Download presentation
Presentation is loading. Please wait.

1
Introduction to Infant Nutrition

2
Framework – Growth and Assessment – Nutrient needs – Formula and Breast milk – Feeding development and relationship – Non milk feedings

3
Population v.s. individual

4
Goals and Objectives Optimal growth and development Individual health Population Health Prevention and Chronic Illness

5
Population vs individual AAP Guidelines DRI’s Bright Futures Start Healthy Feeding Guidelines

6
Needs Guidelines Recommendations education

7
Recommendations/guidelines DRI: Dietary Reference Intakes – AI – UL – EER AAP Bright Futures Start Healthy feeding guidelines

8
DRI: Dietary Reference Intakes – periodically revised recommendations (or guidelines) of the National Academy of Sciences – quantitative estimates of nutrient intakes for planning and assessing diets for healthy people AI: Adequate Intake UL: Tolerable Upper Intake Level EER: Estimated Energy Requirement
 of the National Academy of Sciences – quantitative estimates of nutrient intakes for planning and assessing diets for healthy people AI: Adequate Intake UL: Tolerable Upper Intake Level EER: Estimated Energy Requirement")
9
Infant Feeding Practices Study II Fein, Sara B. et al Pediatrics Vol 122 October 2008 (Supplement) – Data from nationally distributed consumer opinion panel of 500000 households – Mothers of healthy term and late preterm infants – N= 4902 pregnant women, ~2000 continued through infants first year
 – Data from nationally distributed consumer opinion panel of households – Mothers of healthy term and late preterm infants – N= 4902 pregnant women, ~2000 continued through infants first year.")
10
Infant Feeding Practices Study II 83% of survey respondents initiated breastfeeding Declined to 50% at 6 months and 24% at 12 months 52% of breastfed infants received some formula in the hospital 40% received infant cereal at 4 months

11
Infant Feeding Practices Study II Majority of formula feeding mothers did not receive instruction on formula preparation or storage from a health professional (73-77%) 30% did not read safe use instrcutions on package label 55% did not wash hands before bottle prep, 32% did not wash bottle nipples between use, 35% heated bottles in microwave, and 6% did not always discard formula left standing > 2 hours
 30% did not read safe use instrcutions on package label 55% did not wash hands before bottle prep, 32% did not wash bottle nipples between use, 35% heated bottles in microwave, and 6% did not always discard formula left standing > 2 hours")
12
Infant Feeding Practices Study II At 6 months of age 18% of term breastfed and mixed fed infants had not received infant cereal or meat in the previous 7 days. 58% received 3X per week

13
Screening, Assessment, Education

14
Information Collected Growth Dietary Medical history Diagnosis Feeding and developmental information Psychosocial and environmental information Clinical information and appearance (hair, skin, nails, eyes) Other (anthropometrics, laboratory)
 Other (anthropometrics, laboratory)")
15
Nutrition Screening: Purpose To identify individuals who appear to have or be at risk for nutrition problems To identify individuals who require further assessment or evaluation Identify risk and education needs for prevention of nutritional problems

16
Screening: Definition Process of identifying characteristics known to be associated with nutrition problems – ASPEN, Nutri in Clin Practice 1996 (5):217-228 Simplest level of nutritional care (level 1) – Baer et al, J Am Diet Assoc 1997 (10) S2:107-115
: Simplest level of nutritional care (level 1) – Baer et al, J Am Diet Assoc 1997 (10) S2:")
17
Assessment Screening identifies nutritional risk Nutrition Assessment – Uses information gathered in screening – Adds more in depth, comprehensive data – Interprets data – Develops care plan – Reassess

18
Goals of Nutrition Assessment To collect information necessary to document adequacy of nutritional status, identify deficits, and determine etiology of any identifiable problems To develop a nutritional care plan that is realistic and within family context To establish an appropriate plan for monitoring and/or reassessment

19
Assessment Process Linking information collected with: – Goals/expectations – Reference data/standards – Evidence – individual Asking questions

20
CDC Growth Charts: Tool for Screening and Assessment Standardized data collection methods Expanded sample Exclusions – VLBW infants – NHANES III weight data for >6 year olds

21
Challenges

22
Information – Availability, sufficiency, accuracy Interpretation – Goals, expectation, “does it make sense” Questions – What are goals and expectations, “does it make sense”

23
Challenges Nutrient needs influenced by: genetics, activity, body composition, medical conditions and medications Individuals anthropometric date influenced by: genetics, body composition, development, history

24
Considerations Growth in infancy Physiology of infancy GI Renal Infant Development Nutrient requirements * Recommendations Milk based feedings/Infant formulas Timing of complementary foods – What are families actually doing? Specific issues of safety and oral health Challenges: Recommendations for populations v.s individual

25
Challenges Identification of etiology Weighing risk vs benefit Supportive of: – Family – Individual – Development/temperament

26
Assessment Process Linking information collected with: – Goals/expectations – Reference data/standards – Evidence – individual Asking questions

28
Interpretation Linking information collected with: – Goals/expectations – Reference data/standards – Evidence – individual Asking questions

29
Interpretation: Asking Questions Is there a problem? Was there a problem? Does information make sense? What are goals and expectations? What is etiology of the problem?

30
Contributing Factors Inadequate Intake Fluid, energy Medical BPD, reflux, frequent illness Feeding relationship Stress, history Psychosocial

31
Joey

32
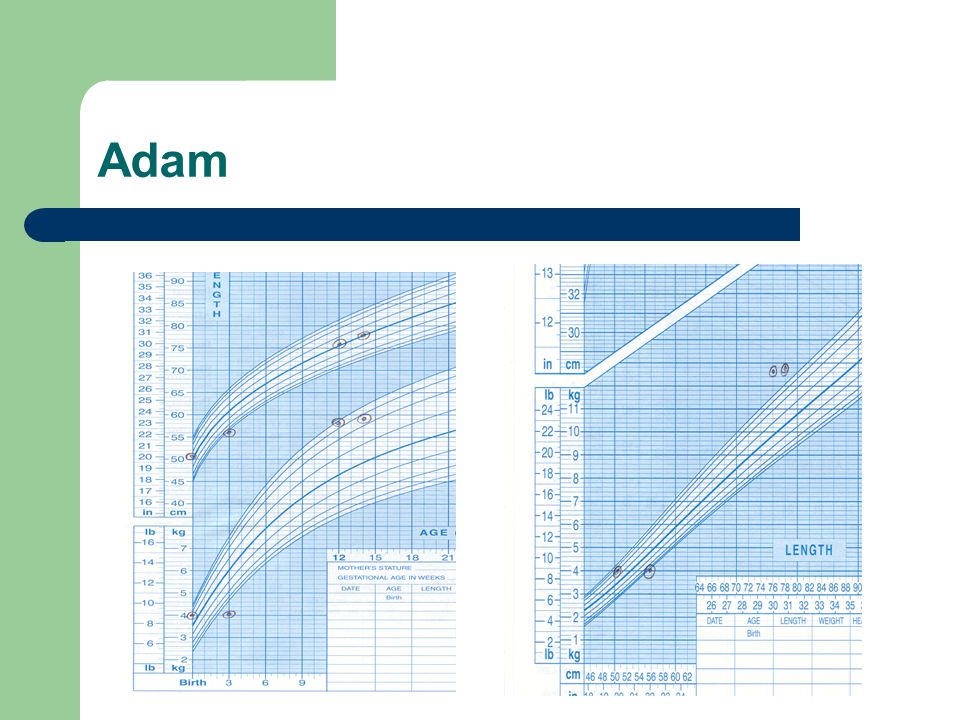
Adam

35
Intervention Identify etiology Identify contributing factors Support feeding relationship Consider psychosocial factors, family choice and input Weigh risk v.s. benefit

36
Intervention Adequate intake vs feeding relationship Concentrating formula vs fluid status Impact on tolerance, compliance, errors, cost Solution to problem vs. exacerbating problem

37
Examples

38
Common Recommendations Breastfeed to at least 1 year Iron fortified cereal by 4-6 months Vitamin D Supplementation Introduce 1 food at a time

39
Screening Risks Weight less than 5 th %ile Weight greater than 90 th %ile Improper or inappropriate food/formula choices or preparation Bottle in bed

40
Jamie 6 months of age Family hx of allergies Mom discontinued breastfeeding when returned to work at 5 months

41
Toby 11 months old FTT Receives formula in bottle. Difficulties with bottle feeding. Likes solids. Takes few jars of stage III fruits, vegetables, dinners per day Advised to avoid milk until baby over 12 months of age (excluded milk, cheese, yogurt, butter)
.")
42
Mattie 10 month old “colicky, irritable” Young mother, lives in small apartment, “thin walls” neighbors complain about noise Baby has 10-12 bottles per day of formula, or juice. Has bottle in bed at nap and night Weight at 75 th %ile, length and 75 th %ile

43
Zoe 8 months old Exclusive breastfeeding Weight and length at 50 th %ile. Hct within normal limits Mom believes breast milk provides all nutrients and offering anything else will result in infant discontinuing or “weaning” from breast

Similar presentations










 WIC’s mission is to safeguard the health of low-income women, infants, and.>")









