Download presentation
Presentation is loading. Please wait.

1
Dan Preece DPM PGY-2

2
HPI: 9 yo healthy male with dorsal right foot pain. Duration of pain x 3 months. Hx of multiple episodes of blunt trauma to right foot. Mass noted with swelling dorsal right foot, pain 7/10, some night pain, CAM boot failed to resolve pain, dorsal mass appears to enlarging. PE: painful palpable mass over Right 1st met base. L and R feet asymmetric. No erythema, ulceration, rash. Remainder of exam is consistent with healthy 9 yo male.

6
What other imaging? Differential? Treatment options?

7
Findings: diffuse edema within the proximal 1st metatarsal with diffuse periostitis. There are periosteal or subcortical cystic lesions which are felt to represent superiosteal hematoma or seroma given the pt’s hx of repeated injury to this location. Short interval f/u is recommended as there are additional lesions which could have this appearance. Repeat imaging recommended in 3-6 months, with and w/o contrast.

8
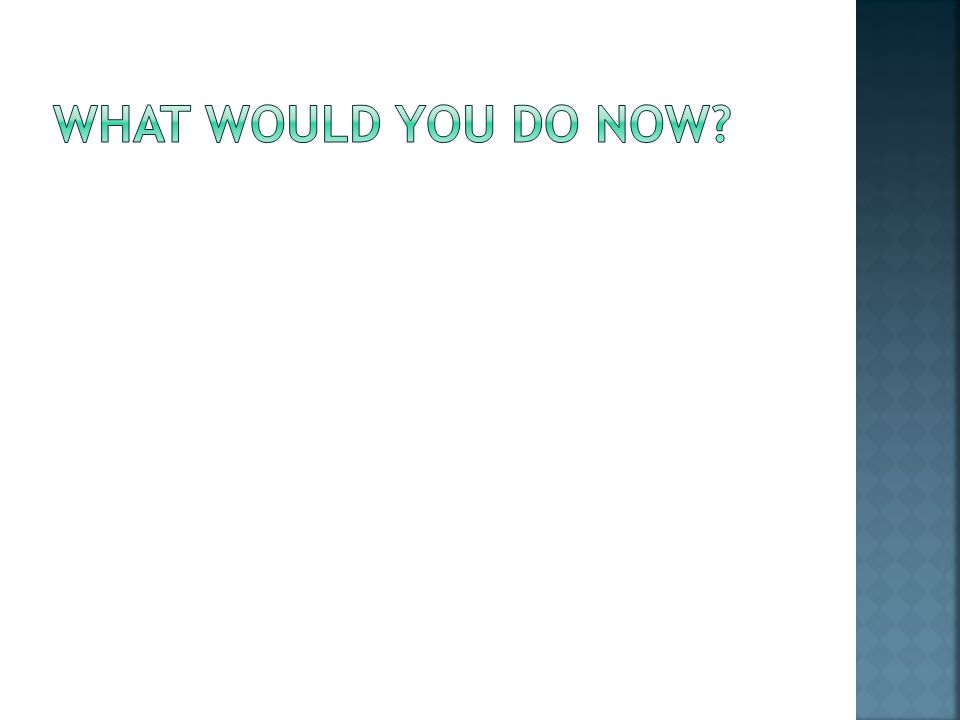
Pain worsening, Right foot mass enlarging clinically. CAM walker failed to relieve pain. No other changes to health status. What are you going to do now?

9
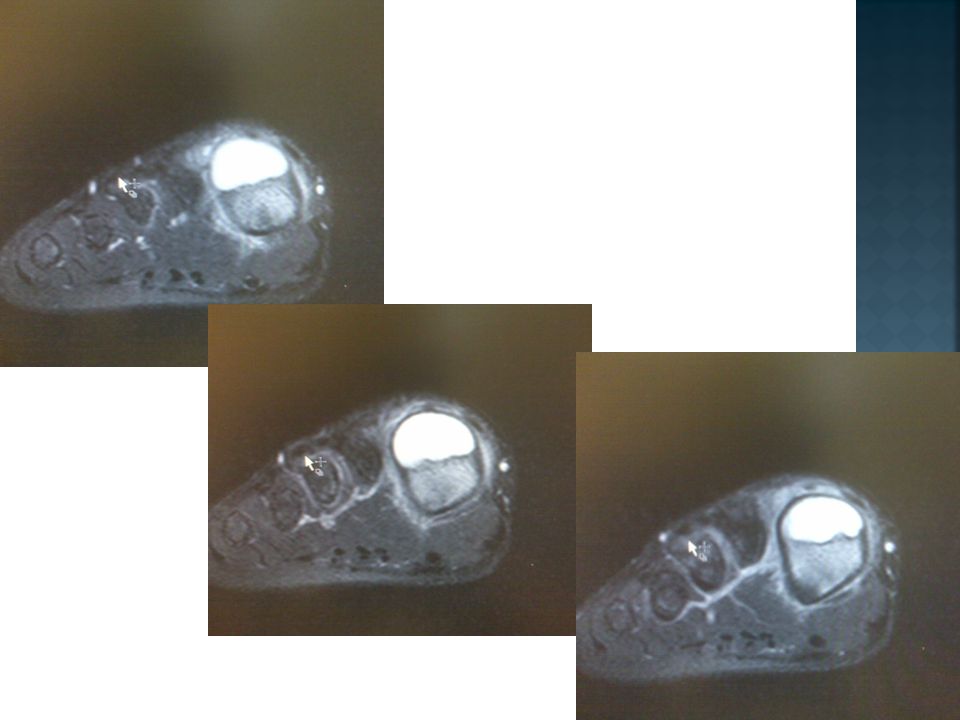
2 nd MRI 3 months later (April 2011):
:")
18
T2 hyperintense expansile proximal met eccentric lesion abutting the dorsal growth plate of the 1 st met. Regional periosteal thickening present. Prominent marrow edema and enhancement. Lesion measures 2 x 1.2 cm, increased from 1.6 x 1.7 cm. Diff: chronic intraosseous abscess or unusual unicameral bone cyst w/ inflammatory changes (less likely). The expansion and peripheral location could be seen w/ aneurysmal bone cyst but single internal cavity is not typical of that Dx. Surgical evaluation should be considered.
. The expansion and peripheral location could be seen w/ aneurysmal bone cyst but single internal cavity is not typical of that Dx. Surgical evaluation should be considered..")
20
Debridement, curettage. Care taken to preserve growth plate. Packed deficit with: Osteosponge (Bacterin) Osteosponge: 100% bone Osteoconductive Osteoinductive Elastic, sponge-like properties Radiolucent Complements orthopedic applications
 Osteosponge: 100% bone Osteoconductive Osteoinductive Elastic, sponge-like properties Radiolucent Complements orthopedic applications.")
23
Op report: appearance of intraosseous ganglion cyst, gelatinous fluid aspirated, dorsal cortex discovered fractured with aspects absent, growth plate not penetrated or affected by mass. Path: sent to Mayo Clinic and UoU by pathology for consultation: Dx: benign chondromyxoid fibroma. Fluid Cytology: No malignant cells.

24
30 days s/p surgery, walking in boot, no pain. X-rays show incorporation of graft, no pathologic fx or recurrence of lesion.

25
Rare, benign, cartilage-forming tumor of the tubular long bones. Clinical Features — usually presents in the teens or 20s. Approximately one-quarter of cases occur in the proximal tibia, distal femur and calcaneus next most common sites. Males affected 1.5 times as often as females. Symptoms include pain and swelling. Radiographic Findings — eccentric, intramedullary, lobulated or bubbly lesion in the metaphysis; it has a sclerotic border. It typically is lucent, with a rare chondral matrix. Differential Diagnosis — Nonossifying fibroma, aneurysmal bone cyst, chondroblastoma, osteomyelitis, fibrous dysplasia. Treatment — curettage and bone grafting. Prognosis — generally is good. There is a 20 percent risk of recurrence, which may require en bloc resection. Source: Up To Date

Similar presentations













>")












>")



