 THA 54 3 TLS 610 30 22 84 2 25 Source: World Health Statistics 2013
 SBA (%) CPR (%) Unmet Need for family planning (%) ANC (%) Births by caesarean section (%) Post natal within 2 days of child birth (%) At least 1 visit. Atleast 4 visits. BAN BHU KRD IND INO MAV MMR NEP SRL THA TLS Source: World Health Statistics")
25
The Region is not likely to reach MDG4
Decline in NMR has been slower WHO-SEARO

26
Newborn mortality remains high in SEAR
Responsible for 54% of under-five deaths Three congenital conditions: Prematurity, Birth Asphyxia and Birth Defects account for 35-55% of under-5 mortality These causes of mortality share many risk factors WHO-SEARO

27
Prematurity, Birth Asphyxia and Birth Defects account for 35% (Myanmar) to 55% (Thailand) of under-5 mortality Source: World Health Statistics WHO-SEARO

28
Estimates of Birth Defects in SEAR
March of Dimes Global Report on Birth Defects (2006) 28 WHO-SEARO
 28. WHO-SEARO.")
29
Birth Defects Situation Analysis: WHO-SEARO and US-CDC

30
Estimates of Pre Term Births Born Too Soon Report: 2012
Very hazy slide. Need to improve or re do it WHO-SEARO

31
Eleven countries with PT birth >15% by Rank Born Too Soon Report: 2012
Again written material not very clear. Re do it WHO-SEARO

32
4.Preconception Care in SEAR
Twin track: Pre- and Inter-pregnancy care: Maternal Health Healthy Transitions for adolescents: Adolescent Health WHO-SEARO

33
Is there a gap in Continuum of Care?
Healthcare provided across the lifecycle through strong public health programs can ensure that all women and babies are healthy There is a gap in the continuum of care for adolescent girls (and boys) and women before pregnancy. All babies and children – female and male – have the right to survive and to grow and develop in good health. Similarly, all women and men have the right to be healthy physically, psychologically and socially. For this to happen, strong public health programmes that use a life-course perspective from infancy through childhood and adolescence to adulthood are needed. The reality is that such programmes do not exist or are very weak in most low- and middle-income countries. Even where strong public health programmes across the life-course are in place, they do not guarantee that women enter pregnancy in good health. For this reason, prenatal programmes are needed to promote good health during pregnancy, to prevent health problems and to respond to those problems that occur. The reality is that many women in low- and middle-income countries do not have adequate access to the prenatal care they need. We need to strengthen public health programmes across the life-course. We also need to improve access to good-quality prenatal care services. In addition, there is growing evidence that extending the maternal, newborn and child health continuum with one step before prenatal care – i.e. before pregnancy occurs – can increase the well-being of women and couples and improve subsequent pregnancy and child health outcomes.
 and women before pregnancy. All babies and children – female and male – have the right to survive and. to grow and develop in good health. Similarly, all women and men have the. right to be healthy physically, psychologically and socially. For this to happen, strong public health programmes that use a life-course perspective from. infancy through childhood and adolescence to adulthood are needed. The. reality is that such programmes do not exist or are very weak in most low- and. middle-income countries. Even where strong public health programmes across the life-course are in. place, they do not guarantee that women enter pregnancy in good health. For. this reason, prenatal programmes are needed to promote good health during. pregnancy, to prevent health problems and to respond to those problems that. occur. The reality is that many women in low- and middle-income countries. do not have adequate access to the prenatal care they need. We need to strengthen public health programmes across the life-course. We. also need to improve access to good-quality prenatal care services. In addition, there is growing evidence that extending the maternal, newborn and child. health continuum with one step before prenatal care – i.e. before pregnancy. occurs – can increase the well-being of women and couples and improve. subsequent pregnancy and child health outcomes.")
34
Strengthening pre-conception care in the RMNCAH Continuum
Clinical Screening and management of chronic diseases especially diabetes Genetic counselling CHILDBIRTH CARE Emergency obstetric care Skilled obstetric care and immediate newborn care (hygiene, warmth, breastfeeding) and resuscitation PMTCT EMERGENCY NEWBORN AND CHILD CARE - Hospital care of newborn and childhood illness including HIV care - Extra care of preterm babies including kangaroo mother care - Emergency care of sick newborns Post-abortion care - STI case management Outreach/outpatient Multivitamin and folic acid supplementation Family planning Youth development programs Prevention of obesity ANTENATAL CARE - 4-visit focused ANC package - IPTp and bednets for malaria - PMTCT POSTNATAL CARE - Promotion of healthy behaviors - Early detection of and referral for illness - Extra care of LBW babies - PMTCT Family/community - Counselling and preparation for newborn care, breastfeeding, birth and emergency preparedness Healthy home care including: Newborn care (hygiene, warmth) Nutrition including exclusive breastfeeding and appropriate complementary feeding Seeking appropriate preventive care - Danger sign recognition and careseeking for illness - Oral rehydration salts for prevention of diarrhoea - Where referral is not available, consider case management for pneumonia, malaria, neonatal sepsis - Where skilled care is not available, consider clean delivery and immediate newborn care including hygiene, warmth and early initiation of breastfeeding Optimising Adolescent and pre-pregnancy nutrition Health education and counseling on risk factors prevention INTERSECTORAL Improved living and working conditions – Housing, water and sanitation, and nutrition education and female empowerment Pre-pregnancy Pregnancy WHO-SEARO Birth 34
 and resuscitation. PMTCT. EMERGENCY NEWBORN AND CHILD CARE. - Hospital care of newborn and childhood illness including HIV care. - Extra care of preterm babies including kangaroo mother care. - Emergency care of sick newborns. Post-abortion care. - STI case management. Outreach/outpatient. Multivitamin and folic acid supplementation. Family planning. Youth development programs. Prevention of obesity. ANTENATAL CARE. - 4-visit focused ANC package. - IPTp and bednets for malaria. - PMTCT. POSTNATAL CARE. - Promotion of healthy behaviors. - Early detection of and referral for illness. - Extra care of LBW babies. - PMTCT. Family/community. - Counselling and preparation for newborn care, breastfeeding, birth and emergency preparedness. Healthy home care including: Newborn care (hygiene, warmth) Nutrition including exclusive breastfeeding and appropriate complementary feeding. Seeking appropriate preventive care. - Danger sign recognition and careseeking for illness. - Oral rehydration salts for prevention of diarrhoea. - Where referral is not available, consider case management for pneumonia, malaria, neonatal sepsis. - Where skilled care is not available, consider clean delivery and immediate newborn care including hygiene, warmth and early initiation of breastfeeding. Optimising Adolescent and pre-pregnancy nutrition. Health education and counseling on risk factors prevention. INTERSECTORAL Improved living and working conditions – Housing, water and sanitation, and nutrition. education and female empowerment. Pre-pregnancy. Pregnancy. WHO-SEARO. Birth. 34.")
35
Pre-pregnancy care for prevention birth defects Life course Continuum
Infancy U5 Neonatal period Pregnancy Birth 10-19 Pre-Pregnancy CH Immunization Newborn Care Ado Health SBA PCC ANC Interventions to address MH risk factors for BD and PT births WHO-SEARO

36
Sri Lanka Package for newly married couples Goal: To have improved reproductive health outcomes by improving the health of the newly married couples. WHO-SEARO

37
Package for newly married couples
RISK SCREENING CLINICAL ASSESSMENT IMMUNIZATION AWARENESS AND COUNSELLING PROVISION OF OTHER SERVICES WHO-SEARO

38
TOOLS IN THE PACKAGE INVITATION CARD SCREENING TOOL
GUIDE FOR HEALTH WORKERS BOOK FOR THE NEW COUPLE BMI CALCULATOR WHO-SEARO

39
SCREENING TOOL Screen for risk factors by using the screening tool by PHM/MOH Basic investigations Physical assessment by PHM Height, weight and BMI Clinical examination by MOH Refer for further diagnosis /treatment/ for specialized care Follow up WHO-SEARO

40
Book for the New Couple ♣ SEXUALITY AND SEXUAL RELATIONSHIP
♣ SEXUALLY TRANSMITTED DISEASES AND RESPONSIBLE SEXUAL BEHAVIOUR ♣ A PLANNED FAMILY ♣ GOOD NUTRITION ♣ GOOD HEALTH HABITS/ HEALTHY BEHAVIOUR/ HEALTHY LIFE STYLE ♣ GOOD MARITAL RELATIONSHIP AND WELL BEING OF THE FAMILY ♣ BENEFITS OF NON VIOLENCE ♣ BEFORE CONCEPTION ♣ MALE PARTICIPATION AND PARENTHOOD ♣ TOBACCO AND ALCOHOL WHO-SEARO

41
5.Many health risk behaviours are initiated during adolescence: Need to catch them young “Healthy Transitions” WHO-SEARO

42
Large number of adolescents in SEAR with many health problems
Proportion of adolescents (10-19) Sexual and reproductive health problems Nutritional problems Substance use: Tobacco, alcohol Injuries, accidents and violence Mental health problems 1.2 billion adolescents (10-19) globally About 350 Millions in SEAR of which 230 million in India WHO-SEARO Source: World population prospects: The 2006 Revision Population Database.
 Sexual and reproductive health problems. Nutritional problems. Substance use: Tobacco, alcohol. Injuries, accidents and violence. Mental health problems. 1.2 billion adolescents (10-19) globally About 350 Millions in SEAR of which 230 million in India. WHO-SEARO. Source: World population prospects: The 2006 Revision Population Database.")
43
Health problems start during Adolescent period
Age parameter: years Confounding factors: Biological: Early or late onset of puberty Social-cultural factors Experiencing rapid growth and development: Physical: Body image and form Sexual: Reproductive capacity Mental: Mind Emotional-psychological Social Formative Phase: Attitudes Behaviours Heterogeneous groups and circumstances with variable needs: Boys and girls Urban and rural In school and out of school Unmarried and married: Pregnant and mothers At home and homeless (on streets) In employment (formal and informal Age is only one of the parameters to define VYA. There are biological and socio-cultural factors that contribute to the definition Early adolescence is a very special time between older childhood and full blown adolescence. Physically, it is the time when puberty occurs and the growth spurt takes off. Brain continues to develop and evolve until 25 years of age Psychologically, it is the time when the cognitive changes of adolescence are beginning and when emotional and social competencies are starting to be built. It is a time when the first steps in the development of sense of personal identity and autonomy are being taken. Socially, it is the time of change – a time when parental influence begins to decline and when the influence of others – including peers and other adults – begins to increase. Attitudes and beliefs start taking roots and behaviours start getting formed. Gender roles and socialization set in.
 In employment (formal and informal. Age is only one of the parameters to define VYA. There are biological and socio-cultural factors that contribute to the definition. Early adolescence is a very special time between older childhood and full blown adolescence. Physically, it is the time when puberty occurs and the growth spurt takes off. Brain continues to develop and evolve until 25 years of age. Psychologically, it is the time when the cognitive changes of adolescence are beginning and when emotional and social competencies are starting to be built. It is a time when the first steps in the development of sense of personal identity and autonomy are being taken. Socially, it is the time of change – a time when parental influence begins to decline and when the influence of others – including peers and other adults – begins to increase. Attitudes and beliefs start taking roots and behaviours start getting formed. Gender roles and socialization set in.")
44
Proportion of adolescents who have begun childbearing
Early Marriage and child- bearing Per cent married by Age 18 among adolescents (15-19 yrs) Proportion of adolescents who have begun childbearing Poor women aged are more likely to begin child bearing early Source: Bangladesh DHS 2007; India NFHS ; Indonesia DHS 2007; Nepal DHS 2006; Sri Lanka DHS ; Timor-Leste DHS 2003 WHO-SEARO
 Proportion of adolescents who have begun childbearing. Poor women aged are more likely to begin child bearing early. Source: Bangladesh DHS 2007; India NFHS ; Indonesia DHS 2007; Nepal DHS 2006; Sri Lanka DHS ; Timor-Leste DHS WHO-SEARO.")
47
Adolescent Pregnancy: Higher Child Mortality
Source: Bangladesh DHS 2011; India NFHS ; Indonesia DHS 2007; Maldives DHS 2009; Myanmar FRHS 2007; Nepal DHS 2011; Sri Lanka DHS ; Timor-Leste DHS WHO-SEARO

48
Large number are under-nourished and anaemic
WHO-SEARO Source: Bangladesh DHS 2011; India NFHS ; Nepal DHS 2011; Sri Lanka DHS 2006; Maldives DHS 2009; Timor-Leste DHS

49
Dietary behaviors, Overweight & Obesity (13-15 years)
Source: Latest Global school-based student health survey (GSHS) WHO-SEARO
 WHO-SEARO.")
50
Early Tobacco use among adolescents (13-15 years)
Source: Latest Global Youth Tobacco Survey (GYTS) WHO-SEARO
 WHO-SEARO.")
51
Early Alcohol Consumption(13-15 years)
Source: Latest Global school-based student health survey (GSHS) WHO-SEARO
 WHO-SEARO.")
52
High Unintentional Injuries and Violence(13-15 Years)
Source: Latest Global school-based student health survey (GSHS) WHO-SEARO
 WHO-SEARO.")
53
Mental Health Problems ( 13-15 Years)
WHO-SEARO Source: Latest Global school-based student health survey (GSHS)
")
54
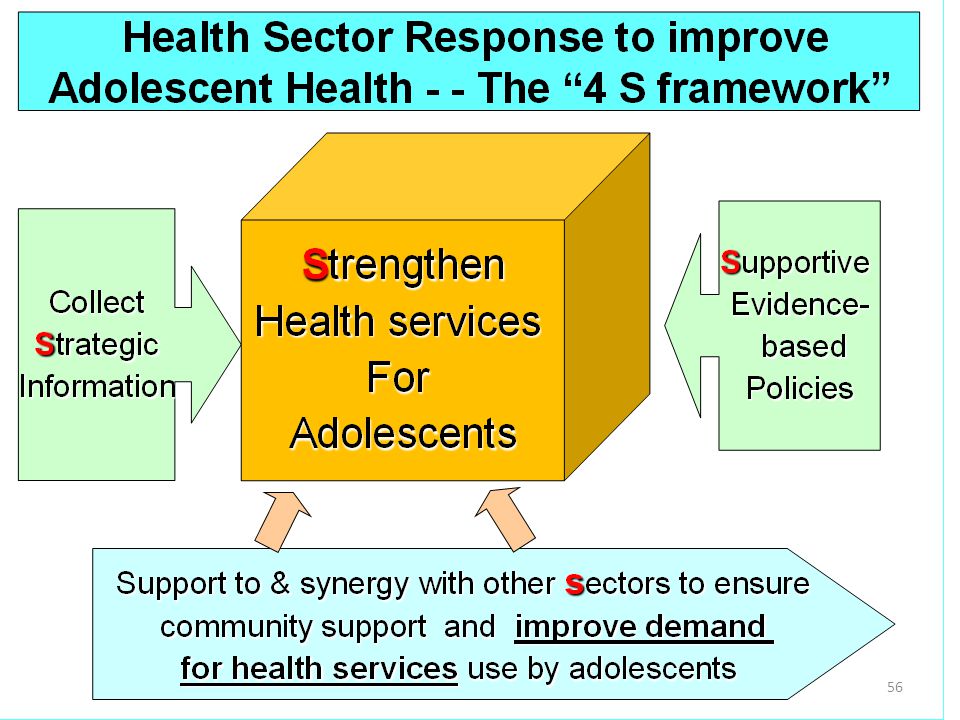
Public Health Issues with Adolescents
Nutrition Issues: Undernutrition, Anemia, Overnutrition Sexual And reproductive health: Early sex: unsafe Coerced sex Early marriage and child bearing STI, HIV Mental Health: Anxiety, stress, depression, suicide Tobacco and alcohol use Injury and accidents Violence: Victims and perpetrators Young adolescents experience important public health problems Health Sector needs to collaborate with other sectors WHO-SEARO

55
“Home” for adolescents in health services ?
Maternal and reproductive health services Newborn and child health services Disease Treatment for all

57
Progress so far Regional Strategy and National strategies (9 countries) Country Fact sheets on AHD and Adolescent pregnancy National Standards and implementation guidelines on AFHS (9 countries) Training packages adapted, HWs trained (8 countries) Quality and coverage assessments (6 countries) Regional Program management capacity building course Collaboration with other sectors - education
 Training packages adapted, HWs trained (8 countries) Quality and coverage assessments (6 countries) Regional Program management capacity building course. Collaboration with other sectors - education.")
58
Package of AH services: Range in SEAR Countries
Physical & mental health promotion Nutrition and micronutrients STI/RTI: Screen and manage HIV/AIDS prevention, testing Contraception, condom promotion Pregnancy and childbirth care Substance use prevention Healthy Lifestyles promotion Immunization SEARO is working towards developing “Healthy Transitions” package for comprehensive care of adolescent boys and girls covering all these areas. An age-appropriate package would be offered to age group

59
Coverage assessment: Utilization Received IFA Tabs in Last Six Month
Haryana, India August 2013 WHO-SEARO

60
Adolescent Health Programme in SEAR
Adolescent Health Programme being scaled up in SEAR Countries Focus has been on Sexual and Reproductive Health Opportunity to add elements of Pre-Conception Care Package – Healthy Transitions Package SEARO is working towards developing “Healthy Transitions” package for comprehensive care of adolescent boys and girls covering all these areas August 2013 WHO-SEARO

61
“Healthy Transitions for Adolescents” package
We know that specific interventions are effective and can be delivered to Adolescents Evidence-based preventive and curative health interventions for adolescents Existing delivery mechanisms that could be used to deliver interventions at scale Provide age-appropriate sexual health education Delay pregnancy Provide contraceptive services including condoms Prevent, screen and manage STIs, HIV Provide Iron folic acid Immunization Prevention of Substance use Prevent NCD risk behaviours School health program Nutrition program Youth programs AFHS HIV testing and counselling clinics NCD programmes Mental Health programmes “Healthy Transitions for Adolescents” package WHO-SEARO

62
‘Healthy Transitions for adolescents’ Ensuring health across life-course
Healthy adolescence Healthy reproductive health outcomes Reduction in prevalence of prematurity, LBW, Birth Defects Reduction in maternal, foetal, neonatal and child mortality Healthy adulthood (long term) NCD prevention Reduction in Tobacco and harmful use of alcohol related problems and cost STIs and HIV prevention WHO-SEARO
 NCD prevention. Reduction in Tobacco and harmful use of alcohol related problems and cost. STIs and HIV prevention. WHO-SEARO.")
63
Existing Opportunities in Public Health Programmes
Where Service type Intervention / package Health Facilities RH Services AFHS Immunization programmes Add preconception-related interventions Integrate essential components of Pre-marital counseling and genetic screening Expanded post-natal care (facility visits) Healthy Lifestyles: NCD prevention Schools School Health Programme Health Promoting Schools Integrate essential components of Pre-marital counseling Nutrition and micronutrient supplementation Out Reach Community support groups & delivery platforms Mass media campaigns/ Social marketing Information technology, (mHealth) Expanded post-natal care (home visits) Pre-marital counseling Optimizing Adolescent and pre-pregnancy nutrition WHO-SEARO
 Healthy Lifestyles: NCD prevention. Schools. School Health Programme. Health Promoting Schools. Integrate essential components of Pre-marital counseling. Nutrition and micronutrient supplementation. Out Reach. Community support groups & delivery platforms. Mass media campaigns/ Social marketing. Information technology, (mHealth) Expanded post-natal care (home visits) Pre-marital counseling. Optimizing Adolescent and pre-pregnancy nutrition. WHO-SEARO.")
64
Existing Opportunities in Public Health Programmes
Where Service type Intervention / package Health Facilities RH Services AFHS Immunization programmes Add preconception-related interventions Integrate essential components of Pre-marital counseling and genetic screening Expanded post-natal care (facility visits) Healthy Lifestyles: NCD prevention Schools School Health Programme Health Promoting Schools Integrate essential components of Pre-marital counseling Nutrition and micronutrient supplementation Out Reach Community support groups & delivery platforms Mass media campaigns/ Social marketing Information technology, (mHealth) Expanded post-natal care (home visits) Pre-marital counseling Optimizing Adolescent and pre-pregnancy nutrition Use of modern communication technology for health assessment and prevention/promotion WHO-SEARO
 Healthy Lifestyles: NCD prevention. Schools. School Health Programme. Health Promoting Schools. Integrate essential components of Pre-marital counseling. Nutrition and micronutrient supplementation. Out Reach. Community support groups & delivery platforms. Mass media campaigns/ Social marketing. Information technology, (mHealth) Expanded post-natal care (home visits) Pre-marital counseling. Optimizing Adolescent and pre-pregnancy nutrition. Use of modern communication technology for health assessment and prevention/promotion. WHO-SEARO.")
65
Preconception care in SEAR: 2 Tracks
Infancy U5 Neonatal period Pregnancy Birth 10-19 Pre-Pregnancy CH Immunization Newborn Care AFHS SBA PCC ANC Healthy Transitions for adolescents Maternal Health WHO-SEARO

66
6. Way forward and challenges
WHO-SEARO

67
Regional expert Group Consultation on Pre-Conception Care: Aug 2013 WHO-SEARO and CDC-US
PCC package would address maternal mortality, neonatal morality, pregnancy wastage, birth defects, pre term births and intrauterine growth retardation. The selected interventions would need to be implemented through integration and convergence within the health system as well as in other sectors. Optimize on established programmes such as Maternal, Reproductive ,Newborn and Child Health and adolescent health programmes as well as the programmes like Birth Defects prevention and Non Communicable Diseases. Expanding interventions to adolescent boys and girls would ensure better RH outcomes as well as healthy adulthood in the long term. WHO-SEARO

68
Opportunities Need for demonstration projects
Global commitments and partnerships for MDG 4 and 5 – Health agenda beyond 2015 Enhanced commitment of national governments for AH programme and earmarking of domestic resources Better understanding of adolescent brain Newborn and child health plans, RH plans at Global, regional and national level. New technology: Information and communication technology (internet,Mobile phones,Social media) to connect with young people and gatekeepers New initiatives: Newborn health, Preterm births, RH ,Birth defects prevention, Pre-conception, HPV, NCD prevention Need for demonstration projects August 2013 WHO-SEARO
 to connect with young people and gatekeepers. New initiatives: Newborn health, Preterm births, RH ,Birth defects prevention, Pre-conception, HPV, NCD prevention. Need for demonstration projects. August WHO-SEARO.")
69
Every Journey begins with a single step, But you will never finish if you don’t start!

70
miles to go…

71
Regional Meeting on Birth Defects, New Delhi
Thank You 13 Dec 2011 Regional Meeting on Birth Defects, New Delhi

Similar presentations














 Office of Overseas Programming & Training Support (OPATS) HIV Prevention Training Package Session 1: Introduction.>")





