Download presentation
Presentation is loading. Please wait.

1
Implementation of WHO Growth Charts & Related Risks for Infants and Children

2
Objectives To explain differences between 2000 CDC growth grids and WHO growth grids To understand the rationale for using WHO growth grids for 0-24 month olds To describe changes to existing risk factors and identify new risk factors To successfully interpret the new WHO growth grids when used in clinic

3
Growth charts are key tools used to interpret growth measurements

4
Activity Discuss at your table: How do you use growth charts? When do you show growth charts to parents? How do you describe the growth charts to parents?

5
History From 1977 to 2000, National Center for Health Statistics (NCHS) charts used worldwide as a growth reference Since 2000, Center for Disease Control (CDC) growth charts used as a growth reference for children ages 0- 20 years April 2006, World Health Organization (WHO) released new international growth standard for children age 0- 5 years
 charts used worldwide as a growth reference Since 2000, Center for Disease Control (CDC) growth charts used as a growth reference for children ages years April 2006, World Health Organization (WHO) released new international growth standard for children age 0- 5 years")
6
Reference Vs. Standard A REFERENCE describes how children have grown in a particular time and place, gives a point of comparison, does not make a value judgment Describes how things are

7
Reference Vs. Standard A STANDARD describes how children should grow regardless of time or place, defines what is normal or optimal, allows for value judgments Describes how things should be

8
CDC Growth Reference Describes growth of children in the U.S. during the 1970s and 1980s Based on data from national surveys and birth certificates No special characteristics were required to be included in the data

9
WHO Growth Standard Frequent data collection from birth to two years of age Large number of observations completed internationally Feeding requirements included: Exclusive/predominant breastfeeding > 4 months Complementary feeding by 6 months Continued breastfeeding > 12 months

10
WHO Growth Standard Optimal Nutrition Breastfed with appropriate complementary feeding Optimal Environment Clean, safe, smoke free Optimal Care Access to immunization and medical care Optimal Growth

11
WHO Growth Standard Hypothesis: Children throughout the world will grow similarly if exposed to optimal circumstances Data collected in: United States Brazil Norway India Oman Ghana

12
Growth patterns from birth to 24 months from the 6 WHO countries

13
Comparison of WHO with CDC Weight-for-Age Percentiles for Girls

14
Recommendations for the U.S. American Academy of Pediatrics (AAP), National Institutes of Health (NIH) and CDC recommend : National use of WHO charts from birth to 2 years Continued use of the CDC charts from 2 years to 20 years USDA accepts recommendations for WIC
, National Institutes of Health (NIH) and CDC recommend : National use of WHO charts from birth to 2 years Continued use of the CDC charts from 2 years to 20 years USDA accepts recommendations for WIC.")
15
Differences between Charts WHO growth standards measured healthy children under optimal conditions so more extreme cutoffs are appropriate for children measured on WHO graphs New cutoffs at the 2 nd and 98 th percentiles on WHO growth charts Continue to use 5 th and 95 th percentiles on CDC growth charts for older children

16
Differences between Charts Fewer infants would be below 5 th percentile on WHO weight-for-age charts Fewer children will be identified as Underweight or Failure to Thrive(FTT), especially from 6 to 23 months More infants would be above 95 th percentile on WHO weight-for-length Formula-fed infants tend to gain weight more rapidly after 3 months and could be identified as overweight
, especially from 6 to 23 months More infants would be above 95 th percentile on WHO weight-for-length Formula-fed infants tend to gain weight more rapidly after 3 months and could be identified as overweight")
17
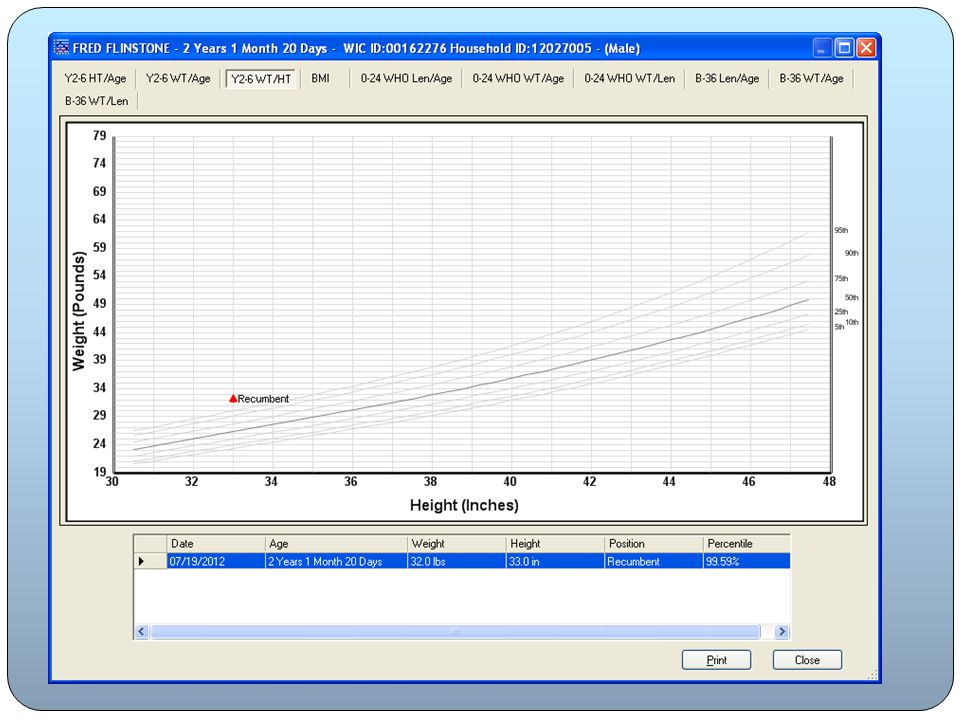
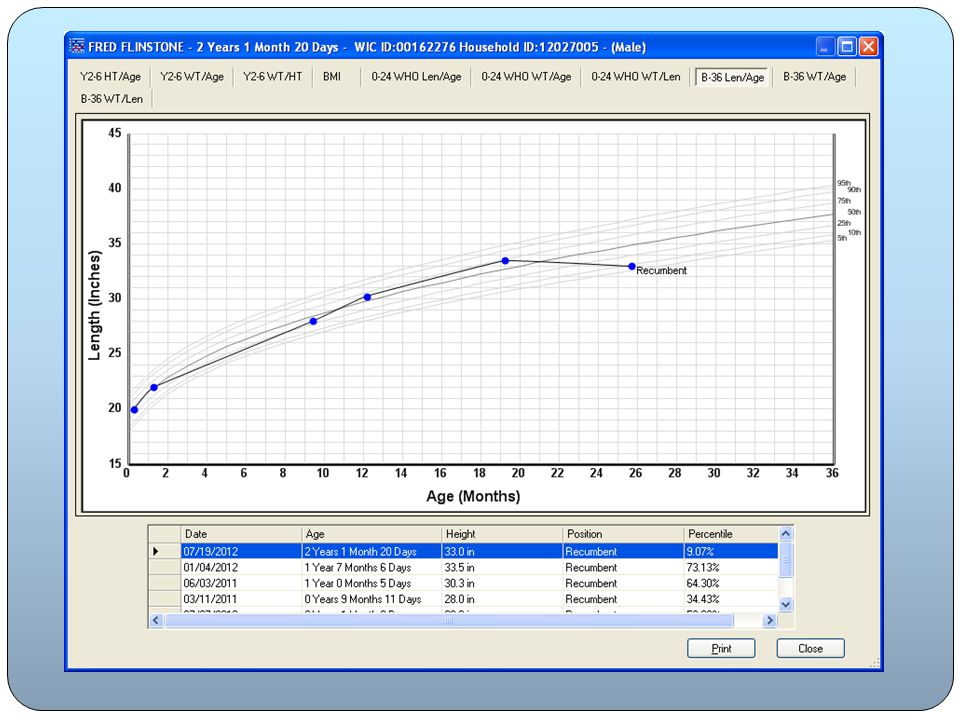
Case Study Compare the following growth charts for Sally, 11 month old infant. What are the differences between the CDC and WHO charts? Measurements for Sally at 3 points in time: AGEWEIGHT (lbs.) LENGTH (in.) WEIGHT-FOR-LENGTH (%) CDCWHO 3 months9.522.17.49%8.11% 7 months13.325.08.92%9.84% 11 months17.028.82.24%7.05%
 LENGTH (in.) WEIGHT-FOR-LENGTH (%) CDCWHO 3 months %8.11% 7 months %9.84% 11 months %7.05%.")
18
Three measurements for Sally plotted on the current CDC chart…

19
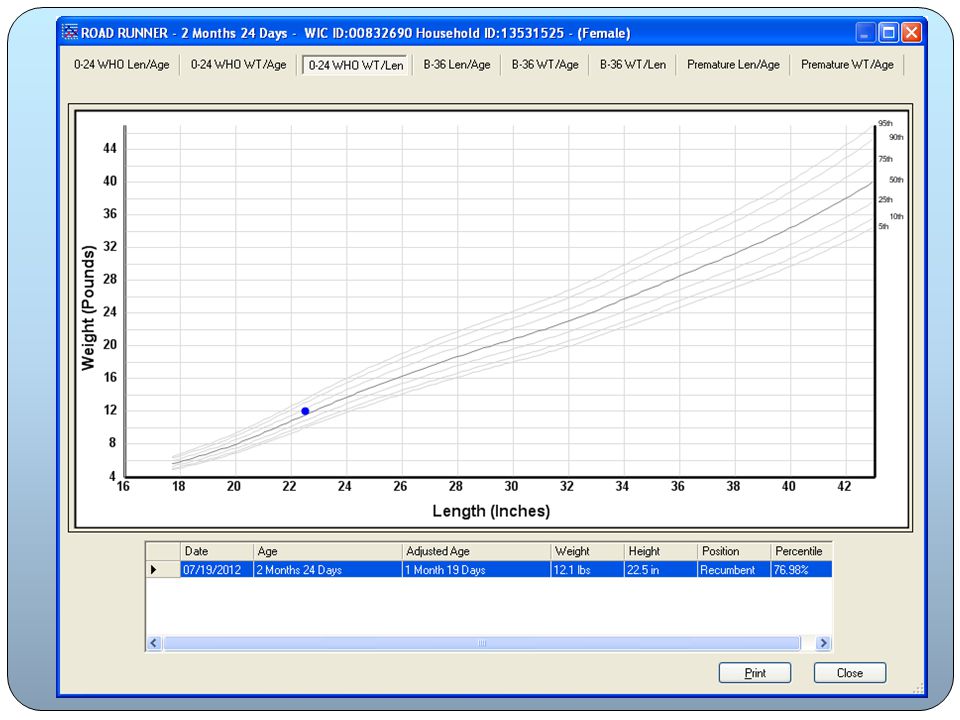
Same three measurements for Sally plotted on the new WHO charts…

20
Recommendations for the U.S. CDC Charts after Age 2 Charts similar for children after 24 months of age CDC charts go through age 19 years Making transition at 2 is practical

21
Minnesota Implementation WHO charts added to HuBERT in November 2012 HuBERT will continue to plot and assign risk factors from the appropriate chart for age: WHO for children from birth to 2 years of age CDC BMI charts for children from 2 to 5 years

22
Minnesota Implementation CDC weight for length charts for children from 2 to 3 years if they cannot be measured standing up B-36 month charts Educational purposes ONLY No Risk Factor assignment

23
WIC Risk Factors Change based on the WHO Growth Charts HuBERT will continue to auto assign risk factors based on information entered on the Height, Weight Blood screen

24
103: Underweight (Infants & Children) Underweight Birth to < 24 months New! < 2.3 rd percentile weight-for-length 2-5 years < 5 th percentile BMI-for-age At Risk of Underweight Birth to < 24 months New! > 2.3 rd percentile and < 5 th percentile weight-for-length 2-5 Years > 5 th percentile and < 10 th percentile BMI-for-age

25
103: High Risk WHO charts Fewer children Indicates significant issue with weight HuBERT assignment continues High Risk follow up needed

26
113: Obese (Children 2-5 years) > 95 th percentile BMI-for-Age ONLY New! Only standing height measurements may be used to assign risk

27
114: Overweight (Children 2-5 years) > 85 th percentile and < 95 th percentile BMI-for-Age Only standing height measurements may be used to assign risk
 > 85 th percentile and < 95 th percentile BMI-for-Age Only standing height measurements may be used to assign risk")
28
114: At Risk Of Overweight < 12 months of age Biological mother with BMI > at time of certification HuBERT will continue to auto-assign when infant record is linked to mother

32
115: High Weight for Length Infants & Children < 24 Months of Age Birth to 24 months of Age > 97.7 th percentile weight-for-length New Risk! YES

33
115: High Risk Only for 12 months and older Based on WHO growth grids with 97.7% threshold HuBERT assignment continues High Risk follow up needed

34
Activity Discuss at your table: What terms do you use when talking to parents about their children’s weight? What questions would you ask to find out more about the child’s family?

35
Talking About Weight Continue to use language that avoids “obese” and “fat” labels Consider use of supportive phrases such as: Monitor weight Watch weight gain Weight higher than average Weight above most children at that age Weight disproportional to height Other?

36
121 Short Stature (Infants & Children) Short Stature Birth to < 24 months: NEW! <2.3 rd percentile length-for-age 2-5 years: < 5 th percentile stature-for-age At Risk of Short Stature Birth to <24 months: NEW! >2.3 rd to <5 th percentile length-for-age 2-5 years: >5 th to <10 th percentile stature-for-age

37
121 Short Stature: Gestational Age Adjustment Assigned after age has been adjusted to correct gestational ages HuBERT will display chronological & age adjusted in table PLOT will only occur at adjusted age Born at 35 weeks; certification at 10 weeks after delivery Plot will occur at 5 weeks of age 40 – 35 = 5 weeks adjustment for prematurity 10 – 5 = 5 weeks gestation adjusted age

41
Premature Growth Grids Plots will display on these grids but NO risk assignment Gestational age & chronological age growth grids Origins of these grids unknown Possibly used for educational purposes with parent but USE WITH CAUTION

44
But wait……. There are three more changes to Risk Factors!

45
Modifications to 3 existing Risk Factors 152: Low Head Circumference (Infants & Children < 24 months of age) 344: Thyroid Disorders 351: Inborn Errors of Metabolism
 344: Thyroid Disorders 351: Inborn Errors of Metabolism")
46
152: Low Head Circumference Birth to < 24 months < 2.3 rd percentile head circumference-for-age Assessed by referral data from health care provider

47
344: Thyroid Disorders Definition, Justification, and Clarification sections are greatly expanded to provide more information about thyroid disorders. Hyperthyroidism Hypothyroidism Congenital Hyperthyroidism Congenital Hypothyroidism Postpartum Thyroiditis

48
351: Inborn Errors of Metabolism Categories now include: Amino Acid Disorders, Urea Cycle Disorders, Organic Acid Metabolism Disorders, Carbohydrate Disorders, Fatty Acid Oxidation Disorders, Peroxisomal Disorders, Lysosomal Storage Diseases, Mitochondrial Disorders Definition, Justification, and Clarification sections are greatly expended to provide more information about inborn errors of metabolism.

49
Nutrition Risk Criteria Found on Minnesota WIC website Expanded definition, clarification and justification of risk factor included New section, Implications for WIC Nutrition Services Highlights key nutrients education messages for each criterion Present in these risk factors Gradually added to all risk factors when updated over time Found at: http://www.health.state.mn.us/divs/fh/wic/localagency/nutritio n/riskcodes/index.html http://www.health.state.mn.us/divs/fh/wic/localagency/nutritio n/riskcodes/index.html

Similar presentations














.>")

 and understand its scope and effects Share who some of the.>")



 including the new growth grids.>")


 What is Body Mass Index (BMI)>")
-for-age Growth Charts: A Training for Health Care Providers Adapted by the CHDP Bay Area Nutrition.>")