Download presentation
Presentation is loading. Please wait.

1
د.ديمه الزعبي معيدة في قسم الأشعة
عملي الأشعه 2013_2014

2
Bone Lesions

3
Fibrous Cortical Defect.
A well-defined lytic lesion is seen in the medial metaphysis of this tibia (arrows), which is typical for a fibrous cortical defect
, which is typical for. a fibrous cortical defect.")
4
Nonossifying Fibroma. A large, well-defined lytic lesion, which is slightly expansile with scalloped sclerotic margins, is seen in the distal tibia in this young patient. This is a characteristic appearance of a nonossifying fibroma. The examination was obtained for a sprained ankle and not for this asymptomatic lesion.

5
Nonossifying Fibroma. A well- defined, expansile lytic lesion in the distal fibula is noted in this asymptomatic patient, which is characteristic for a nonossifying fibroma.

6
Nonossifying Fibroma. A
Nonossifying Fibroma. A. A well-defined, lytic lesion that is minimally expansile is seen in the distal tibia in this child who was examined for a sprained ankle. B. A CT examination showed apparent cortical destruction (arrow), which was believed to be suggestive of an aggressive lesion. Biopsy showed this to be a nonossifying fibroma. Both CT and MR will often show apparent cortical destruction, which is merely cortical replacement by benign fibrous tissue.
, which was believed to be suggestive of an aggressive lesion. Biopsy showed this to be a nonossifying fibroma. Both CT and MR will often show apparent cortical destruction, which is merely cortical replacement by benign fibrous tissue.")
7
Healing Nonossifying Fibroma
Healing Nonossifying Fibroma. A predominantly sclerotic lesion, which is minimally expansile and well defined, is seen in the proximal humerus in this child who is asymptomatic. This is a typical appearance of a disappearing or healing nonossifying fibroma. With time, this lesion will melt into the normal bone and essentially disappear.

8
Nonossifying Fibroma. This large, well- defined lytic lesion with faint sclerotic margins is seen in the distal femur. It has a very typical appearance for a giant cell tumor; however, it has sclerotic margins and does not abut the articular surface. The lesion underwent biopsy and was found to be a nonossifying fibroma.

10
Solitary Bone Cyst. A well-defined lytic lesion, which is central in location, is seen in the proximal femur in this child. This is characteristic for a solitary bone cyst.

11
Solitary Bone Cyst. A well-defined lytic lesion is present in the proximal humerus in this child who suffered a fracture through the lesion. The location and central appearance, as well as the age of the patient, are characteristic for a solitary bone cyst. A piece of cortical bone has broken off and descended through the serous fluid contained within the lesion and can be seen in the dependent portion of the lesion (arrow) as a fallen fragment sign. A fallen fragment sign is said to be pathognomonic for a unicameral bone cyst.
 as a fallen fragment sign. A fallen fragment sign is said to be pathognomonic for a unicameral bone cyst.")
12
Solitary Bone Cyst. A well-defined lytic lesion is seen in the calcaneus abutting the inferior surface, which is typical in location and appearance for a solitary bone cyst. A solitary bone cyst in the calcaneus occurs almost exclusively in this location and is not subject to pathologic fracture as readily as when one occurs in the proximal femur and humerus

14
Aneurysmal Bone Cyst. A well-defined expansile lesion is seen in the midshaft of the ulna in a child who presented with pain in this region. This is a characteristic appearance for an aneurysmal bone cyst.

15
Aneurysmal Bone Cyst. An axial T2WI through a thoracic vertebral body shows an expansile lesion involving the posterior elements that has several fluid–fluid levels (arrows). This is a typical appearance for an aneurysmal bone cyst.

17
Osteoblastoma. A. A lytic expansile lesion involving the right T12 pedicle (arrow) and transverse process is seen on this anteroposterior plain film. B. The lesion is seen on CT to extend into the vertebral body. It has intact cortices and contains some calcified matrix. This is a classic example of an osteoblastoma of the spine.
 and transverse process is seen on this anteroposterior plain film. B. The lesion is seen on CT to extend into the vertebral body. It has intact cortices and contains some calcified matrix. This is a classic example of an osteoblastoma of the spine..")
19
Giant Cell Tumor. A well-defined lytic lesion without a sclerotic margin is seen abutting the articular surface of the distal femur in a patient who has closed epiphyses. These are all characteristics of a giant cell tumor

20
Giant Cell Tumor. A large, well-defined lytic lesion in the iliac wing is seen, which does contain a sclerotic margin and does not appear to abut any articular surface. The pelvis is a good location for giant cell tumor, which this proved to be at biopsy. The usual rules for giant cell tumors such as presence of a nonsclerotic margin do not apply in flat bones

21
Giant Cell Tumor. This well-defined lytic lesion that does not have a sclerotic margin completely involves the greater trochanter. The apophyses have the same differential diagnosis as lesions in the epiphyses , which makes giant cell tumor a strong possibility in this example. Biopsy showed this to be a giant cell tumor.

23
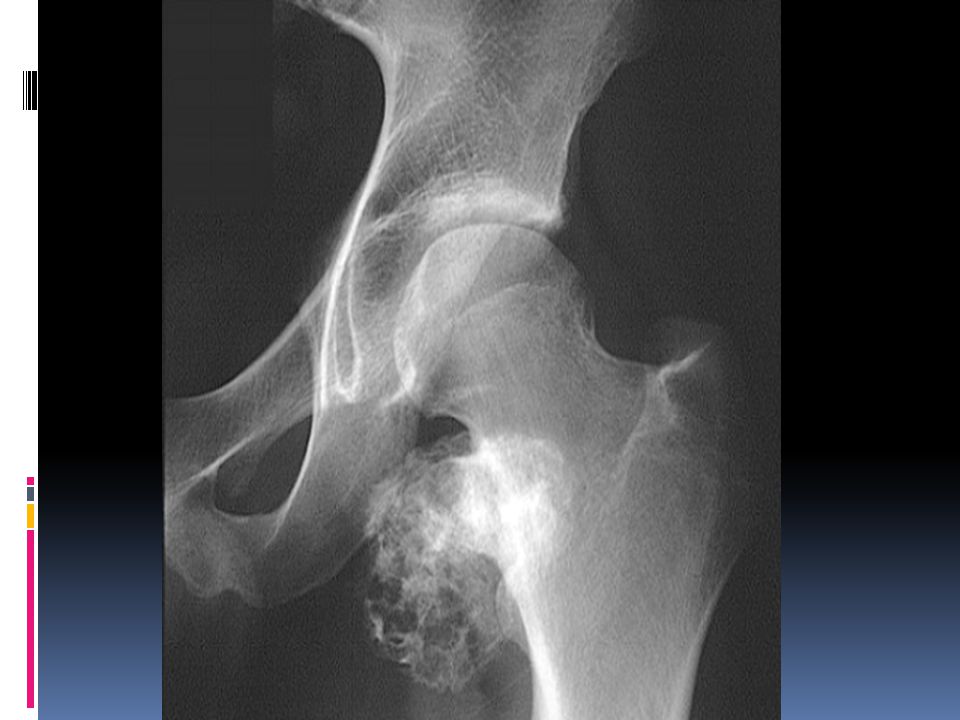
Enchondroma. This lesion in the distal right femur shows the stippled, punctate calcification typical for chondroid matrix seen in an enchondroma.

24
A lytic lesion in the phalanges is most commonly an enchondroma.
This is the only location in the skeleton where an enchondroma does not contain calcified chondroid matrix. These most often present with pathologic fractures, as in this example

25
Ollier Disease. Multiple enchondromas are present throughout the hand.
This is a typical example of Ollier disease.

26
Maffucci Syndrome. Multiple enchondromas associated with phleboliths are present in the phalanges.
This combination of findings invariably represents hemangiomas and enchondromas in Maffucci syndrome

27
On MR imaging bone infarcts are characterized by irregulair serpentiginous margins with low signal intensity on both T1 and T2 WI and with intermediate to high fat signal in the center part. Enhancement after i.v. Gadolinium is usually minimal or absent (see right image). At the periphery of the infarct a zone of relative high signal intensity on T2WI may be found.
. At the periphery of the infarct a zone of relative high signal intensity on T2WI may be found.")
33
Chondromyxoid Fibroma.
A well-defined lytic lesion in the distal tibia that extends slightly into the epiphysis is noted on this anteroposterior plain film. A nonossifying fibroma could certainly have this appearance; however, this underwent biopsy and was found to be a chondromyxoid fibroma. Chondromyxoid fibromas often extend into the epiphysis, as in this example, whereas nonossifying fibromas usually do not.

34
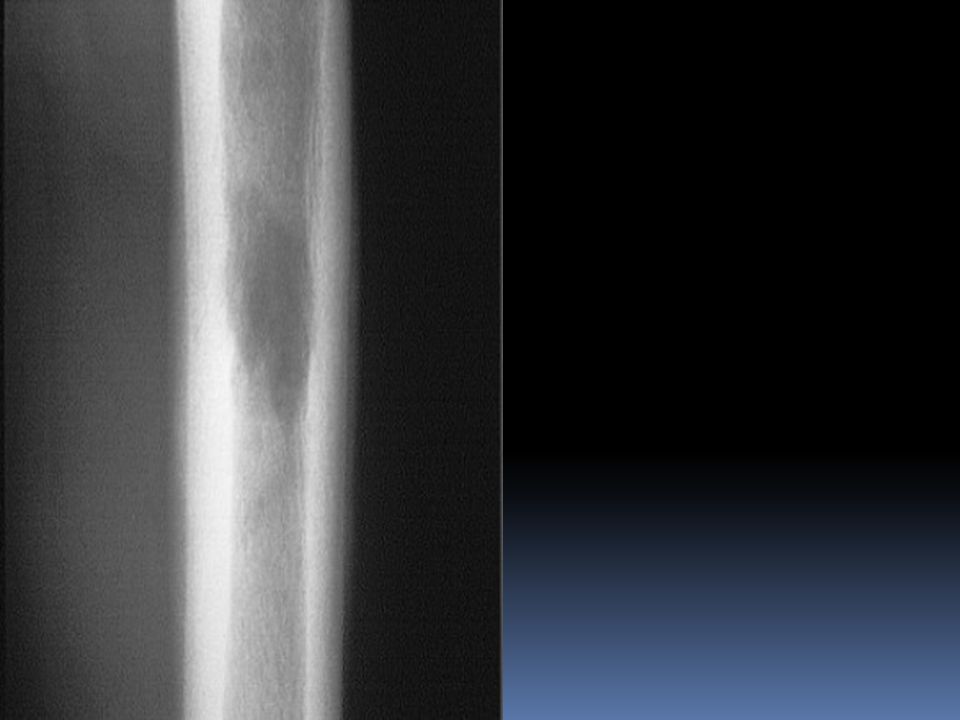
Eosinophilic Granuloma (EG).
A well-defined lytic lesion is seen involving the midfemur in this 20-year-old patient. Biopsy showed this to be EG

36
Eosinophilic Granuloma (EG).
This well-defined lytic lesion contains a bony sequestrum (arrow), which is typical for osteomyelitis or EG. Biopsy revealed this to be EG
, which is typical for osteomyelitis or EG. Biopsy revealed this to be EG.")
37
Fibrous Dysplasia. Polyostotic fibrous dysplasia is seen in the radius in this child. Parts of this lesion have a hazy, ground-glass appearance, whereas others are more lytic appearing. A hazy, ground-glass appearance is often present in fibrous dysplasia, but just as often, the appearance can be purely lytic or even sclerotic.

38
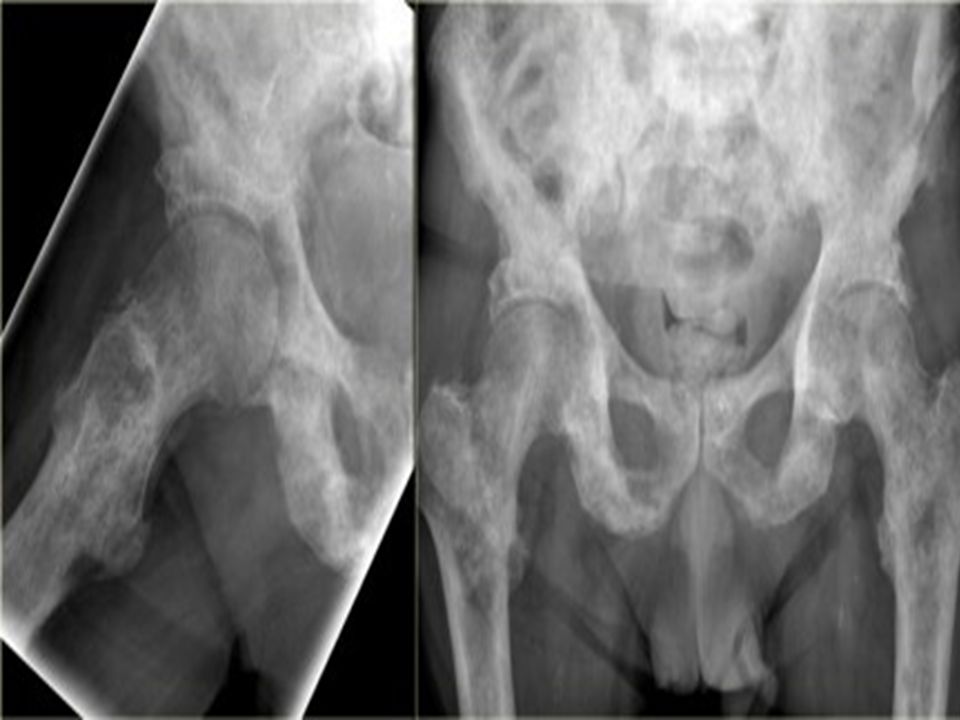
Fibrous Dysplasia. This patient has polyostotic fibrous dysplasia with diffuse involvement of the pelvis as well as the proximal femurs

39
Fibrous Dysplasia. This patient has polyostotic fibrous dysplasia with involvement of the right femur as well as the supraacetabular portion of the ilium. When the pelvis is involved with fibrous dysplasia, the ipsilateral femur on the affected side is invariably also involved

40
Fibrous Dysplasia. This patient has a well-defined lytic lesion with a hazy, ground-glass appearance in the neck of the right femur. The pelvis was uninvolved. It is not unusual for monostotic fibrous dysplasia to involve the proximal femur and spare the pelvis.

41
Fibrous Dysplasia. When fibrous dysplasia affects the ribs, the posterior ribs often demonstrate a lytic expansile appearance, as in this example. When the anterior ribs are involved, they are most often sclerotic in appearance. Note also the involvement of the thoracic spine

42
Chondromyxoid Fibroma
Chondromyxoid Fibroma. A well-defined lytic lesion in the distal tibia that extends slightly into the epiphysis is noted on this anteroposterior plain film. A nonossifying fibroma could certainly have this appearance; however, this underwent biopsy and was found to be a chondromyxoid fibroma. Chondromyxoid fibromas often extend into the epiphysis, as in this example, whereas nonossifying fibromas usually do not.

44
Osteomyelitis. A. A lytic lesion is present in the proximal humerus, which has some associated periostitis laterally. B. CT scan through this area reveals a lytic lesion that contains a calcific density within (arrow), which is a bony sequestrum. This is an area of osteomyelitis with a bony sequestration
, which is a bony sequestrum. This is an area of osteomyelitis with a bony sequestration.")
47
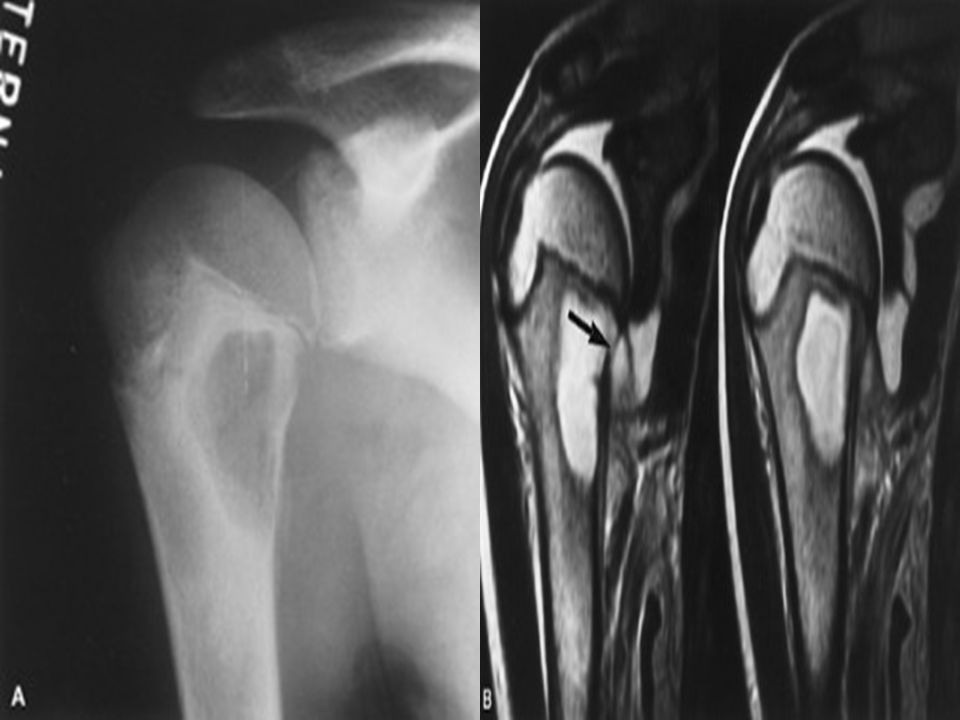
A plain film of the proximal humerus in this child with shoulder pain reveals a well-defined lytic lesion in the medial metaphysis. B. T2WI of the humerus shows the lesion to have high signal and an associated joint effusion. The probable site of connection to the joint can be seen (arrow), which likely represents a draining abscess. Aspiration of the joint fluid revealed pus. This is a large focus of osteomyelitis or Brodie abscess.
, which likely represents a draining abscess. Aspiration of the joint fluid revealed pus. This is a large focus of osteomyelitis or Brodie abscess.")
54
“Ill defined solitary osteolytic lesios can be caused by following entities1 haemangioma chondroblastoma osteoblastoma giant cell tumour fibrosarco...” This is osteo sarcoma

55
Conventional radiography continues to play an important role in diagnosis.
Typical appearances of conventional high grade osteosarcoma include: medullary and cortical bone destruction wide zone of transition, permeative or moth-eaten appearance aggressive periosteal reaction sunburst type Codman triangle lamellated (onionskin) reaction - less frequently seen soft-tissue mass tumour matrix ossification / calcification variable: reflects a combination of the amount of tumour bone production, calcified matrix, and osteoid ill-defined "fluffy" or "cloud-like"
 reaction - less frequently seen. soft-tissue mass. tumour matrix ossification / calcification. variable: reflects a combination of the amount of tumour bone production, calcified matrix, and osteoid. ill-defined fluffy or cloud-like")
59
MULTIPLE MEYLOMA numerous, well circumscribed lytic bone lesions (more common) punched out lucencies e.g. pepperpot skull or raindrop skull 7 endosteal scalloping generalized osteopaenia (less common) often associated with vertebral compression fractures / vertebra plana
 often associated with vertebral compression fractures / vertebra plana.")
61
Chondroblastoma Typical presentation:
well-defined osteolytic lesion in tarsal bone, patella or epiphysis of a long bone in a 20-year old with pain and swelling in a joint. Abundant edema is almost always present. DD: Ganglion cyst, osteomyelitis, GCT, ABC, enchondroma. Here a lesion located in the epi- and metaphysis of the proximal humerus. The lesion is predominantly calcified. Coronal T1W image shows lobulated margins and peripheral low SI due to the calcifications.

62
Here a chondrosarcoma of the left iliac bone.
Because of the large dimensions with soft tissue extension on plain radiograph and axial T2-weighted MR image, a high grade chondrosarcoma was suspected. Biopsy showed grade 2 chondroarcoma.

Similar presentations


























>")





 By : Dwi Damar Andriyani Consultant : dr. Edy Moeljono, Sp.Rad (K)RA TEXT BOOK READING DAVID SUTTON VOL.2 PAGE 1130-1140.>")








