Download presentation
Presentation is loading. Please wait.

1
ECPSLLC.COM O (843) F (843)
 F (843)")
2
Anxiety Spectrum Updates 2012
Ricardo J. Fermo, MD Medical Director East Cooper Psychiatric Solutions, LLC 1073 B. Johnnie Dodds Blvd. Mount Pleasant, South Carolina 29464 Diplomate of the American Board of Psychiatry and Neurology Diplomate of American Board of Child and Adolescent Psychiatry DATE: Friday, May 4th 8:30 AM - 10:30 AM Location: Palmetto Lowcountry Behavioral Health, 2777 Speissegger Drive, North Charleston, SC 29405 Presentation: Anxiety Spectrum Updates
Presenter: Ricardo Fermo, MD Dr. Fermo is a dual board certified psychiatrist with a Diplomate of the American Board of Psychiatry and Neurology and Diplomate of the American Board of Child and Adolescent Psychiatry. Dr. Fermo has been practicing psychiatry for 21 years and has a strong background in evaluating, diagnosing and treating child to adult psychiatric disorders. He specializes in early childhood and adult conditions such as attention deficit hyperactivity disorder, affective disorders such as clinical depression and bipolar, psychotic, and anxiety disorders, substance use related disorders, autism spectrum and behavioral disorders. Dr. Fermo completed an internship at Robert Wood Johnson University Hospital in South Jersey, residency in General Psychiatry at the University of Cincinnati, and Clinical Fellowship in Child and Adolescent Psychiatry at the University of Cincinatti. Dr. Fermo practices Adult/Child and Adolescent Psychiatry at East Cooper Psychiatric Solutions, LLC in Mt. Pleasant. Program Description:
This session will provide updates on the Anxiety Spectrum in regards to : Epidemiology Evidence Based Medicine Diagnostic Criteria If you have questions, please contact Stacey Lindbergh at or

3
FINANCIAL DISCLOSURES/CONFLICTS OF INTEREST
Abbott Laboratories AstraZeneca Bristol Myer-Squibb Cephalon Eli Lilly & Co. Forest Laboratories, Inc. GalaxoSmithKline Janssen Research Jazz Pharmaceuticals Mallinckrodt Merck Novartis Palmlabs Pfizer, Inc. Sanofi Aventis Sepacor Inc. Shire Pharmaceuticals Somaxon Pharmaceuticals Sunovion Pharmaceuticals Inc. Takeda UCB Pharma Inc. Wyeth Pharmaceuticals ECPSLLC.COM

4
Learning Objectives Review updates on the epidemiology of Anxiety
Provide a summary of the disease state (s) Discuss diagnostic criteria for various anxiety disorders Treatment/Goals Discuss evidence-based approaches for treatment-Anxiety Epidemiology Evidence Based Medicine Diagnostic Criteria ECPSLLC.COM
 Discuss diagnostic criteria for various anxiety disorders. Treatment/Goals. Discuss evidence-based approaches for treatment-Anxiety. Epidemiology. Evidence Based Medicine. Diagnostic Criteria ECPSLLC.COM.")
5
References NIMH SAMHCA APA CDC CLINICALTRIALS.GOV CLINICAL PRACTICE
EVIDENCE BASED MEDICINE WEBSITES GOOGLE SCHOLAR COCHRANE PUBMED DYNAMED EVIDENCE BASED (BMJ)
")
6
www.adaa.org www.ocfoundation.org www.socialanxietysupport.com

8
Stress and anxiety are the same thing. True False
Stress is your response to a change in your environment, be it positive or negative. Your body reacts to change -- falling in love, starting a new job, or suffering an unexpected loss -- with physical, mental, and emotional responses. Anxiety is an emotion that’s characterized by a feeling of apprehension, nervousness, or fear.

9
The causes of stress are essentially the same for everyone. True False
YOUR ANSWER: False Something that causes stress for you may not for someone else. Something that's a source of negative stress for one person -- such as a deadline -- might actually be helpful for someone else.

10
Anxiety is the most common mental illness in the US:
True False About 40 million American adults (18 and older) are affected by anxiety disorders each year. That's about 18% of the adult population.
 are affected by anxiety disorders each year. That s about 18% of the adult population.")
11
Men are twice as likely to have Generalized Anxiety then Woman?
True False Women are twice as likely as men to be affected by generalized anxiety disorder, which is characterized by at least six months of excessive, unrealistic worry over everyday problems.

12
What percentage of people with mental illnesses improve if they receive treatment?
25% to 45% 50% to 70% 70% to 90% Between 70% and 90% of people with mental illnesses have an improved quality of life if they receive appropriate treatment and support. However, only about a third of people who are ill receive treatment.

13
Anxiety as a Normal and an Abnormal Response
Some amount of anxiety is “normal” and is associated with optimal levels of functioning. Only when anxiety begins to interfere with social or occupational functioning is it considered “abnormal.”

14
ANXIETY DISORDERS Anxiety is a normal reaction to stress and can actually be beneficial in some situations. Fear and anxiety are part of life anxiety can become excessive, and while the person suffering may realize it is excessive they may also have difficulty controlling it and it may negatively affect their day-to-day living. Most common of emotional disorders Affects more than 40 million Americans The most prevalent psychiatric disorders Anxiety disorders are the most common of emotional disorders and affect more than 25 million Americans. Many forms and symptoms may include: • Overwhelming feelings of panic and fear • Uncontrollable obsessive thoughts • Painful, intrusive memories • Recurring nightmares • Physical symptoms such as feeling sick to your stomach, “butterflies” in your stomach, heart pounding, startling easily, and muscle tension

15
The Fear and Anxiety Response Patterns
Panic Anxiety Anxiety Disorder

16
Definition of Anxiety Anxiety is a feeling of apprehension or fear. The source of this uneasiness is not always known or recognized, which can add to the distress you feel. Anxiety disorders are a group of psychiatric conditions that involve excessive anxiety.

17
2003 Anxiety Disorders Association of America
Anxiety Facts Most common mental illness in the U.S. with 18 million of the adult (ages 18-54) U.S. population affected. Anxiety disorders cost more than $42 billion a year. More than $22 billion are associated with the repeated use of healthcare services, as those with anxiety disorders seek relief for symptoms that mimic physical illnesses. Anxiety is highly treatable (up to 90% of cases), but only one-third of those who suffer from it receive treatment People with an anxiety disorder are three-to-five times more likely to go to the doctor and six times more likely to be hospitalized for psychiatric disorders than non-sufferers. Depression often accompanies anxiety disorders 2003 Anxiety Disorders Association of America
 U.S. population affected. Anxiety disorders cost more than $42 billion a year. More than $22 billion are associated with the repeated use of healthcare services, as those with anxiety disorders seek relief for symptoms that mimic physical illnesses. Anxiety is highly treatable (up to 90% of cases), but only one-third of those who suffer from it receive treatment. People with an anxiety disorder are three-to-five times more likely to go to the doctor and six times more likely to be hospitalized for psychiatric disorders than non-sufferers. Depression often accompanies anxiety disorders Anxiety Disorders Association of America.")
18
Anxiety Facts Anxiety disorders are the most common mental illness in the U.S., affecting 40 million adults in the United States age 18 and older (18% of U.S. population). Anxiety disorders are highly treatable, yet only about one-third of those suffering receive treatment. Anxiety disorders cost the U.S. more than $42 billion a year, almost one-third of the country's $148 billion total mental health bill, according to "The Economic Burden of Anxiety Disorders," a study commissioned by ADAA (The Journal of Clinical Psychiatry, 60(7), July 1999). More than $22.84 billion of those costs are associated with the repeated use of health care services; people with anxiety disorders seek relief for symptoms that mimic physical illnesses.
. Anxiety disorders are highly treatable, yet only about one-third of those suffering receive treatment. Anxiety disorders cost the U.S. more than $42 billion a year, almost one-third of the country s $148 billion total mental health bill, according to The Economic Burden of Anxiety Disorders, a study commissioned by ADAA (The Journal of Clinical Psychiatry, 60(7), July 1999). More than $22.84 billion of those costs are associated with the repeated use of health care services; people with anxiety disorders seek relief for symptoms that mimic physical illnesses.")
19
Anxiety disorders in the U.S. cost more than $42 billion each year.
1/3 of the total amount spent on mental health care

20
Anxiety Disorders One-quarter of the U.S. population experiences pathologic anxiety in their lifetime People with an anxiety disorder are three to five times more likely to go to the doctor and six times more likely to be hospitalized for psychiatric disorders than those who do not suffer from anxiety disorders. Anxiety disorders develop from a complex set of risk factors, including genetics, brain chemistry, personality, and life events. Anxiety and Depression It's not uncommon for someone with an anxiety disorder to also suffer from depression or vice versa. Nearly 70 % of those diagnosed with depression are also diagnosed with an anxiety disorder. Presenting problem for 11% of patients visiting primary care physicians 90% of patients with anxiety present with somatic complaints

21
Anxiety Nervousness and fear are common human emotions.
Adaptive at lower levels; disabling at high levels. Physicians must recognize the difference between pathological anxiety and anxiety as a normal or adaptive response.

22
Definition of Anxiety Diffuse, unpleasant, vague sense of apprehension
Often accompanied by autonomic symptoms such as headache, perspiration, heart palpitations, chest tightness, stomach discomfort and restlessness Presentation depends on perception of stress, personal resources, psychological defenses, and coping mechanisms

23
Pathological Anxiety Anxiety that is excessive, persistent, easily triggered. Degree of the person’s fear is out-of-proportion to actual danger. Disrupts the person’s life and functioning. Creates intense discomfort. Doesn’t respond to rational reassurance. in pathological anxiety, attention is focused also on the person's response to the threat.

24
Features of Pathologic Anxiety
Autonomy: no or minimal environmental trigger Intensity: exceeds patient’s capacity to bear the discomfort Duration: symptoms are persistent Behavior: anxiety impairs coping and results in disabling behaviors

25
Etiology Neurophysiology Cognitive-Behavioral Formulations
Central noradrenergic systems– in particular, the locus coeruleus is the major source of adrenergic innervation GABA neurons from the limbic system Serotoninergic systems and neuropeptides Cognitive-Behavioral Formulations Developmental (Psychodynamic) Formulations
 Formulations.")
26
Common Medical Conditions Associated with Anxiety Disorders
Endocrine: thyroid dysfunction, hyper adrenalism Drug Intoxication: caffeine, cocaine Drug Withdrawal: alcohol, narcotics Hypoxia: CHF, angina, anemia, COPD Metabolic: acidosis, hyperthermia Neurological: seizures, vestibular dysfxn

30
Lifetime Prevalence of Common Psychiatric Disorders
Major depressive disorder1 17.1% Alcohol dependence1 14.1% Social anxiety disorder1 13.3% Posttraumatic stress disorder (PTSD)2 7.8% Generalized anxiety disorder (GAD)1 5.1% Panic disorder1 3.5% Obsessive-compulsive disorder (OCD)3 2.5% 2 4 6 8 10 12 14 16 18 Prevalence (%) *In menstruating women. Kessler RC, et al. Arch Gen Psychiatry. 1994;51(1): Kessler RC, et al. Arch Gen Psychiatry. 1995;52(12): DSM-IV-TR 29 of 45
2. 7.8% Generalized anxiety. disorder (GAD)1. 5.1% Panic disorder1. 3.5% Obsessive-compulsive. disorder (OCD)3. 2.5% Prevalence (%) *In menstruating women. Kessler RC, et al. Arch Gen Psychiatry. 1994;51(1): Kessler RC, et al. Arch Gen Psychiatry. 1995;52(12): DSM-IV-TR of 45.")
31
40 million American adults age 18 years and older (about 18%)
Anxiety Disorders affect about 40 million American adults age 18 years and older (about 18%) in a given year,1 causing them to be filled with fearfulness and uncertainty. Unlike the relatively mild, brief anxiety caused by a stressful event (such as speaking in public or a first date), anxiety disorders last at least 6 months and can get worse if they are not treated. Anxiety disorders commonly occur along with other mental or physical illnesses, including alcohol or substance abuse, which may mask anxiety symptoms or make them worse. In some cases, these other illnesses need to be treated before a person will respond to treatment for the anxiety disorder
 in a given year,1 causing them to be filled with fearfulness and uncertainty. Unlike the relatively mild, brief anxiety caused by a stressful event (such as speaking in public or a first date), anxiety disorders last at least 6 months and can get worse if they are not treated. Anxiety disorders commonly occur along with other mental or physical illnesses, including alcohol or substance abuse, which may mask anxiety symptoms or make them worse. In some cases, these other illnesses need to be treated before a person will respond to treatment for the anxiety disorder.")
32
Generalized Anxiety Disorder Obsessive-Compulsive Disorder (OCD)
Panic Disorder Post-Traumatic Stress Disorder (PTSD) Social Phobia (or Social Anxiety Disorder) Specific Phobia Each anxiety disorder has different symptoms, but all the symptoms cluster around excessive, irrational fear and dread. Each anxiety disorder has different symptoms, but all the symptoms cluster around excessive, irrational fear and dread. Fear and anxiety are part of life. You may feel anxious before you take a test or walk down a dark street. This kind of anxiety is useful - it can make you more alert or careful. It usually ends soon after you are out of the situation that caused it. But for millions of people in the United States, the anxiety does not go away, and gets worse over time. They may have chest pains or nightmares. They may even be afraid to leave home. These people have anxiety disorders.
 Social Phobia (or Social Anxiety Disorder) Specific Phobia. Each anxiety disorder has different symptoms, but all the symptoms cluster around excessive, irrational fear and dread. Each anxiety disorder has different symptoms, but all the symptoms cluster around excessive, irrational fear and dread. Fear and anxiety are part of life. You may feel anxious before you take a test or walk down a dark street. This kind of anxiety is useful - it can make you more alert or careful. It usually ends soon after you are out of the situation that caused it. But for millions of people in the United States, the anxiety does not go away, and gets worse over time. They may have chest pains or nightmares. They may even be afraid to leave home. These people have anxiety disorders.")
33
Explaining anxiety disorders
Learning perspective Biological perspective

34
Learning perspective Fear conditioning Stimulus generalization
One bad event can lead to classical conditioning of fear Stimulus generalization Fear may broaden: fear of heights fear of airplanes Guy who got bit by spider and became arachnophobic

35
Learning perspective Reinforcement can help maintain fears.
Avoiding or escaping the feared situation reduces anxiety, so the avoiding or escaping behavior is reinforced Can anyone give an example?

36
Learning perspective Observational learning
We learn our fears by watching and listening to others Example of parent-instilled fear? Roommate banging tooth on beer bottle

37
Biological perspective
We are biologically prepared to fear threats faced by ancestors Spiders Snakes Darkness

38
Biological perspective
Genes Some people seem genetically predisposed to particular fears and high anxiety 35 year old identical twins

39
Biological perspective
35 year old identical twins who independently developed claustrophobia and fear of water

40
Biological perspective
Physiology Brain scans of people with OCD unusually high activity in certain parts of the frontal lobes

41
Physiology Generalized anxiety, panic attacks, and OCD are linked with overarousal in brain areas linked with impulse control and habitual behaviors People cannot “turn off” these thoughts.

42
Physical Reaction to Anxiety
Auditory and Visual Stimuli: sights and sounds are processed first by the thalamus, which filters the incoming cues and shunts them either directly to the amygdala or to the other parts of the cortex. Olfactory and tactile stimuli: Smells and touch sensations Bypass the thalamus altogether, Taking a shortcut directly to the Amygdala. Smells, therefore, Often evoke stronger memories Or feelings than do sights or Sounds.

43
Physical Reaction to Anxiety
Thalamus: The hub for sights and sounds, The thalamus breaks down Incoming visual ques by size, Shape and color, and auditory Cues, by volume and Dissonance, and then signals The appropriate part of the Cortex. Cortex: It gives raw sights and sounds meanings, enabling the brain to become conscious of what it Is seeing or hearing. One region, the prefrontal cortex, may be vital to turning off the anxiety response once a threat has passed.

44
Physical Reaction to Anxiety
Amygdala: emotional core of the brain, the amygdala has the primary role of triggering the fear response. information that passes through the amygdala is tagged with emotional significance. Bed Nucleus of Stria Terminalis: unlike the Amygdala, which sets off an immediate burst of fear, the BNST perpetuates the fear response, causing the longer term unease typical of anxiety.

45
Physical Reaction to Anxiety
Locus Ceruleus: It receives signals from the amygdala and is responsible for initiating many of the classic anxiety responses: rapid heartbeat, increased blood pressure, sweating and pupil dilation. Hippocampus: This is the memory center, vital to storing the raw information coming in from the senses along with the emotional baggage attached to the data during their trip through the amygdala.

46
Generalized Anxiety Disorder: Biological Causal Factors
Genetic factors A functional deficiency of GABA Neurobiological differences between anxiety and panic

47
Relationship Between Arousal (anxiety) and Performance
Yerkes-Dodson Law 47

48
Three Components of Anxiety
Physical Psychological (Cognition and emotion) Behaviours
 Behaviours.")
49
The Physical Component
Trembling, twitching ,Shaking Dizziness Numbness/Tingling Backache, headache Muscle tension Shortness of breath, hyperventilation Fatigability Startle response Difficulty swallowing Autonomic hyperactivity: Flushing and pallor Tachycardia, palpitation Sweating Cold hands Diarrhea Dry mouth (xerostomia) Urinary frequency Blurred Vision
 Urinary frequency. Blurred Vision.")
51
The Psychological Component
Anxious Thoughts Anxious Predictions Anxious Beliefs and Interpretations Difficulty in Attention and Memory Mental Images Unreality/Detachment Hypervigilance Insomnia Decreased libido Lump in the throat

52
The Behavioural Component
Avoidance of Situations and Activities Subtle Avoidance Strategies, Safety Signals, and Overprotective Behaviours Alcohol, Drug, and Medication Use

53
Anxiety Disorders - DSM-IV
1. Generalized Anxiety Disorder (GAD) 2. Panic Disorder (PD) with Agoraphobia (AG) 3. PD without Agoraphobia 4. Specific Phobia (SP) 5. Social Phobia (SoP) 6. Obsessive Compulsive Disorder (OCD) 7. Post traumatic Stress Disorder (PTSD) 8. Acute Stress Disorder (ASD) 9. Substance-Induced Anxiety disorder (SIAD) 10. Anxiety disorder due some medical illness Dual Diagnosis Disorders
 2. Panic Disorder (PD) with Agoraphobia (AG) 3. PD without Agoraphobia. 4. Specific Phobia (SP) 5. Social Phobia (SoP) 6. Obsessive Compulsive. Disorder (OCD) 7. Post traumatic Stress. Disorder (PTSD) 8. Acute Stress Disorder. (ASD) 9. Substance-Induced. Anxiety disorder (SIAD) 10. Anxiety disorder due. some medical illness. Dual Diagnosis Disorders.")
54
Panic disorder with agoraphobia Phobic anxiety disorder
Anxiety disorders Continuous anxiety Episodic anxiety Generalized anxiety disorder Mixed pattern In any situation In defined situation Panic disorder with agoraphobia Panic disorder Phobic anxiety disorder Simple phobia Social phobia Agoraphobia

55
Epidemiology Overall, anxiety disorders are among the most prevalent of psychiatric disorders. Age; Earlier onset than depression Sex factor; More in females Frequency (Prevalence): 18 %of general population 28% (life time prevalence) Strong genetic component 55
: 18 %of general population. 28% (life time prevalence) Strong genetic component. 55.")
56
Shared features of anxiety disorders
Substantial proportion of aetiology is stress related. Difference with Psychosis - free of delusions and hallucinations, good insight - Reality testing is intact. Symptoms are ego dystonic (distressing) Disorders are enduring or recurrent. Demonstrable organic factors are absent Note: Hierarchy of Diagnosis Precedence: Psychosis >Depression >Anxiety
 Disorders are enduring or recurrent. Demonstrable organic factors are absent. Note: Hierarchy of Diagnosis Precedence: Psychosis >Depression >Anxiety.")
57
Risk Factors/Etiology
Psychodynamic theory posits that anxiety occurs when instinctual drives arc thwarted (dissatisfied). Behavioral theory states that anxiety is a conditioned response to environmental stimuli originally paired with a feared situation. Cognitive approach: Selective attention and catastrophic thinking Biologic theories implicate various neurotransmitters (especially: gamma-aminobutyric acid [GABA], norepinephrine, and serotonin) and various CNS structures (especially reticular activating system and limbic system). Other theories: Social and personality factors.
. Behavioral theory states that anxiety is a conditioned response to environmental stimuli originally paired with a feared situation. Cognitive approach: Selective attention and catastrophic thinking. Biologic theories implicate various neurotransmitters (especially: gamma-aminobutyric acid [GABA], norepinephrine, and serotonin) and various CNS structures (especially reticular activating system and limbic system). Other theories: Social and personality factors.")
58
The Psychodynamic Approach to Anxiety
Anxiety is a signal that the ego is having a hard time mediating between reality, id and superego. Different anxiety disorders are the result of different defense mechanisms used to cope. Phobia - displacement OCD - reaction formation, undoing PTSD - denial, repression Attachment Theories : Bowlby disturbances in parent-child bond leads to “anxious attachment” and a vulnerability to anxiety disorders later in life.

59
The Behavioural Approach to Anxiety (learning theory)
Behavioral theories:- anxiety is a conditional response to specific environmental stimuli followed by its generalization, displacement, or transference. It may be learned through identification and imitation of anxiety pattern in parents (social learning theory). Mowrer (1948) Avoidance learning (learned behaviour) 1) classical (respondent) conditioning 2) negative reinforcement
. Mowrer (1948) Avoidance learning (learned behaviour) 1) classical (respondent) conditioning. 2) negative reinforcement.")
60
The Cognitive Approach to Anxiety
Individuals misperceive and misinterpret internal and external stimuli. Selective attention and catastrophic thinking Cognitive Appraisal (perceive threat) Stimulus--->Appraisal---> Response evaluation of stimulus based on memories, beliefs, and expectations. . Albert Ellis identified basic irrational assumptions: It is necessary for humans to be loved by everyone It is catastrophic when things are not as one wants them to be If something is dangerous, a person should be terribly concerned and dwell on the possibility that it will occur One should be competent in all domains to be a worthwhile person The idea is, when these assumptions are applied to everyday life, GAD may develop. Aaron Beck :Those with GAD hold unrealistic silent assumptions that imply imminent danger: Any strange situation is dangerous A situation/person is unsafe until proven safe Individuals misperceive and misinterpret internal and external stimuli. Selective attention and catastrophic thinking Cognitive Appraisal (perceive threat) Stimulus--->Appraisal---> Response evaluation of stimulus based on memories, beliefs, and expectations. . Albert Ellis identified basic irrational assumptions: It is necessary for humans to be loved by everyone It is catastrophic when things are not as one wants them to be If something is dangerous, a person should be terribly concerned and dwell on the possibility that it will occur One should be competent in all domains to be a worthwhile person The idea is, when these assumptions are applied to everyday life, GAD may develop. Aaron Beck :Those with GAD hold unrealistic silent assumptions that imply imminent danger: Any strange situation is dangerous A situation/person is unsafe until proven safe
 Stimulus--->Appraisal---> Response. evaluation of stimulus based on memories, beliefs, and expectations. . Albert Ellis identified basic irrational assumptions: It is necessary for humans to be loved by everyone. It is catastrophic when things are not as one wants them to be. If something is dangerous, a person should be terribly concerned and dwell on the possibility that it will occur. One should be competent in all domains to be a worthwhile person. The idea is, when these assumptions are applied to everyday life, GAD may develop. Aaron Beck :Those with GAD hold unrealistic silent assumptions that imply imminent danger: Any strange situation is dangerous. A situation/person is unsafe until proven safe. Individuals misperceive and misinterpret internal and external stimuli. Selective attention and catastrophic thinking. Cognitive Appraisal (perceive threat) Stimulus--->Appraisal---> Response. evaluation of stimulus based on memories, beliefs, and expectations. . Albert Ellis identified basic irrational assumptions: It is necessary for humans to be loved by everyone. It is catastrophic when things are not as one wants them to be. If something is dangerous, a person should be terribly concerned and dwell on the possibility that it will occur. One should be competent in all domains to be a worthwhile person. The idea is, when these assumptions are applied to everyday life, GAD may develop. Aaron Beck :Those with GAD hold unrealistic silent assumptions that imply imminent danger: Any strange situation is dangerous. A situation/person is unsafe until proven safe.")
61
The Biological Approach to Anxiety
Genetic Component family and twin studies suggest a genetic component in most anxiety disorders panic disorder shows the strongest genetic component and generalized anxiety disorder the least. Neurotransmitter abnormalities - the release of catecholamine (NA, DA) is increased. - decrease level of GABA (GABA inhibit CNS irritability). - serotonin decrease causes anxiety; increased dopaminergic activity is associated with anxiety. Activity in the temporal cerebral cortex is increased. The locus ceruleus, a brain center of noradrengic neurons, is hyperactive in anxiety disorders, especially panic attacks. Elevated responsiveness in the amygdala, part of the fear circuit of the limbic system. HPA axis dysregulation Serotonin and basal ganglia abnormalities in OCD Hormonal theory of PTSD
 is increased. - decrease level of GABA (GABA inhibit CNS irritability). - serotonin decrease causes anxiety; increased dopaminergic activity is associated with anxiety. Activity in the temporal cerebral cortex is increased. The locus ceruleus, a brain center of noradrengic neurons, is hyperactive in anxiety disorders, especially panic attacks. Elevated responsiveness in the amygdala, part of the fear circuit of the limbic system. HPA axis dysregulation. Serotonin and basal ganglia abnormalities in OCD. Hormonal theory of PTSD.")
62
Other theories: Social factors Personality factors
Early life adversity Stressful events especially those involving threat Lack of support network Personality factors Some personality traits predispose to certain anxiety disorders – avoidant, perfectionist

63
Depression-Anxiety Comorbidity
The lifetime prevalence of depression is 60% in patients with social anxiety disorder Major Depressive Disorder 16.2% (lifetime prevalence) Anxiety Disorders 24.9% (lifetime prevalence) Up to 60% Overlap The lifetime prevalence of depression is 57% in patients with panic disorder Brown TA, et al. J Abnorm Psychol 2001;36: Kessler RC, et al. JAMA 2003;289: Kessler RC, et al. Arch Gen Psychiatry 1994;51:8-19.
 Anxiety Disorders 24.9% (lifetime prevalence) Up to 60% Overlap. The lifetime prevalence of depression is 57% in patients with panic disorder. Brown TA, et al. J Abnorm Psychol 2001;36: Kessler RC, et al. JAMA 2003;289: Kessler RC, et al. Arch Gen Psychiatry 1994;51:8-19.")
64
Depression and Anxiety Disorders Commonly Occur Together
SAD 37%* (SAD + MDD2) Fear/avoidance of social situations Blushing Trembling/shaking Palpitations Sweating Low self- esteem GAD MDD Difficulty concentrating GI complaints Interpersonal sensitivity 62%* (GAD + MDD1) Anhedonia Depressed mood Suicidal ideation Feelings of worthlessness Appetite disturbance Worry Anxiety Muscle tension Dry mouth Agitation Irritability Sleep disturbance Fatigue Pain *Lifetime prevalence of MDD among individuals with lifetime diagnoses of each anxiety disorder. 1. Wittchen HU, et al. Arch Gen Psychiatry. 1994;51: 2. Magee WJ, et al. Arch Gen Psychiatry. 1996;53: 3. DSM-IV-TR™. Washington, DC: American Psychiatric Association; 2000.
 Fear/avoidance. of social situations. Blushing. Trembling/shaking. Palpitations. Sweating. Low self- esteem. GAD. MDD. Difficulty concentrating. GI complaints Interpersonal sensitivity. 62%* (GAD + MDD1) Anhedonia. Depressed mood. Suicidal ideation. Feelings of worthlessness. Appetite disturbance. Worry. Anxiety. Muscle tension. Dry mouth. Agitation. Irritability. Sleep disturbance. Fatigue. Pain. *Lifetime prevalence of MDD among individuals with lifetime diagnoses of each anxiety disorder. 1. Wittchen HU, et al. Arch Gen Psychiatry. 1994;51: Magee WJ, et al. Arch Gen Psychiatry. 1996;53: DSM-IV-TR™. Washington, DC: American Psychiatric Association;")
65
Screening and Diagnosis Measurement-Based Care
GAD-7, LSAS, PTSD, YBOC Detect depression (PHQ-9, QIDS, CUDOS, Zung) Rule out bipolarity (MDQ, WHO CIDI 3.0) Diagnosis DSM-IV overview Comorbidity Suicide Assessment Symptom Tracking HAM-A (physician) CGI-A
 Rule out bipolarity (MDQ, WHO CIDI 3.0) Diagnosis. DSM-IV overview. Comorbidity. Suicide Assessment. Symptom Tracking. HAM-A (physician) CGI-A.")
66
Generalized Anxiety Disorder (GAD) GAD affects 6
Generalized Anxiety Disorder (GAD)
GAD affects 6.8 million adults, or 3.1% of the U.S. population.
Women are twice as likely to be affected as men.
Obsessive-Compulsive Disorder (OCD)
2.2 million, 1.0%
Equally common among men and women.
The median age of onset is 19, with 25 percent of cases occurring by age 14. One-third of affected adults first experienced symptoms in childhood. Hoarding is the compulsive purchasing, acquiring, searching, and saving of items that have little or no value. Panic Disorder
6 million, 2.7%
Women are twice as likely to be affected as men.
Very high comorbidity rate with major depression.
Posttraumatic Stress Disorder (PTSD)
7.7 million, 3.5%
Women are more likely to be affected than men.
Rape is the most likely trigger of PTSD: 65% of men and 45.9% of women who are raped will develop the disorder.
Childhood sexual abuse is a strong predictor of lifetime likelihood for developing PTSD.
Social Anxiety Disorder
15 million, 6.8%
Equally common among men and women, typically beginning around age 13.
According to a 2007 ADAA survey, 36% of people with social anxiety disorder report experiencing symptoms for 10 or more years before seeking help.
Specific Phobias
19 million, 8.7%
Women are twice as likely to be affected as men. Related Illnesses
Many people with an anxiety disorder also have a co-occurring disorder or physical illness, which can make their symptoms worse and recovery more difficult. It’s essential to be treated for both disorders. Generalized Anxiety Disorder (GAD)
GAD affects 6.8 million adults, or 3.1% of the U.S. population.
Women are twice as likely to be affected as men.
Obsessive-Compulsive Disorder (OCD)
2.2 million, 1.0%
Equally common among men and women.
The median age of onset is 19, with 25 percent of cases occurring by age 14. One-third of affected adults first experienced symptoms in childhood. Hoarding is the compulsive purchasing, acquiring, searching, and saving of items that have little or no value.
Posttraumatic Stress Disorder (PTSD)
7.7 million, 3.5%
Women are more likely to be affected than men.
Rape is the most likely trigger of PTSD: 65% of men and 45.9% of women who are raped will develop the disorder.
Childhood sexual abuse is a strong predictor of lifetime likelihood for developing PTSD.
Social Anxiety Disorder
15 million, 6.8%
Equally common among men and women, typically beginning around age 13.
According to a 2007 ADAA survey, 36% of people with social anxiety disorder report experiencing symptoms for 10 or more years before seeking help.
Specific Phobias
19 million, 8.7%
Women are twice as likely to be affected as men. Related Illnesses
Many people with an anxiety disorder also have a co-occurring disorder or physical illness, which can make their symptoms worse and recovery more difficult. It’s essential to be treated for both disorders.
 GAD affects 6.8 million adults, or 3.1% of the U.S. population. Women are twice as likely to be affected as men. Obsessive-Compulsive Disorder (OCD) 2.2 million, 1.0% Equally common among men and women. The median age of onset is 19, with 25 percent of cases occurring by age 14. One-third of affected adults first experienced symptoms in childhood. Hoarding is the compulsive purchasing, acquiring, searching, and saving of items that have little or no value. Panic Disorder 6 million, 2.7% Women are twice as likely to be affected as men. Very high comorbidity rate with major depression. Posttraumatic Stress Disorder (PTSD) 7.7 million, 3.5% Women are more likely to be affected than men. Rape is the most likely trigger of PTSD: 65% of men and 45.9% of women who are raped will develop the disorder. Childhood sexual abuse is a strong predictor of lifetime likelihood for developing PTSD. Social Anxiety Disorder 15 million, 6.8% Equally common among men and women, typically beginning around age 13. According to a 2007 ADAA survey, 36% of people with social anxiety disorder report experiencing symptoms for 10 or more years before seeking help. Specific Phobias 19 million, 8.7% Women are twice as likely to be affected as men. Related Illnesses Many people with an anxiety disorder also have a co-occurring disorder or physical illness, which can make their symptoms worse and recovery more difficult. It’s essential to be treated for both disorders. Generalized Anxiety Disorder (GAD) GAD affects 6.8 million adults, or 3.1% of the U.S. population. Women are twice as likely to be affected as men. Obsessive-Compulsive Disorder (OCD) 2.2 million, 1.0% Equally common among men and women. The median age of onset is 19, with 25 percent of cases occurring by age 14. One-third of affected adults first experienced symptoms in childhood. Hoarding is the compulsive purchasing, acquiring, searching, and saving of items that have little or no value. Posttraumatic Stress Disorder (PTSD) 7.7 million, 3.5% Women are more likely to be affected than men. Rape is the most likely trigger of PTSD: 65% of men and 45.9% of women who are raped will develop the disorder. Childhood sexual abuse is a strong predictor of lifetime likelihood for developing PTSD. Social Anxiety Disorder 15 million, 6.8% Equally common among men and women, typically beginning around age 13. According to a 2007 ADAA survey, 36% of people with social anxiety disorder report experiencing symptoms for 10 or more years before seeking help. Specific Phobias 19 million, 8.7% Women are twice as likely to be affected as men. Related Illnesses Many people with an anxiety disorder also have a co-occurring disorder or physical illness, which can make their symptoms worse and recovery more difficult. It’s essential to be treated for both disorders.")
67
generalized anxiety disorder (GAD)
")
68
Generalized Anxiety Disorder
Excessive uncontrollable worry about everyday things. This constant worry affects daily functioning and can cause physical symptoms. GAD can occur with other anxiety disorders, depressive disorders, or substance abuse. People with generalized anxiety disorder (GAD) go through the day filled with exaggerated worry and tension, even though there is little or nothing to provoke it. They anticipate disaster and are overly concerned about health issues, money, family problems, or difficulties at work. Sometimes just the thought of getting through the day produces anxiety. GAD is diagnosed when a person worries excessively about a variety of everyday problems for at least 6 months.13 People with GAD can’t seem to get rid of their concerns, even though they usually realize that their anxiety is more intense than the situation warrants. They can’t relax, startle easily, and have difficulty concentrating. Often they have trouble falling asleep or staying asleep. Physical symptoms that often accompany the anxiety include fatigue, headaches, muscle tension, muscle aches, difficulty swallowing, trembling, twitching, irritability, sweating, nausea, lightheadedness, having to go to the bathroom frequently, feeling out of breath, and hot flashes. When their anxiety level is mild, people with GAD can function socially and hold down a job. Although they don’t avoid certain situations as a result of their disorder, people with GAD can have difficulty carrying out the simplest daily activities if their anxiety is severe. GAD affects about 6.8 million American adults,1 including twice as many women as men.2 The disorder develops gradually and can begin at any point in the life cycle, although the years of highest risk are between childhood and middle age.2 There is evidence that genes play a modest role in GAD.13 Other anxiety disorders, depression, or substance abuse2,4 often accompany GAD, which rarely occurs alone. GAD is commonly treated with medication or cognitive-behavioral therapy, but co-occurring conditions must also be treated using the appropriate therapies.
 go through the day filled with exaggerated worry and tension, even though there is little or nothing to provoke it. They anticipate disaster and are overly concerned about health issues, money, family problems, or difficulties at work. Sometimes just the thought of getting through the day produces anxiety. GAD is diagnosed when a person worries excessively about a variety of everyday problems for at least 6 months.13 People with GAD can’t seem to get rid of their concerns, even though they usually realize that their anxiety is more intense than the situation warrants. They can’t relax, startle easily, and have difficulty concentrating. Often they have trouble falling asleep or staying asleep. Physical symptoms that often accompany the anxiety include fatigue, headaches, muscle tension, muscle aches, difficulty swallowing, trembling, twitching, irritability, sweating, nausea, lightheadedness, having to go to the bathroom frequently, feeling out of breath, and hot flashes. When their anxiety level is mild, people with GAD can function socially and hold down a job. Although they don’t avoid certain situations as a result of their disorder, people with GAD can have difficulty carrying out the simplest daily activities if their anxiety is severe. GAD affects about 6.8 million American adults,1 including twice as many women as men.2 The disorder develops gradually and can begin at any point in the life cycle, although the years of highest risk are between childhood and middle age.2 There is evidence that genes play a modest role in GAD.13. Other anxiety disorders, depression, or substance abuse2,4 often accompany GAD, which rarely occurs alone. GAD is commonly treated with medication or cognitive-behavioral therapy, but co-occurring conditions must also be treated using the appropriate therapies.")
69
Generalized Anxiety Disorder
The focus of GAD worry can shift, usually focusing on issues like job, finances, health of both self and family; but it can also include more mundane issues such as, chores, car repairs and being late for appointments. The intensity, duration and frequency of the worry are disproportionate to the issue

70
Generalized Anxiety Disorder
Characterized by at least 6 months of persistent and excessive anxiety and worry

71
Generalized Anxiety Disorder (GAD) GAD affects 6
Generalized Anxiety Disorder (GAD)
GAD affects 6.8 million adults, or 3.1% of the U.S. population.
Women are twice as likely to be affected as men.
 GAD affects 6.8 million adults, or 3.1% of the U.S. population. Women are twice as likely to be affected as men.")
72
GAD Epidemiology 5% prevalence in community samples
2:1 female/male ratio Age of onset is frequently in childhood or adolescence Chronic but fluctuating course of illness (worsened during stressful periods)
")
73
Generalized Anxiety Disorder (GAD)
Patients with GAD suffer from severe worry or anxiety that is out of proportion to situational factors. Must last most days for at least 6 months Described as “worriers” or “nervous”

74
GAD Symptoms include: Muscle tension Restlessness Insomnia
Difficulty concentrating Easy fatigability Irritability Persistent anxiety (rather than discrete panic attacks)
")
75
GAD Diagnostic Criteria
Excessive anxiety and worry that occurs more days than not for 6 months Difficult to control the worry 3 out of 6 symptoms Anxiety caused significant distress or impairment in function Not attributed to another organic cause

76
GAD Treatment Cognitive Behavioral Therapy Other Psychotherapies
Pharmacotherapy Antidepressants Benzodiazepines Buspirone

77
Common Causes There is no one cause for anxiety disorders. Several factors can play a role Genetics Brain biochemistry Overactive "fight or flight" response Can be caused by too much stress Life circumstances Personality People who have low self-esteem and poor coping skills may be more prone Certain drugs, both recreational and medicinal, can lead to symptoms of anxiety due to either side effects or withdrawal from the drug. In very rare cases, a tumor of the adrenal gland (pheochromocytoma) may be the cause of anxiety.
 may be the cause of anxiety.")
78
Symptoms of Anxiety Anxiety is an emotion often accompanied by
various physical symptoms, including: Twitching or trembling Muscle tension Headaches Sweating Dry mouth Difficulty swallowing Abdominal pain (may be the only symptom of stress especially in a child)
")
79
Additional Symptoms of Anxiety
Sometimes other symptoms accompany anxiety: Dizziness Rapid or irregular heart rate Rapid breathing Diarrhea or frequent need to urinate Fatigue Irritability, including loss of your temper Sleeping difficulties and nightmares Decreased concentration Sexual problems

80
Generalized anxiety disorder
Person is continually tense, apprehensive, and in a state of CNS arousal.

81
Generalized anxiety disorder
Tense and jittery Worried bad things will happen Muscular tension Agitation Sleeplessness

82
Generalized anxiety disorder
Person cannot identify the cause of the anxiety, and therefore can’t avoid or deal “Free floating anxiety”

83
Generalized anxiety disorder
Worry about things that are not too likely to happen Worry more intensely

84
Generalized Anxiety Disorder
Generalized anxiety disorder (GAD) is characterized by unrealistic or excessive worry (generalized free-floating persistent anxiety) about every day events/problems with symptoms of muscle and psychic tension, causing significant distress/functional impairment.
 is characterized by unrealistic or excessive worry (generalized free-floating persistent anxiety) about every day events/problems with symptoms of muscle and psychic tension, causing significant distress/functional impairment.")
85
What is Gen. Anxiety Disorder ?
Anxiety Disorders are characterized by persistent fear and anxiety that occurs too often, is too severe, is triggered too easily or lasts too long. Compared with others with anxiety disorders, persons with GAD have a better ability to maintain normal work and social relationships in spite of their distress. The “What if?” disorder

86
DSM-IV Diagnostic Criteria for Generalized Anxiety Disorder
A. Excessive anxiety or worry is present most days during at least a six-month period and involves a number of life events. B. The anxiety is difficult to control. C. At least three of the following: 1. Restlessness or feeling on edge. 2. Easy fatigability. 3. Difficulty concentrating. 4. Irritability. 5. Muscle tension. 6. Sleep disturbance. D. The focus of anxiety is not anticipatory anxiety about having a panic attack, as in panic disorder. E. The anxiety or physical symptoms cause significant distress or impairment in functioning. F. Symptoms are not caused by substance use or a medical condition, and symptoms are not related to a mood or psychotic disorder.

87
Diagnostic criteria of GAD- SUMMARY
Excessive Worry About Work Family and Children Health Finances Minor Matters Worry occurs most days (for at least 6 months) Difficult to control worry Associated with disturbed sleep, irritability, restlessness, poor concentration, fatigue, muscle tension
 Difficult to control worry. Associated with disturbed sleep, irritability, restlessness, poor concentration, fatigue, muscle tension.")
88
Clinical Features of Generalized Anxiety Disorder
A. Other features often include insomnia, irritability, trembling, muscle aches and soreness, muscle twitches, sweaty hands, dry mouth, and a heightened startle reflex. Patients may also report palpitations, dizziness, difficulty breathing, urinary frequency, dysphagia, light-headedness, abdominal pain, and diarrhea. B. Patients often complain that they “can't stop worrying,” which may revolve around valid concerns about money, jobs, marriage, health, and the safety of children. C. Chronic worry is a prominent feature of generalized anxiety disorder, unlike the intermittent terror that characterizes panic disorder.

89
D. Mood disorders, substance- and stress-related disorders (headaches, dyspepsia) commonly coexist with GAD. Up to one-fourth of GAD patients develop panic disorder. Excessive worry and somatic symptoms, including autonomic hyperactivity and hypervigilance, occur most days. E. About 30-50% of patients with anxiety disorders will also meet criteria for major depressive disorder. Drugs and alcohol may cause anxiety or may be an attempt at self-treatment. Substance abuse may be a complication of GAD.

90
Differential Diagnosis of Generalized Anxiety Disorder
Substance-Induced Anxiety Disorder: Substances such as caffeine, amphetamines, or cocaine can cause anxiety symptoms. Alcohol or benzodiazepine withdrawal can mimic symptoms of GAD. These disorders should be excluded by history and toxicology screen. B. Panic Disorder, Obsessive-Compulsive Disorder, Social Phobia, Hypochondriasis and Anorexia Nervosa 1. Many psychiatric disorders present with marked anxiety, and the diagnosis of GAD should be made only if the anxiety is unrelated to the other disorders. 2. For example, GAD should not be diagnosed in panic disorder if the patient has excessive anxiety about having a panic attack, or if an anorexic patient has anxiety about weight gain.

91
C. Anxiety Disorder Due to a General Medical Condition
C. Anxiety Disorder Due to a General Medical Condition. Hyperthyroidism, cardiac arrhythmias, pulmonary embolism, congestive heart failure, and hypoglycemia, may produce significant anxiety and should be ruled out as clinically indicated. D. Mood and Psychotic Disorders 1. Excessive worry and anxiety occurs in many mood and psychotic disorders. 2. If anxiety occurs only during the course of the mood or psychotic disorder, then GAD cannot be diagnosed.

92
Course and prognosis Course is chronic; symptoms may diminish as the patient get older. With time, secondary depression may develop. This is not uncommon if the condition is left untreated.

93
Treatment of Generalized Anxiety Disorder
The combination of pharmacologic therapy and psychotherapy is the most successful form of treatment.

94
I. Pharmacotherapy of Generalized Anxiety Disorder:
,Fluoxetine

95
Antidepressants 1. SSRIs and Venlafaxine
a. The onset of action of antidepressants is much slower than the benzodiazepines, but they have no addictive potential and may be more effective. An antidepressant is the agent of choice when depression coexists with anxiety. b. The side-effect profile for GAD patients is similar to that seen with depressive disorders. 2. Tricyclic antidepressants are also effective in treating GAD, but adverse effects limit their use.

96
Treatment Options Antidepressant Medications
Selective Serotonin Reuptake Inhibitors (SSRI) Serotonin and Norepinephrine Reuptake Inhibitors (SNRI) Norepinephrine-dopamine Reuptake Inhibitors Mixed Selective Serotonin Reuptake Inhibitors and Receptor Blockers Tricyclic Antidepressants (TCA) Monoamine Oxidase Inhibitors (MAOI) Nonpharmacological Therapy Psychotherapy Cognitive Behavioral Therapy (CBT) Interpersonal Therapy (IPT) Biofeedback? Exposure Response Treatment Trauma Focused CBT DBT 96
 Serotonin and Norepinephrine Reuptake Inhibitors (SNRI) Norepinephrine-dopamine Reuptake Inhibitors. Mixed Selective Serotonin Reuptake Inhibitors and Receptor Blockers. Tricyclic Antidepressants (TCA) Monoamine Oxidase Inhibitors (MAOI) Nonpharmacological Therapy. Psychotherapy. Cognitive Behavioral Therapy (CBT) Interpersonal Therapy (IPT) Biofeedback Exposure Response Treatment. Trauma Focused CBT. DBT. 96.")
97
Alternative Treatments
Acupuncture Aromatherapy Breathing Exercises Exercise Meditation Nutrition and Diet Therapy Vitamins Self Love

98
Factors to Consider in Choosing an Medications for Anxiety
Patient preference Nature of prior response to medication Relative efficacy and effectiveness Safety, tolerability, and anticipated side effects Co-occurring psychiatric or general medical conditions Potential drug interactions Half-life Cost

99
B. Buspirone a. Buspirone is an effective treatment for GAD. It lacks sedative effects. Tolerance to the beneficial effects of buspirone does not seem to develop. There is no physiologic dependence or withdrawal syndrome.

100
C. Benzodiazepines 1. Benzodiazepines can almost always relieve anxiety if given in adequate doses, and they have no delayed onset of action. 2. Benzodiazepines have few side effects other than sedation. Tolerance to their sedative effects develops but not to their antianxiety properties. 3. Drug dependency becomes a clinical issue if the benzodiazepine is used regularly for more than 2-3 weeks. A withdrawal syndrome occurs in 70% of patients, characterized by intense anxiety, tremulousness, dysphoria, sleep and perceptual disturbances and appetite suppression. 4. Slow tapering of benzodiazepines is crucial (especially those with short half-lives).
.")
101
Comparison of Benzodiazepines
BZN Sedation Anxiolytic Half life Lipid solu Dose Diazepam +++ + 20-80 h High 5 mg od Alprazolam 6-20 h Low 0.5 mg qid Clonazapam ++ 22-50 h 0.5 mg bid Lorazepam 10-20 h Med 1 mg tid Chlordiazepx 7-30 h 15 mg bid

102
II. Non-Drug Approaches to Anxiety
1. Patients should stop drinking coffee and other caffeinated beverages, and avoid excessive alcohol consumption. 2. Patients should get adequate sleep, with the use of medication if necessary. Moderate exercise each day may help reduce the intensity of anxiety symptoms. 3. Psychotherapy a. Cognitive behavioral therapy, with emphasis on relaxation techniques and instruction on misinterpretation of physiologic symptoms, may improve functioning in mild cases. b. Supportive or insight oriented psychotherapy can be helpful in mild cases of anxiety.

103
GOOD SLEEP HYGENE ECPSLLC.COM
No sleeping during the day (If you have to no longer than 30 mins) Don’t lay in bed if not sleepy Get out of bed if unable to sleep No milk during the evening No caffeine No Nicotine No Alcohol Warm baths, no showers No exercising before going to bed but exercise in the morning Sleep at the same time every night Wake up at the same time every morning Make sure bed and pillow is comfortable, primarily for sleep with appropriate room temp (Cool about 60 degrees), noise free (some sleep better with white noise). Remember Cool, dark and quiet) Jot down all of your concerns and worries Avoid “Over the counter” sleep aides Don’t over sleep Set your body clock (wake up to light) Develop a bedtime routine No TV in bed ECPSLLC.COM
 Don’t lay in bed if not sleepy Get out of bed if unable to sleep. No milk during the evening. No caffeine. No Nicotine. No Alcohol. Warm baths, no showers. No exercising before going to bed but exercise in the morning. Sleep at the same time every night. Wake up at the same time every morning. Make sure bed and pillow is comfortable, primarily for sleep with appropriate room temp (Cool about 60 degrees), noise free (some sleep better with white noise). Remember Cool, dark and quiet) Jot down all of your concerns and worries. Avoid Over the counter sleep aides. Don’t over sleep. Set your body clock (wake up to light) Develop a bedtime routine. No TV in bed. ECPSLLC.COM.")
104
Other Psychological managements:
Education about nature of disorder Progressive muscle relaxation Structured problem solving Graded exposure to difficult situations Support (guidance, advice, development of coping strategies) Counselling Stress management (relaxation, meditation, exercise regimens that improve stress recovery)
 Counselling. Stress management (relaxation, meditation, exercise regimens that improve stress recovery)")
105
Combination Maximize benefit by affecting multiple neurotransmitters
Could increase adherence and lower drop-out rates Could target side effects of first agent (eg, insomnia, fatigue, sexual dysfunction) Papakostas G. J Clin Psychiatry. 2009;70(S6):16-25.
 Papakostas G. J Clin Psychiatry. 2009;70(S6):")
106
(SOCIAL PHOBIA)
")
107
social anxiety disorder

108
Social Anxiety Disorder 15 million, 6
Social Anxiety Disorder
15 million, 6.8%
Equally common among men and women, typically beginning around age 13.
(According to a 2007 ADAA survey, 36% of people with social anxiety disorder report experiencing symptoms for 10 or more years before seeking help. Comorbity exisits Social phobia, also called social anxiety disorder, is diagnosed when people become overwhelmingly anxious and excessively self-conscious in everyday social situations. People with social phobia have an intense, persistent, and chronic fear of being watched and judged by others and of doing things that will embarrass them. They can worry for days or weeks before a dreaded situation. This fear may become so severe that it interferes with work, school, and other ordinary activities, and can make it hard to make and keep friends. While many people with social phobia realize that their fears about being with people are excessive or unreasonable, they are unable to overcome them. Even if they manage to confront their fears and be around others, they are usually very anxious beforehand, are intensely uncomfortable throughout the encounter, and worry about how they were judged for hours afterward. Social phobia can be limited to one situation (such as talking to people, eating or drinking, or writing on a blackboard in front of others) or may be so broad (such as in generalized social phobia) that the person experiences anxiety around almost anyone other than the family. Physical symptoms that often accompany social phobia include blushing, profuse sweating, trembling, nausea, and difficulty talking. When these symptoms occur, people with social phobia feel as though all eyes are focused on them. Social phobia affects about 15 million American adults.1 Women and men are equally likely to develop the disorder,10 which usually begins in childhood or early adolescence.2 There is some evidence that genetic factors are involved.11 Social phobia is often accompanied by other anxiety disorders or depression,2,4and substance abuse may develop if people try to self-medicate their anxiety.4,5 Social phobia can be successfully treated with certain kinds of psychotherapy or medications.
 or may be so broad (such as in generalized social phobia) that the person experiences anxiety around almost anyone other than the family. Physical symptoms that often accompany social phobia include blushing, profuse sweating, trembling, nausea, and difficulty talking. When these symptoms occur, people with social phobia feel as though all eyes are focused on them. Social phobia affects about 15 million American adults.1 Women and men are equally likely to develop the disorder,10 which usually begins in childhood or early adolescence.2 There is some evidence that genetic factors are involved.11 Social phobia is often accompanied by other anxiety disorders or depression,2,4and substance abuse may develop if people try to self-medicate their anxiety.4,5. Social phobia can be successfully treated with certain kinds of psychotherapy or medications.")
109
Facts AFFECTS ABOUT 15 MILLION AMERICANS
BEGINS IN CHILDHOOD AND EARLY ADOLESCENCE EVIDENCE THAT GENETICS ARE INVOLVED COMORBIDITY OFTEN EXSISTS Social phobia affects about 15 million American adults. Women and men are equally likely to develop the disorder Usually begins in childhood or early adolescence. There is some evidence that genetic factors are involved. Social phobia is often accompanied by other anxiety disorders or depression, and substance abuse may develop if people try to self-medicate their anxiety.

110
Social Phobia General characteristics
Fear of being in social situations in which one will be embarrassed or humiliated Social phobia, also called social anxiety disorder, is diagnosed when people become overwhelmingly anxious and excessively self-conscious in everyday social situations. People with social phobia have an intense, persistent, and chronic fear of being watched and judged by others and of doing things that will embarrass them. They can worry for days or weeks before a dreaded situation. This fear may become so severe that it interferes with work, school, and other ordinary activities, and can make it hard to make and keep friends. While many people with social phobia realize that their fears about being with people are excessive or unreasonable, they are unable to overcome them. Even if they manage to confront their fears and be around others, they are usually very anxious beforehand, are intensely uncomfortable throughout the encounter, and worry about how they were judged for hours afterward. Social phobia can be limited to one situation (such as talking to people, eating or drinking, or writing on a blackboard in front of others) or may be so broad (such as in generalized social phobia) that the person experiences anxiety around almost anyone other than the family. Physical symptoms that often accompany social phobia include blushing, profuse sweating, trembling, nausea, and difficulty talking. When these symptoms occur, people with social phobia feel as though all eyes are focused on them. Social phobia affects about 15 million American adults.1 Women and men are equally likely to develop the disorder,10 which usually begins in childhood or early adolescence.2 There is some evidence that genetic factors are involved.11 Social phobia is often accompanied by other anxiety disorders or depression,2,4and substance abuse may develop if people try to self-medicate their anxiety.4,5 Social phobia can be successfully treated with certain kinds of psychotherapy or medications.
 or may be so broad (such as in generalized social phobia) that the person experiences anxiety around almost anyone other than the family. Physical symptoms that often accompany social phobia include blushing, profuse sweating, trembling, nausea, and difficulty talking. When these symptoms occur, people with social phobia feel as though all eyes are focused on them. Social phobia affects about 15 million American adults.1 Women and men are equally likely to develop the disorder,10 which usually begins in childhood or early adolescence.2 There is some evidence that genetic factors are involved.11 Social phobia is often accompanied by other anxiety disorders or depression,2,4and substance abuse may develop if people try to self-medicate their anxiety.4,5. Social phobia can be successfully treated with certain kinds of psychotherapy or medications.")
111
Social Phobia Interaction of psychosocial and biological causal factors Social phobias as learned behavior Social fears and phobias in an evolutionary context Preparedness and social phobia

112
Social Phobia Interaction of psychosocial and biological causal factors Genetic and temperamental factors Perceptions of uncontrollability Cognitive variables

113
Social phobias Shyness to the extreme
Persistent, irrational fear linked to presence of others Fear of being scrutinized or negatively evaluated by others

114
Social phobias Person with social phobia may avoid Speaking Eating out
Going to parties Anything in the presence of others

115
CONCERN Very Under diagnosed and Therefore undertreated.
Can cause severe impairment in social, occupational and academic functioning Can Lead to Avoidant Behavior

116
DIAGNOSIS Fear or avoidance of social or performance situations
Situations avoided, or endured with anxiety or distress Patients recognize symptoms as excessive or unreasonable Very distressing or disabling Key Point The core feature of SAD is fear/anxiety associated with social or performance situations Background DSM-IV diagnostic criteria for SAD include Fear and/or avoidance of social situations Feared situations are avoided, or endured with intense anxiety or distress The fear is recognized as excessive or unreasonable The fear or avoidance interferes with work, social, and daily activities Reference DSM-IV-TR™. Washington, DC: American Psychiatric Association; 2000. .

117
Feared/Avoided Situations
Public speaking/performing Eating, drinking, writing, working while being observed by others Social events Dating Meeting new people Being center of attention Using public bathroom

118
Common Somatic Complaints
Stuttering Blushing Palpitations Sweating Trembling Shaking

119
Spectrum of Social Discomfort
Transient Low interference Low avoidance Chronic High interference High avoidance Shyness Key Point The symptoms of social phobia lie on a continuum Background Some researchers feel that SAD represents the severe end of a continuum of shyness, as shown on the slide. Although the relationship between shyness and SAD has not been extensively researched, there are a number of similarities between the 2 constructs Both are characterized by the manifestation of symptoms of physiologic arousal and fears of negative evaluation in response to various social situations Differentiation may be a matter of severity Shyness tends to be transitory and associated with little impairment or avoidance, while SAD is chronic and is often associated with substantial impairment and avoidance At the far end of the continuum is avoidant personality disorder, which may be conceptualized as chronic, severe generalized SAD Reference Lang AJ, Stein MB. J Clin Psychiatry. 2001;62(suppl 1):5-10. Nongeneralized SAD Generalized SAD Avoidant personality disorder
:5-10. Nongeneralized SAD. Generalized SAD. Avoidant. personality disorder.")
120
Treatment Goals Eliminate anxiety/phobic avoidance
Eliminate functional disability Treat associated comorbidities Choose therapy that is tolerable for the long term

121
Social Phobia: Treatment
Antidepressants, SSRI’s and MAOI’s High potency benzodiazepines Low doses of beta blockers are helpful for public speaking (if only an occasional event); this alleviates the autonomic symptoms Psychotherapy-cognitive restructuring
; this alleviates the autonomic symptoms. Psychotherapy-cognitive restructuring.")
122
Treatment Medication Management Psychotherapy
Combined Medication Management and Psychotherapy Practice Practice Practice!

123
Social Effects of Anxiety
Depression Not as involved with family and friends the way you used to be Lowered quality of relationships Low energy Lack of motivation to do the things you once looked forward to doing Unable to convey the person that you are Fear and avoidance of situations where previous attacks occurred

125
Social Phobia/Anxiety
Social anxiety disorder, also known as social phobia, is an intense fear of social situations. This fear arises when the individual believes that they may be judged, scrutinized or humiliated by others. Individuals with the disorder are acutely aware of the physical signs of their anxiety and fear that others will notice, judge them, and think poorly of them. In extreme cases this intense uneasiness can progress into a full blown panic attack.

126
Social Phobia/Anxiety
Common anxiety provoking social situations include: public speaking talking with people in authority dating and developing close relationships making a phone call or answering the phone interviewing attending and participating in class speaking with strangers meeting new people eating, drinking, or writing in public using public bathrooms driving shopping

127
Specific Disorder Facts
Generalized Anxiety Disorder Women are twice as likely to be afflicted than men. Very likely to exist along with other disorders. Obsessive Compulsive Disorder It is equally common among men and women. One third of afflicted adults had their first symptoms in childhood. Panic Disorder Occurs with major depression in very high rates. 2003 Anxiety Disorders Association of America

128
Obsessive-Compulsive Disorder
People with obsessive-compulsive disorder (OCD) have persistent, upsetting thoughts (obsessions) and use rituals (compulsions) to control the anxiety these thoughts produce. Most of the time, the rituals end up controlling them. For example, if people are obsessed with germs or dirt, they may develop a compulsion to wash their hands over and over again. If they develop an obsession with intruders, they may lock and relock their doors many times before going to bed. Being afraid of social embarrassment may prompt people with OCD to comb their hair compulsively in front of a mirror-sometimes they get “caught” in the mirror and can’t move away from it. Performing such rituals is not pleasurable. At best, it produces temporary relief from the anxiety created by obsessive thoughts. Other common rituals are a need to repeatedly check things, touch things (especially in a particular sequence), or count things. Some common obsessions include having frequent thoughts of violence and harming loved ones, persistently thinking about performing sexual acts the person dislikes, or having thoughts that are prohibited by religious beliefs. People with OCD may also be preoccupied with order and symmetry, have difficulty throwing things out (so they accumulate), or hoard unneeded items. Healthy people also have rituals, such as checking to see if the stove is off several times before leaving the house. The difference is that people with OCD perform their rituals even though doing so interferes with daily life and they find the repetition distressing. Although most adults with OCD recognize that what they are doing is senseless, some adults and most children may not realize that their behavior is out of the ordinary. OCD affects about 2.2 million American adults,1 and the problem can be accompanied by eating disorders,6 other anxiety disorders, or depression.2,4 It strikes men and women in roughly equal numbers and usually appears in childhood, adolescence, or early adulthood.2 One-third of adults with OCD develop symptoms as children, and research indicates that OCD might run in families.3 The course of the disease is quite varied. Symptoms may come and go, ease over time, or get worse. If OCD becomes severe, it can keep a person from working or carrying out normal responsibilities at home. People with OCD may try to help themselves by avoiding situations that trigger their obsessions, or they may use alcohol or drugs to calm themselves.4,5 OCD usually responds well to treatment with certain medications and/or exposure-based psychotherapy, in which people face situations that cause fear or anxiety and become less sensitive (desensitized) to them. NIMH is supporting research into new treatment approaches for people whose OCD does not respond well to the usual therapies. These approaches include combination and augmentation (add-on) treatments, as well as modern techniques such as deep brain stimulation.
 have persistent, upsetting thoughts (obsessions) and use rituals (compulsions) to control the anxiety these thoughts produce. Most of the time, the rituals end up controlling them. For example, if people are obsessed with germs or dirt, they may develop a compulsion to wash their hands over and over again. If they develop an obsession with intruders, they may lock and relock their doors many times before going to bed. Being afraid of social embarrassment may prompt people with OCD to comb their hair compulsively in front of a mirror-sometimes they get caught in the mirror and can’t move away from it. Performing such rituals is not pleasurable. At best, it produces temporary relief from the anxiety created by obsessive thoughts. Other common rituals are a need to repeatedly check things, touch things (especially in a particular sequence), or count things. Some common obsessions include having frequent thoughts of violence and harming loved ones, persistently thinking about performing sexual acts the person dislikes, or having thoughts that are prohibited by religious beliefs. People with OCD may also be preoccupied with order and symmetry, have difficulty throwing things out (so they accumulate), or hoard unneeded items. Healthy people also have rituals, such as checking to see if the stove is off several times before leaving the house. The difference is that people with OCD perform their rituals even though doing so interferes with daily life and they find the repetition distressing. Although most adults with OCD recognize that what they are doing is senseless, some adults and most children may not realize that their behavior is out of the ordinary. OCD affects about 2.2 million American adults,1 and the problem can be accompanied by eating disorders,6 other anxiety disorders, or depression.2,4 It strikes men and women in roughly equal numbers and usually appears in childhood, adolescence, or early adulthood.2 One-third of adults with OCD develop symptoms as children, and research indicates that OCD might run in families.3. The course of the disease is quite varied. Symptoms may come and go, ease over time, or get worse. If OCD becomes severe, it can keep a person from working or carrying out normal responsibilities at home. People with OCD may try to help themselves by avoiding situations that trigger their obsessions, or they may use alcohol or drugs to calm themselves.4,5. OCD usually responds well to treatment with certain medications and/or exposure-based psychotherapy, in which people face situations that cause fear or anxiety and become less sensitive (desensitized) to them. NIMH is supporting research into new treatment approaches for people whose OCD does not respond well to the usual therapies. These approaches include combination and augmentation (add-on) treatments, as well as modern techniques such as deep brain stimulation.")
129
Obsessive-Compulsive Disorder (OCD) 2. 2 million, 1
Obsessive-Compulsive Disorder (OCD)
2.2 million, 1.0%
Equally common among men and women.
The median age of onset is 19, with 25 percent of cases occurring by age 14. One-third of affected adults first experienced symptoms in childhood. Hoarding is the compulsive purchasing, acquiring, searching, and saving of items that have little or no value.
 2.2 million, 1.0% Equally common among men and women. The median age of onset is 19, with 25 percent of cases occurring by age 14. One-third of affected adults first experienced symptoms in childhood. Hoarding is the compulsive purchasing, acquiring, searching, and saving of items that have little or no value.")
130
Obsessive-Compulsive Disorder
Characterized by uncontrollable obsessions and compulsions which the sufferer usually recognizes as being excessive or unreasonable. Obsessions are recurring thoughts or impulses that are intrusive or inappropriate and cause the sufferer anxiety: Thoughts about contamination, for example, when an individual fears coming into contact with dirt, germs or "unclean" objects; Persistent doubts, for example, whether or not one has turned off the iron or stove, locked the door or turned on the answering machine; Extreme need for orderliness; Aggressive impulses or thoughts, for example, being overcome with the urge to yell 'fire' in a crowded theater

131
Obsessive-Compulsive Disorder
Compulsions are repetitive behaviors or rituals performed by the OCD sufferer, performance of these rituals neutralize the anxiety caused by obsessive thoughts, relief is only temporary. Cleaning. Repeatedly washing their hands, showering, or constantly cleaning their home; Checking. Individuals may check several or even hundreds of times to make sure that stoves are turned off and doors are locked; Repeating. Some repeat a name, phrase or action over and over; Slowness. Some individuals may take an excessively slow and methodical approach to daily activities, they may spend hours organizing and arranging objects; Hoarding. Hoarders are unable to throw away useless items, such as old newspapers, junk mail, even broken appliances In order for OCD to be diagnosed, the obsessions and/or compulsions must take up a considerable amount of the sufferers time, at least one hour every day, and interfere with normal routines .

132
Obsessive-Compulsive Disorder
Obsessions- repetitive unwanted ideas that the person recognizes are irrational Compulsions- repetitive, often ritualized behavior whose behavior serves to diminish anxiety caused by obsessions

133
Obsessive-Compulsive Disorder
Prevalence and age of onset Characteristics of OCD Types of compulsions Comorbidity with other disorders

134
Common Examples of OCD Common Obsessions: Common Compulsions:
Contamination fears of germs, dirt, etc. Washing Imagining having harmed self or others Repeating Imagining losing control of aggressive urges Checking Intrusive sexual thoughts or urges Touching Excessive religious or moral doubt Counting Forbidden thoughts Ordering/arranging A need to have things "just so" Hoarding or saving A need to tell, ask, confess Praying

135
OCD is not OCPD Obsessive-Compulsive Disorder is different from obsessive compulsive personality disorder (OCPD) OCPD: a pervasive pattern of preoccupation with orderliness, perfectionism and control that begins by early adulthood

136
Obsessive-Compulsive Disorder: Psychosocial Causal Factors
Psychoanalytic viewpoint Behavioral viewpoint The role of memory Attempting to suppress obsessive thoughts

137
Obsessive-Compulsive Disorder: Biological Causal Factors
Genetic influences Abnormalities in brain function The role of serotonin

138
OCD Treatment Serotonin reuptake inhibitors
Clomipramine, a serotonergic tricyclic antidepressant Psychotherapy: exposure and response prevention

139
Panic Disorder Panic disorder is a real illness that can be successfully treated. It is characterized by sudden attacks of terror, usually accompanied by a pounding heart, sweatiness, weakness, faintness, or dizziness. During these attacks, people with panic disorder may flush or feel chilled; their hands may tingle or feel numb; and they may experience nausea, chest pain, or smothering sensations. Panic attacks usually produce a sense of unreality, a fear of impending doom, or a fear of losing control. A fear of one’s own unexplained physical symptoms is also a symptom of panic disorder. People having panic attacks sometimes believe they are having heart attacks, losing their minds, or on the verge of death. They can’t predict when or where an attack will occur, and between episodes many worry intensely and dread the next attack. Panic attacks can occur at any time, even during sleep. An attack usually peaks within 10 minutes, but some symptoms may last much longer. Panic disorder affects about 6 million American adults1 and is twice as common in women as men.2 Panic attacks often begin in late adolescence or early adulthood,2 but not everyone who experiences panic attacks will develop panic disorder. Many people have just one attack and never have another. The tendency to develop panic attacks appears to be inherited.3 People who have full-blown, repeated panic attacks can become very disabled by their condition and should seek treatment before they start to avoid places or situations where panic attacks have occurred. For example, if a panic attack happened in an elevator, someone with panic disorder may develop a fear of elevators that could affect the choice of a job or an apartment, and restrict where that person can seek medical attention or enjoy entertainment. Some people’s lives become so restricted that they avoid normal activities, such as grocery shopping or driving. About one-third become housebound or are able to confront a feared situation only when accompanied by a spouse or other trusted person. 2 When the condition progresses this far, it is called agoraphobia, or fear of open spaces. Early treatment can often prevent agoraphobia, but people with panic disorder may sometimes go from doctor to doctor for years and visit the emergency room repeatedly before someone correctly diagnoses their condition. This is unfortunate, because panic disorder is one of the most treatable of all the anxiety disorders, responding in most cases to certain kinds of medication or certain kinds of cognitive psychotherapy, which help change thinking patterns that lead to fear and anxiety. Panic disorder is often accompanied by other serious problems, such as depression, drug abuse, or alcoholism.4,5 These conditions need to be treated separately. Symptoms of depression include feelings of sadness or hopelessness, changes in appetite or sleep patterns, low energy, and difficulty concentrating. Most people with depression can be effectively treated with antidepressant medications, certain types of psychotherapy, or a combination of the two.

140
Panic Disorder 6 million, 2
Panic Disorder
6 million, 2.7%
Women are twice as likely to be affected as men.
Very high comorbidity rate with major depression.
Panic Disorder
6 million, 2.7%
Women are twice as likely to be affected as men.
Very high comorbidity rate with major depression.

141
Epidemiology of Panic Disorder
Panic disorder has a lifetime prevalence of % 2:1 female/male ratio ? Of true gender difference versus men tend to self-medicate with alcohol and are less likely to seek treatment. Onset is late teens through third decade of life.

142
Panic Disorder With and Without Agoraphobia
Panic versus anxiety Agoraphobia Agoraphobia without panic

143
Panic Disorder Prevalence and age of onset
Comorbidity with other disorders Biological causal factors The role of Norepinephrine and Serotonin

144
Panic Attack Discrete episodes of intense anxiety Sudden onset
Peak within 10 minutes Associated with at least 4 of the 13 other somatic or cognitive symptoms of autonomic arousal

145
Panic Attack Symptoms Cardiac: palpitations, tachycardia, chest pain or discomfort Pulmonary: shortness of breath, a feeling of choking GI: nausea or abdominal distress Neurological: trembling and shaking, dizziness, lightheadedness or faintness, paresthesias

146
Panic Attack Symptoms Autonomic Arousal: sweating, chills or hot flashes Psychological: Derealization (feeling of unreality) Depersonalization (feeling detached from oneself) Fear of losing control or going crazy Fear of dying
 Fear of losing control or going crazy. Fear of dying.")
147
Panic Disorder A syndrome characterized by recurrent unexpected panic attacks (at least 4 in one month) Attacks are followed for at least one month with: Concern about having another attack Worry about implications of the attack Behavior changes because of the attacks

148
Agoraphobia Complication of panic disorder Means “ fear of the market”
Anxiety or avoidance of places or situations from which escape might be difficult, embarrassing, or help may be unavailable. Restricts daily activities

149
Agoraphobia Agoraphobia
The patient may avoid crowds, restaurants, highways, bridges, movie theaters etc. In its most severe form, the patient may become dependent on companions to face situations outside the home. Some individuals become homebound.

150
Differential Diagnosis of Panic Disorder
Not due to another anxiety disorder Not due to effects of a general medical condition Cardiovascular disease Pulmonary disease Neurological disease Endocrine disease Drug intoxication or withdrawal Other (lupus, infections, heavy metal poisoning, uremia, temporal arteritis)
")
151
Panic Disorder: Costs 200,000 normal coronary angiograms/yr in the U.S. at a cost of 600 million dollars: 1/3 of these patients have panic disorder ½ of patients referred for non-invasive testing for atypical chest pain and who have normal tests have panic disorder 1/3 patients undergoing work-up for vestibular disorder with c/o dizziness have panic disorder

152
Panic Disorder: Comorbidity
Panic disorder patients have an increased personal and family history of other anxiety, mood and substance abuse disorders. Major depression is a co-morbid diagnosis in 1/3 of cases presenting for treatment Untreated patients have high risk of suicide

153
Panic Disorder: Treatment
About 80% of patients will respond to treatment Antidepressant medications are effective Serotonin reuptake inhibitors (SSRI) are first line therapy Tricyclic antidepressants (TCA) and monoamine oxidase inhibitors (MAOI’s) are also used.
 are first line therapy. Tricyclic antidepressants (TCA) and monoamine oxidase inhibitors (MAOI’s) are also used.")
154
Panic Disorder: Treatment
Sedative-Hypnotics: benzodiazepines are ideally used in the short term before an antidepressant has had time to work Cognitive Behavioral Therapy (CBT): helps patients overcome a learned pattern of catastrophically misinterpreting the physical symptoms associated with panic attacks.
: helps patients overcome a learned pattern of catastrophically misinterpreting the physical symptoms associated with panic attacks.")
155
Panic Disorder The abrupt onset of an episode of intense fear or discomfort, which peaks in approximately 10 minutes, and includes at least four of the following symptoms: A feeling of imminent danger or doom The need to escape Palpitations Sweating Trembling Shortness of breath or a smothering feeling A feeling of choking Chest pain or discomfort Nausea or abdominal discomfort Dizziness or lightheadedness A sense of things being unreal, depersonalization A fear of losing control or "going crazy" A fear of dying Tingling sensations Chills or hot flushes

156
Panic Disorder There are three types of Panic Attacks:
1. Unexpected - the attack "comes out of the blue" without warning and for no discernable reason. 2. Situational - situations in which an individual always has an attack, for example, upon entering a tunnel. 3. Situationally Predisposed - situations in which an individual is likely to have a Panic Attack, but does not always have one. An example of this would be an individual who sometimes has attacks while driving.

157
Panic and the Brain

158
Panic Disorder Genetic factors Cognitive and behavioral causal factors
Interoceptive fears

159
Panic Disorder: The Cognitive Theory of Panic

160
Panic Disorder: The Cognitive Theory of Panic
Perceived control and safety Anxiety sensitivity as a vulnerability factor for panic Safety behaviors and the persistence of panic Cognitive biases and the maintenance of panic

161
Treating Panic Disorder and Agoraphobia
Medications Behavioral and cognitive-behavioral treatments

162
Post-traumatic stress disorder (PTSD)
Post-traumatic stress disorder (PTSD) develops after a terrifying ordeal that involved physical harm or the threat of physical harm. The person who develops PTSD may have been the one who was harmed, the harm may have happened to a loved one, or the person may have witnessed a harmful event that happened to loved ones or strangers. PTSD was first brought to public attention in relation to war veterans, but it can result from a variety of traumatic incidents, such as mugging, rape, torture, being kidnapped or held captive, child abuse, car accidents, train wrecks, plane crashes, bombings, or natural disasters such as floods or earthquakes. People with PTSD may startle easily, become emotionally numb (especially in relation to people with whom they used to be close), lose interest in things they used to enjoy, have trouble feeling affectionate, be irritable, become more aggressive, or even become violent. They avoid situations that remind them of the original incident, and anniversaries of the incident are often very difficult. PTSD symptoms seem to be worse if the event that triggered them was deliberately initiated by another person, as in a mugging or a kidnapping. Most people with PTSD repeatedly relive the trauma in their thoughts during the day and in nightmares when they sleep. These are called flashbacks. Flashbacks may consist of images, sounds, smells, or feelings, and are often triggered by ordinary occurrences, such as a door slamming or a car backfiring on the street. A person having a flashback may lose touch with reality and believe that the traumatic incident is happening all over again. Not every traumatized person develops full-blown or even minor PTSD. Symptoms usually begin within 3 months of the incident but occasionally emerge years afterward. They must last more than a month to be considered PTSD. The course of the illness varies. Some people recover within 6 months, while others have symptoms that last much longer. In some people, the condition becomes chronic. PTSD affects about 7.7 million American adults,1but it can occur at any age, including childhood.7 Women are more likely to develop PTSD than men,8 and there is some evidence that susceptibility to the disorder may run in families.9 PTSD is often accompanied by depression, substance abuse, or one or more of the other anxiety disorders.4 Certain kinds of medication and certain kinds of psychotherapy usually treat the symptoms of PTSD very effectively.
 develops after a terrifying ordeal that involved physical harm or the threat of physical harm. The person who develops PTSD may have been the one who was harmed, the harm may have happened to a loved one, or the person may have witnessed a harmful event that happened to loved ones or strangers. PTSD was first brought to public attention in relation to war veterans, but it can result from a variety of traumatic incidents, such as mugging, rape, torture, being kidnapped or held captive, child abuse, car accidents, train wrecks, plane crashes, bombings, or natural disasters such as floods or earthquakes. People with PTSD may startle easily, become emotionally numb (especially in relation to people with whom they used to be close), lose interest in things they used to enjoy, have trouble feeling affectionate, be irritable, become more aggressive, or even become violent. They avoid situations that remind them of the original incident, and anniversaries of the incident are often very difficult. PTSD symptoms seem to be worse if the event that triggered them was deliberately initiated by another person, as in a mugging or a kidnapping. Most people with PTSD repeatedly relive the trauma in their thoughts during the day and in nightmares when they sleep. These are called flashbacks. Flashbacks may consist of images, sounds, smells, or feelings, and are often triggered by ordinary occurrences, such as a door slamming or a car backfiring on the street. A person having a flashback may lose touch with reality and believe that the traumatic incident is happening all over again. Not every traumatized person develops full-blown or even minor PTSD. Symptoms usually begin within 3 months of the incident but occasionally emerge years afterward. They must last more than a month to be considered PTSD. The course of the illness varies. Some people recover within 6 months, while others have symptoms that last much longer. In some people, the condition becomes chronic. PTSD affects about 7.7 million American adults,1but it can occur at any age, including childhood.7 Women are more likely to develop PTSD than men,8 and there is some evidence that susceptibility to the disorder may run in families.9 PTSD is often accompanied by depression, substance abuse, or one or more of the other anxiety disorders.4. Certain kinds of medication and certain kinds of psychotherapy usually treat the symptoms of PTSD very effectively.")
163
Women are more likely to be afflicted than men.
Posttraumatic Stress Disorder (PTSD)
7.7 million, 3.5%
Women are more likely to be affected than men.
Rape is the most likely trigger of PTSD: 65% of men and 45.9% of women who are raped will develop the disorder.
Childhood sexual abuse is a strong predictor of lifetime likelihood for developing PTSD.
Women are more likely to be afflicted than men. Rape is the most likely trigger of PTSD, 65% of men and 45.9% of women who are raped will develop the disorder. Childhood sexual abuse is a strong predictor of lifetime likelihood for developing PTSD.
 7.7 million, 3.5% Women are more likely to be affected than men. Rape is the most likely trigger of PTSD: 65% of men and 45.9% of women who are raped will develop the disorder. Childhood sexual abuse is a strong predictor of lifetime likelihood for developing PTSD. Women are more likely to be afflicted than men. Rape is the most likely trigger of PTSD, 65% of men and 45.9% of women who are raped will develop the disorder. Childhood sexual abuse is a strong predictor of lifetime likelihood for developing PTSD.")
164
Post Traumatic Stress Disorder (PTSD)
Patients with PTSD have experienced a trauma and develop disabling symptoms in response to the event. Symptoms usually begin within 3 months of the trauma Syndrome can occur at any age

165
Definition of Trauma The person experienced, witnessed or learned of an event that involved actual or threatened death, serious injury, or threat of harm to self or others The person’s response involved intense fear, helplessness or horror

166
Diagnosis of PTSD Symptoms must be > one month duration and include: Re-experiencing symptoms Avoidance symptoms Emotional numbing Hyperarousal symptoms

167
Re-experiencing Symptoms
There are recurrent, intrusive thoughts of the event (can’t not think about it) Dreams (nightmares) about the event Acting or feeling the event is recurring, or sense of living the event (flashbacks) Psychological or Physiological Distress upon exposure to reminders or cues of the event.
 Dreams (nightmares) about the event. Acting or feeling the event is recurring, or sense of living the event (flashbacks) Psychological or Physiological Distress upon exposure to reminders or cues of the event.")
168
Avoidance/Numbing Symptoms
Avoid thoughts, feelings, places or people that arouse memories of the event Being unable to recall important parts of the event Decrease interest in activities Feeling detached or estranged from others Decreased range of affect Sense of foreshortened future

169
Hyperarousal Symptoms
Patient experiences at least two of the following: Insomnia (falling or staying asleep) Irritability or outbursts of anger Decreased concentration Hypervigilance Increased/exaggerated startle response
 Irritability or outbursts of anger. Decreased concentration. Hypervigilance. Increased/exaggerated startle response.")
170
Post-Traumatic Stress Disorder
Critical Component Symptoms occurs AFTER a traumatic stressor

171
Types of Traumas Natural Human induces earthquakes floods fires war
crimes of violence

172
Types of Trauma Being diagnosed with a life threatening illness
Sudden unexpected death of family/friend Witnessing violence (including domestic violence) Learning one’s child has life threatening illness Sexual abuse Rape Physical abuse Severe motor vehicle accidents Robbery/mugging Terrorist attack Combat veteran Natural disasters
 Learning one’s child has life threatening illness. Sexual abuse. Rape. Physical abuse. Severe motor vehicle accidents. Robbery/mugging. Terrorist attack. Combat veteran. Natural disasters.")
173
Co-Morbid Diagnoses Alcoholism Depression Generalized Anxiety
75% for Vietnam Veterans with PTSD Depression 77% of firefighters with PTSD also have depression Generalized Anxiety Panic Attacks

174
Symptoms Categories Intrusive distressing recollections dreams
flashbacks psychological trigger reactions physiological trigger reactions

175
Symptoms Categories Avoidance avoid thoughts, feelings or discussions
avoid activities, places memory blocks anhedonia (without pleasure) numb alexithymia (emotions unknown) feeling of doom
 numb. alexithymia (emotions unknown) feeling of doom.")
176
Symptom Categories Hyperarousal Symptoms sleep disturbance
anger problems concentration startle response “on guard” hypervigilence

177
Diagnoses Acute Stress Disorder PTSD new to DSM-IV (1994)
symptoms 2 days to 4 weeks following traumatic event PTSD new to DSM-III (1980) symptoms beyond 4 weeks delayed onset
 symptoms beyond 4 weeks. delayed onset.")
178
Post-Traumatic Stress Disorder
Exposure to traumas such as a serious accident, a natural disaster, or criminal assault can result in PTSD. When the aftermath of a traumatic experience interferes with normal functioning, the person may be suffering from PTSD. Symptoms of PTSD are: Reexperiencing the event, which can take the form of intrusive thoughts and recollections, or recurrent dreams; Avoidance behavior in which the sufferer avoids activities, situations, people,and/or conversations which he/she associates with the trauma; A general numbness and loss of interest in surroundings; Hypersensitivity, including: inability to sleep, anxious feelings, overactive startle response, hypervigilance, irritability and outbursts of anger.

179
Specific Disorder Facts
Posttraumatic Stress Disorder

180
Who Is Vulnerable? All ages Both genders
Across Cultures and ethnic groups

181
PTSD Treatment Psychotherapies
Exposure-based cognitive behavioral therapy Psychotherapy aimed at survivor anger, guilt and helplessness (victimization) Pharmacological treatment targets the reduction of prominent symptoms SSRI’s are first line therapy Atypical antipsychotics are being increasingly used
 Pharmacological treatment targets the reduction of prominent symptoms. SSRI’s are first line therapy. Atypical antipsychotics are being increasingly used.")
182
Specific Phobia A specific phobia is an intense, irrational fear of something that poses little or no actual danger. Some of the more common specific phobias are centered around closed-in places, heights, escalators, tunnels, highway driving, water, flying, dogs, and injuries involving blood. Such phobias aren’t just extreme fear; they are irrational fear of a particular thing. You may be able to ski the world’s tallest mountains with ease but be unable to go above the 5th floor of an office building. While adults with phobias realize that these fears are irrational, they often find that facing, or even thinking about facing, the feared object or situation brings on a panic attack or severe anxiety. Specific phobias affect an estimated 19.2 million adult Americans1 and are twice as common in women as men.10 They usually appear in childhood or adolescence and tend to persist into adulthood.12 The causes of specific phobias are not well understood, but there is some evidence that the tendency to develop them may run in families.11 If the feared situation or feared object is easy to avoid, people with specific phobias may not seek help; but if avoidance interferes with their careers or their personal lives, it can become disabling and treatment is usually pursued. Specific phobias respond very well to carefully targeted psychotherapy.

183
Specific Phobias 19 million, 8
Specific Phobias
19 million, 8.7%
Women are twice as likely to be affected as men. Related Illnesses
Many people with an anxiety disorder also have a co-occurring disorder or physical illness, which can make their symptoms worse and recovery more difficult. It’s essential to be treated for both disorders.

184
Epidemiology of Specific Phobias
Lifetime prevalence is 10% of the population Age of onset varies with subtype Childhood onset for phobias of animals, natural environments blood and injections Bimodal distribution (childhood and mid-twenties for situational phobias

185
Phobic Disorders Phobias Specific phobias Social phobia Agoraphobia

186
Specific Phobias

187
Specific Phobias Psychosocial causal factors
Genetic and temperamental causal factors Preparedness and the nonrandom distribution of fears and phobias Treating specific phobias

188
Specific Phobia Marked and persistent fear that is excessive and unreasonable of a specific object or situation Exposure to the phobic stimulus will provoke an anxiety response

189
Phobia Subtypes Animals or insects
Natural environment– storms, water, heights Blood, injury, injection, medical procedure Situational flying, driving, enclosed places Having a phobia of a specific subtype increased the chances of having another phobia within that subtype

190
Specific Phobia Treatments
Flooding-exposing the person to the feared stimulus Exposure therapy works to desensitize the patient using a series of gradual, self-paced exposures to the phobic stimulus; uses relaxation, hypnosis, breathing control and other cognitive approaches Benzodiazepines or Beta blockers are useful acutely

191
Specific Phobia: Treatment
Example: Fear of Flying Visualize a plane. Look at a plane in the sky. Drive by an airport. Go to a museum that has planes. Same museum—visualize going inside. Go inside. Go to airport and watch planes take off and land. Visualize yourself on a plane flying. Omnimax theater experience. The real thing.

192
Generalized anxiety disorder (GAD) is a pattern of frequent, constant worry and anxiety over many different activities and events. Causes Anyone can develop this disorder, even kids. Most people with the disorder report that they have been anxious for as long as they can remember. GAD occurs somewhat more often in women than in men. Generalized anxiety disorder (GAD) is a common condition. Genes may play a role. Stress may also contribute to the development of GAD. Symptoms The main symptom is the almost constant presence of worry or tension, even when there is little or no cause. Worries seem to float from one problem to another, such as family or relationship problems, work issues, money, health, and other problems. Other symptoms include: Even when aware that their worries or fears are stronger than needed, a person with GAD still has difficulty controlling them. Difficulty concentrating Fatigue Irritability Restlessness, and often becoming startled very easily Problems falling or staying asleep, and sleep that is often restless and unsatisfying Along with the worries and anxieties, a number of physical symptoms may also be present, including muscle tension (shakiness, headaches) and stomach problems, such as nausea or diarrhea. Exams and Tests The health care provider will perform a physical and mental health exam. Tests will be done to rule out other conditions and behaviors that cause similar symptoms. The goal of treatment is to help you function well during day-to-day life. A combination of medicine and cognitive-behavioral therapy (CBT) works best. Treatment Medications are an important part of treatment. Once you start them, do not suddenly stop without talking with your health care provider. Medications that may be used include: Selective serotonin reuptake inhibitors (SSRIs) are usually the first choice in medications. Serotonin-norepinephrine reuptake inhibitors (SNRIs) are another choice. Other antidepressants and some antiseizure drugs may be used for severe cases. Benzodiazepines such as alprazolam (Xanax), clonazepam (Klonopin), and lorazepam (Ativan) may be used if antidepressants don't help enough with symptoms. Long-term dependence on these drugs is a concern. A medication called buspirone may also be used. Cognitive-behavioral therapy helps you understand your behaviors and how to gain control of them. You will have 10 to 20 visits over a number of weeks. During therapy you will learn how to: Understand and gain control of your distorted views of life stressors, such as other people's behavior or life events. Manage stress and relax when symptoms occur. Recognize and replace panic-causing thoughts, decreasing the sense of helplessness. Avoid thinking that minor worries will develop into very bad problems. Avoiding caffeine, illicit drugs, and even some cold medicines may also help reduce symptoms. A healthy lifestyle that includes exercise, enough rest, and good nutrition can help reduce the impact of anxiety. A support group allows you to talk to people who share common experiences and problems. This may help ease the stress related to a medical condition. Support Groups Support groups are not a substitute for effective treatment, but can be a helpful addition to it. Outlook (Prognosis) How well a person does depends on the severity of the condition. GAD may continue and be difficult to treat. However, most patients get better with a combination of medication and behavioral therapy. Depression and substance abuse may occur with an anxiety disorder. Possible Complications When to Contact a Medical Professional Call your health care provider if you constantly worry and feel anxious and it interferes with your daily activities. Alternative Names GAD; Anxiety disorder
 is a common condition. Genes may play a role. Stress may also contribute to the development of GAD. Symptoms. The main symptom is the almost constant presence of worry or tension, even when there is little or no cause. Worries seem to float from one problem to another, such as family or relationship problems, work issues, money, health, and other problems. Other symptoms include: Even when aware that their worries or fears are stronger than needed, a person with GAD still has difficulty controlling them. Difficulty concentrating. Fatigue. Irritability. Restlessness, and often becoming startled very easily. Problems falling or staying asleep, and sleep that is often restless and unsatisfying. Along with the worries and anxieties, a number of physical symptoms may also be present, including muscle tension (shakiness, headaches) and stomach problems, such as nausea or diarrhea. Exams and Tests. The health care provider will perform a physical and mental health exam. Tests will be done to rule out other conditions and behaviors that cause similar symptoms. The goal of treatment is to help you function well during day-to-day life. A combination of medicine and cognitive-behavioral therapy (CBT) works best. Treatment. Medications are an important part of treatment. Once you start them, do not suddenly stop without talking with your health care provider. Medications that may be used include: Selective serotonin reuptake inhibitors (SSRIs) are usually the first choice in medications. Serotonin-norepinephrine reuptake inhibitors (SNRIs) are another choice. Other antidepressants and some antiseizure drugs may be used for severe cases. Benzodiazepines such as alprazolam (Xanax), clonazepam (Klonopin), and lorazepam (Ativan) may be used if antidepressants don t help enough with symptoms. Long-term dependence on these drugs is a concern. A medication called buspirone may also be used. Cognitive-behavioral therapy helps you understand your behaviors and how to gain control of them. You will have 10 to 20 visits over a number of weeks. During therapy you will learn how to: Understand and gain control of your distorted views of life stressors, such as other people s behavior or life events. Manage stress and relax when symptoms occur. Recognize and replace panic-causing thoughts, decreasing the sense of helplessness. Avoid thinking that minor worries will develop into very bad problems. Avoiding caffeine, illicit drugs, and even some cold medicines may also help reduce symptoms. A healthy lifestyle that includes exercise, enough rest, and good nutrition can help reduce the impact of anxiety. A support group allows you to talk to people who share common experiences and problems. This may help ease the stress related to a medical condition. Support Groups. Support groups are not a substitute for effective treatment, but can be a helpful addition to it. Outlook (Prognosis) How well a person does depends on the severity of the condition. GAD may continue and be difficult to treat. However, most patients get better with a combination of medication and behavioral therapy. Depression and substance abuse may occur with an anxiety disorder. Possible Complications. When to Contact a Medical Professional. Call your health care provider if you constantly worry and feel anxious and it interferes with your daily activities. Alternative Names. GAD; Anxiety disorder.")
193
Treatment of Anxiety Disorders
Medications Specific types of psychotherapy Comorbidities History In general, anxiety disorders are treated with medication, specific types of psychotherapy, or both.14 Treatment choices depend on the problem and the person’s preference. Before treatment begins, a doctor must conduct a careful diagnostic evaluation to determine whether a person’s symptoms are caused by an anxiety disorder or a physical problem. If an anxiety disorder is diagnosed, the type of disorder or the combination of disorders that are present must be identified, as well as any coexisting conditions, such as depression or substance abuse. Sometimes alcoholism, depression, or other coexisting conditions have such a strong effect on the individual that treating the anxiety disorder must wait until the coexisting conditions are brought under control. Treatment of Anxiety Disorders People with anxiety disorders who have already received treatment should tell their current doctor about that treatment in detail. If they received medication, they should tell their doctor what medication was used, what the dosage was at the beginning of treatment, whether the dosage was increased or decreased while they were under treatment, what side effects occurred, and whether the treatment helped them become less anxious. If they received psychotherapy, they should describe the type of therapy, how often they attended sessions, and whether the therapy was useful. Often people believe that they have “failed” at treatment or that the treatment didn’t work for them when, in fact, it was not given for an adequate length of time or was administered incorrectly. Sometimes people must try several different treatments or combinations of treatment before they find the one that works for them. Medication will not cure anxiety disorders, but it can keep them under control while the person receives psychotherapy. Medication must be prescribed by physicians, usually psychiatrists, who can either offer psychotherapy themselves or work as a team with psychologists, social workers, or counselors who provide psychotherapy. The principal medications used for anxiety disorders are antidepressants, anti-anxiety drugs, and beta-blockers to control some of the physical symptoms. With proper treatment, many people with anxiety disorders can lead normal, fulfilling lives. Medication Antidepressants Antidepressants were developed to treat depression but are also effective for anxiety disorders. Although these medications begin to alter brain chemistry after the very first dose, their full effect requires a series of changes to occur; it is usually about 4 to 6 weeks before symptoms start to fade. It is important to continue taking these medications long enough to let them work. Fluoxetine (Prozac®), sertraline (Zoloft®), escitalopram (Lexapro®), paroxetine (Paxil®), and citalopram (Celexa®) are some of the SSRIs commonly prescribed for panic disorder, OCD, PTSD, and social phobia. SSRIs are also used to treat panic disorder when it occurs in combination with OCD, social phobia, or depression. Venlafaxine (Effexor®), a drug closely related to the SSRIs, is used to treat GAD. These medications are started at low doses and gradually increased until they have a beneficial effect. Some of the newest antidepressants are called selective serotonin reuptake inhibitors, or SSRIs. SSRIs alter the levels of the neurotransmitter serotonin in the brain, which, like other neurotransmitters, helps brain cells communicate with one another. SSRIs SSRIs have fewer side effects than older antidepressants, but they sometimes produce slight nausea or jitters when people first start to take them. These symptoms fade with time. Some people also experience sexual dysfunction with SSRIs, which may be helped by adjusting the dosage or switching to another SSRI. Tricyclics are older than SSRIs and work as well as SSRIs for anxiety disorders other than OCD. They are also started at low doses that are gradually increased. They sometimes cause dizziness, drowsiness, dry mouth, and weight gain, which can usually be corrected by changing the dosage or switching to another tricyclic medication. Tricyclics MAOIs Tricyclics include imipramine (Tofranil®), which is prescribed for panic disorder and GAD, and clomipramine (Anafranil®), which is the only tricyclic antidepressant useful for treating OCD. Monoamine oxidase inhibitors (MAOIs) are the oldest class of antidepressant medications. The MAOIs most commonly prescribed for anxiety disorders are phenelzine (Nardil®), followed by tranylcypromine (Parnate®), and isocarboxazid (Marplan®), which are useful in treating panic disorder and social phobia. People who take MAOIs cannot eat a variety of foods and beverages (including cheese and red wine) that contain tyramine or take certain medications, including some types of birth control pills, pain relievers (such as Advil®, Motrin®, or Tylenol®), cold and allergy medications, and herbal supplements; these substances can interact with MAOIs to cause dangerous increases in blood pressure. The development of a new MAOI skin patch may help lessen these risks. MAOIs can also react with SSRIs to produce a serious condition called “serotonin syndrome,” which can cause confusion, hallucinations, increased sweating, muscle stiffness, seizures, changes in blood pressure or heart rhythm, and other potentially life-threatening conditions. High-potency benzodiazepines combat anxiety and have few side effects other than drowsiness. Because people can get used to them and may need higher and higher doses to get the same effect, benzodiazepines are generally prescribed for short periods of time, especially for people who have abused drugs or alcohol and who become dependent on medication easily. One exception to this rule is people with panic disorder, who can take benzodiazepines for up to a year without harm. Anti-Anxiety Drugs Some people experience withdrawal symptoms if they stop taking benzodiazepines abruptly instead of tapering off, and anxiety can return once the medication is stopped. These potential problems have led some physicians to shy away from using these drugs or to use them in inadequate doses. Clonazepam (Klonopin®) is used for social phobia and GAD, lorazepam (Ativan®) is helpful for panic disorder, and alprazolam (Xanax®) is useful for both panic disorder and GAD. Buspirone (Buspar®), an azapirone, is a newer anti-anxiety medication used to treat GAD. Possible side effects include dizziness, headaches, and nausea. Unlike benzodiazepines, buspirone must be taken consistently for at least 2 weeks to achieve an anti-anxiety effect. Beta-blockers, such as propranolol (Inderal®), which is used to treat heart conditions, can prevent the physical symptoms that accompany certain anxiety disorders, particularly social phobia. When a feared situation can be predicted (such as giving a speech), a doctor may prescribe a beta-blocker to keep physical symptoms of anxiety under control. Beta-Blockers Before taking medication for an anxiety disorder: Taking Medications Ask your doctor when and how the medication should be stopped. Some drugs can’t be stopped abruptly but must be tapered off slowly under a doctor’s supervision. Tell your doctor about any alternative therapies or over-the-counter medications you are using. Ask your doctor to tell you about the effects and side effects of the drug. Psychotherapy Be aware that some medications are effective only if they are taken regularly and that symptoms may recur if the medication is stopped. Work with your doctor to determine which medication is right for you and what dosage is best. Cognitive-Behavioral Therapy Psychotherapy involves talking with a trained mental health professional, such as a psychiatrist, psychologist, social worker, or counselor, to discover what caused an anxiety disorder and how to deal with its symptoms. Cognitive-behavioral therapy (CBT) is very useful in treating anxiety disorders. The cognitive part helps people change the thinking patterns that support their fears, and the behavioral part helps people change the way they react to anxiety-provoking situations. For example, CBT can help people with panic disorder learn that their panic attacks are not really heart attacks and help people with social phobia learn how to overcome the belief that others are always watching and judging them. When people are ready to confront their fears, they are shown how to use exposure techniques to desensitize themselves to situations that trigger their anxieties. People with OCD who fear dirt and germs are encouraged to get their hands dirty and wait increasing amounts of time before washing them. The therapist helps the person cope with the anxiety that waiting produces; after the exercise has been repeated a number of times, the anxiety diminishes. People with social phobia may be encouraged to spend time in feared social situations without giving in to the temptation to flee and to make small social blunders and observe how people respond to them. Since the response is usually far less harsh than the person fears, these anxieties are lessened. People with PTSD may be supported through recalling their traumatic event in a safe situation, which helps reduce the fear it produces. CBT therapists also teach deep breathing and other types of exercises to relieve anxiety and encourage relaxation. Exposure-based behavioral therapy has been used for many years to treat specific phobias. The person gradually encounters the object or situation that is feared, perhaps at first only through pictures or tapes, then later face-to-face. Often the therapist will accompany the person to a feared situation to provide support and guidance. CBT is undertaken when people decide they are ready for it and with their permission and cooperation. To be effective, the therapy must be directed at the person’s specific anxieties and must be tailored to his or her needs. There are no side effects other than the discomfort of temporarily increased anxiety. CBT or behavioral therapy often lasts about 12 weeks. It may be conducted individually or with a group of people who have similar problems. Group therapy is particularly effective for social phobia. Often “homework” is assigned for participants to complete between sessions. There is some evidence that the benefits of CBT last longer than those of medication for people with panic disorder, and the same may be true for OCD, PTSD, and social phobia. If a disorder recurs at a later date, the same therapy can be used to treat it successfully a second time. Medication can be combined with psychotherapy for specific anxiety disorders, and this is the best treatment approach for many people.
, sertraline (Zoloft®), escitalopram (Lexapro®), paroxetine (Paxil®), and citalopram (Celexa®) are some of the SSRIs commonly prescribed for panic disorder, OCD, PTSD, and social phobia. SSRIs are also used to treat panic disorder when it occurs in combination with OCD, social phobia, or depression. Venlafaxine (Effexor®), a drug closely related to the SSRIs, is used to treat GAD. These medications are started at low doses and gradually increased until they have a beneficial effect. Some of the newest antidepressants are called selective serotonin reuptake inhibitors, or SSRIs. SSRIs alter the levels of the neurotransmitter serotonin in the brain, which, like other neurotransmitters, helps brain cells communicate with one another. SSRIs. SSRIs have fewer side effects than older antidepressants, but they sometimes produce slight nausea or jitters when people first start to take them. These symptoms fade with time. Some people also experience sexual dysfunction with SSRIs, which may be helped by adjusting the dosage or switching to another SSRI. Tricyclics are older than SSRIs and work as well as SSRIs for anxiety disorders other than OCD. They are also started at low doses that are gradually increased. They sometimes cause dizziness, drowsiness, dry mouth, and weight gain, which can usually be corrected by changing the dosage or switching to another tricyclic medication. Tricyclics. MAOIs. Tricyclics include imipramine (Tofranil®), which is prescribed for panic disorder and GAD, and clomipramine (Anafranil®), which is the only tricyclic antidepressant useful for treating OCD. Monoamine oxidase inhibitors (MAOIs) are the oldest class of antidepressant medications. The MAOIs most commonly prescribed for anxiety disorders are phenelzine (Nardil®), followed by tranylcypromine (Parnate®), and isocarboxazid (Marplan®), which are useful in treating panic disorder and social phobia. People who take MAOIs cannot eat a variety of foods and beverages (including cheese and red wine) that contain tyramine or take certain medications, including some types of birth control pills, pain relievers (such as Advil®, Motrin®, or Tylenol®), cold and allergy medications, and herbal supplements; these substances can interact with MAOIs to cause dangerous increases in blood pressure. The development of a new MAOI skin patch may help lessen these risks. MAOIs can also react with SSRIs to produce a serious condition called serotonin syndrome, which can cause confusion, hallucinations, increased sweating, muscle stiffness, seizures, changes in blood pressure or heart rhythm, and other potentially life-threatening conditions. High-potency benzodiazepines combat anxiety and have few side effects other than drowsiness. Because people can get used to them and may need higher and higher doses to get the same effect, benzodiazepines are generally prescribed for short periods of time, especially for people who have abused drugs or alcohol and who become dependent on medication easily. One exception to this rule is people with panic disorder, who can take benzodiazepines for up to a year without harm. Anti-Anxiety Drugs. Some people experience withdrawal symptoms if they stop taking benzodiazepines abruptly instead of tapering off, and anxiety can return once the medication is stopped. These potential problems have led some physicians to shy away from using these drugs or to use them in inadequate doses. Clonazepam (Klonopin®) is used for social phobia and GAD, lorazepam (Ativan®) is helpful for panic disorder, and alprazolam (Xanax®) is useful for both panic disorder and GAD. Buspirone (Buspar®), an azapirone, is a newer anti-anxiety medication used to treat GAD. Possible side effects include dizziness, headaches, and nausea. Unlike benzodiazepines, buspirone must be taken consistently for at least 2 weeks to achieve an anti-anxiety effect. Beta-blockers, such as propranolol (Inderal®), which is used to treat heart conditions, can prevent the physical symptoms that accompany certain anxiety disorders, particularly social phobia. When a feared situation can be predicted (such as giving a speech), a doctor may prescribe a beta-blocker to keep physical symptoms of anxiety under control. Beta-Blockers. Before taking medication for an anxiety disorder: Taking Medications. Ask your doctor when and how the medication should be stopped. Some drugs can’t be stopped abruptly but must be tapered off slowly under a doctor’s supervision. Tell your doctor about any alternative therapies or over-the-counter medications you are using. Ask your doctor to tell you about the effects and side effects of the drug. Psychotherapy. Be aware that some medications are effective only if they are taken regularly and that symptoms may recur if the medication is stopped. Work with your doctor to determine which medication is right for you and what dosage is best. Cognitive-Behavioral Therapy. Psychotherapy involves talking with a trained mental health professional, such as a psychiatrist, psychologist, social worker, or counselor, to discover what caused an anxiety disorder and how to deal with its symptoms. Cognitive-behavioral therapy (CBT) is very useful in treating anxiety disorders. The cognitive part helps people change the thinking patterns that support their fears, and the behavioral part helps people change the way they react to anxiety-provoking situations. For example, CBT can help people with panic disorder learn that their panic attacks are not really heart attacks and help people with social phobia learn how to overcome the belief that others are always watching and judging them. When people are ready to confront their fears, they are shown how to use exposure techniques to desensitize themselves to situations that trigger their anxieties. People with OCD who fear dirt and germs are encouraged to get their hands dirty and wait increasing amounts of time before washing them. The therapist helps the person cope with the anxiety that waiting produces; after the exercise has been repeated a number of times, the anxiety diminishes. People with social phobia may be encouraged to spend time in feared social situations without giving in to the temptation to flee and to make small social blunders and observe how people respond to them. Since the response is usually far less harsh than the person fears, these anxieties are lessened. People with PTSD may be supported through recalling their traumatic event in a safe situation, which helps reduce the fear it produces. CBT therapists also teach deep breathing and other types of exercises to relieve anxiety and encourage relaxation. Exposure-based behavioral therapy has been used for many years to treat specific phobias. The person gradually encounters the object or situation that is feared, perhaps at first only through pictures or tapes, then later face-to-face. Often the therapist will accompany the person to a feared situation to provide support and guidance. CBT is undertaken when people decide they are ready for it and with their permission and cooperation. To be effective, the therapy must be directed at the person’s specific anxieties and must be tailored to his or her needs. There are no side effects other than the discomfort of temporarily increased anxiety. CBT or behavioral therapy often lasts about 12 weeks. It may be conducted individually or with a group of people who have similar problems. Group therapy is particularly effective for social phobia. Often homework is assigned for participants to complete between sessions. There is some evidence that the benefits of CBT last longer than those of medication for people with panic disorder, and the same may be true for OCD, PTSD, and social phobia. If a disorder recurs at a later date, the same therapy can be used to treat it successfully a second time. Medication can be combined with psychotherapy for specific anxiety disorders, and this is the best treatment approach for many people.")
194
How to Get Help for Anxiety Disorders
See our MD See A Clincian Support Groups CBT Cut Caffiene, Alcohol, Drugs, Cold Medicaations Internet Family Support Systems How to Get Help for Anxiety Disorders If you think you have an anxiety disorder, the first person you should see is your family doctor. A physician can determine whether the symptoms that alarm you are due to an anxiety disorder, another medical condition, or both. If an anxiety disorder is diagnosed, the next step is usually seeing a mental health professional. The practitioners who are most helpful with anxiety disorders are those who have training in cognitive-behavioral therapy and/or behavioral therapy, and who are open to using medication if it is needed. You should feel comfortable talking with the mental health professional you choose. If you do not, you should seek help elsewhere. Once you find a mental health professional with whom you are comfortable, the two of you should work as a team and make a plan to treat your anxiety disorder together. Remember that once you start on medication, it is important not to stop taking it abruptly. Certain drugs must be tapered off under the supervision of a doctor or bad reactions can occur. Make sure you talk to the doctor who prescribed your medication before you stop taking it. If you are having trouble with side effects, it’s possible that they can be eliminated by adjusting how much medication you take and when you take it. Most insurance plans, including health maintenance organizations (HMOs), will cover treatment for anxiety disorders. Check with your insurance company and find out. If you don’t have insurance, the Health and Human Services division of your county government may offer mental health care at a public mental health center that charges people according to how much they are able to pay. If you are on public assistance, you may be able to get care through your state Medicaid plan. Ways to Make Treatment More Effective Many people with anxiety disorders benefit from joining a self-help or support group and sharing their problems and achievements with others. Internet chat rooms can also be useful in this regard, but any advice received over the Internet should be used with caution, as Internet acquaintances have usually never seen each other and false identities are common. Talking with a trusted friend or member of the clergy can also provide support, but it is not a substitute for care from a mental health professional. Stress management techniques and meditation can help people with anxiety disorders calm themselves and may enhance the effects of therapy. There is preliminary evidence that aerobic exercise may have a calming effect. Since caffeine, certain illicit drugs, and even some over-the-counter cold medications can aggravate the symptoms of anxiety disorders, they should be avoided. Check with your physician or pharmacist before taking any additional medications. The family is very important in the recovery of a person with an anxiety disorder. Ideally, the family should be supportive but not help perpetuate their loved one’s symptoms. Family members should not trivialize the disorder or demand improvement without treatment. If your family is doing either of these things, you may want to show them this booklet so they can become educated allies and help you succeed in therapy.
, will cover treatment for anxiety disorders. Check with your insurance company and find out. If you don’t have insurance, the Health and Human Services division of your county government may offer mental health care at a public mental health center that charges people according to how much they are able to pay. If you are on public assistance, you may be able to get care through your state Medicaid plan. Ways to Make Treatment More Effective. Many people with anxiety disorders benefit from joining a self-help or support group and sharing their problems and achievements with others. Internet chat rooms can also be useful in this regard, but any advice received over the Internet should be used with caution, as Internet acquaintances have usually never seen each other and false identities are common. Talking with a trusted friend or member of the clergy can also provide support, but it is not a substitute for care from a mental health professional. Stress management techniques and meditation can help people with anxiety disorders calm themselves and may enhance the effects of therapy. There is preliminary evidence that aerobic exercise may have a calming effect. Since caffeine, certain illicit drugs, and even some over-the-counter cold medications can aggravate the symptoms of anxiety disorders, they should be avoided. Check with your physician or pharmacist before taking any additional medications. The family is very important in the recovery of a person with an anxiety disorder. Ideally, the family should be supportive but not help perpetuate their loved one’s symptoms. Family members should not trivialize the disorder or demand improvement without treatment. If your family is doing either of these things, you may want to show them this booklet so they can become educated allies and help you succeed in therapy.")
195
Physical and psychological stress Diet Brain imaging technology
Role of Research in Improving the Understanding and Treatment of Anxiety Disorders Role of Genes Enviormental factors Physical and psychological stress Diet Brain imaging technology Neurochemical techniques – Amygdala and Hippocampus Developing Medications and behavioral therapies NIMH supports research into the causes, diagnosis, prevention, and treatment of anxiety disorders and other mental illnesses. Scientists are looking at what role genes play in the development of these disorders and are also investigating the effects of environmental factors such as pollution, physical and psychological stress, and diet. In addition, studies are being conducted on the “natural history” (what course the illness takes without treatment) of a variety of individual anxiety disorders, combinations of anxiety disorders, and anxiety disorders that are accompanied by other mental illnesses such as depression. Scientists currently think that, like heart disease and type 1 diabetes, mental illnesses are complex and probably result from a combination of genetic, environmental, psychological, and developmental factors. For instance, although NIMH-sponsored studies of twins and families suggest that genetics play a role in the development of some anxiety disorders, problems such as PTSD are triggered by trauma. Genetic studies may help explain why some people exposed to trauma develop PTSD and others do not. Several parts of the brain are key actors in the production of fear and anxiety. 15 Using brain imaging technology and neurochemical techniques, scientists have discovered that the amygdala and the hippocampus play significant roles in most anxiety disorders. The amygdala is an almond-shaped structure deep in the brain that is believed to be a communications hub between the parts of the brain that process incoming sensory signals and the parts that interpret these signals. It can alert the rest of the brain that a threat is present and trigger a fear or anxiety response. It appears that emotional memories are stored in the central part of the amygdala and may play a role in anxiety disorders involving very distinct fears, such as fears of dogs, spiders, or flying. The hippocampus is the part of the brain that encodes threatening events into memories. Studies have shown that the hippocampus appears to be smaller in some people who were victims of child abuse or who served in military combat.16, 17 Research will determine what causes this reduction in size and what role it plays in the flashbacks, deficits in explicit memory, and fragmented memories of the traumatic event that are common in PTSD. By learning more about how the brain creates fear and anxiety, scientists may be able to devise better treatments for anxiety disorders. For example, if specific neurotransmitters are found to play an important role in fear, drugs may be developed that will block them and decrease fear responses; if enough is learned about how the brain generates new cells throughout the lifecycle, it may be possible to stimulate the growth of new neurons in the hippocampus in people with PTSD.18 Current research at NIMH on anxiety disorders includes studies that address how well medication and behavioral therapies work in the treatment of OCD, and the safety and effectiveness of medications for children and adolescents who have a combination of anxiety disorders and attention deficit hyperactivity disorder.
 of a variety of individual anxiety disorders, combinations of anxiety disorders, and anxiety disorders that are accompanied by other mental illnesses such as depression. Scientists currently think that, like heart disease and type 1 diabetes, mental illnesses are complex and probably result from a combination of genetic, environmental, psychological, and developmental factors. For instance, although NIMH-sponsored studies of twins and families suggest that genetics play a role in the development of some anxiety disorders, problems such as PTSD are triggered by trauma. Genetic studies may help explain why some people exposed to trauma develop PTSD and others do not. Several parts of the brain are key actors in the production of fear and anxiety. 15 Using brain imaging technology and neurochemical techniques, scientists have discovered that the amygdala and the hippocampus play significant roles in most anxiety disorders. The amygdala is an almond-shaped structure deep in the brain that is believed to be a communications hub between the parts of the brain that process incoming sensory signals and the parts that interpret these signals. It can alert the rest of the brain that a threat is present and trigger a fear or anxiety response. It appears that emotional memories are stored in the central part of the amygdala and may play a role in anxiety disorders involving very distinct fears, such as fears of dogs, spiders, or flying. The hippocampus is the part of the brain that encodes threatening events into memories. Studies have shown that the hippocampus appears to be smaller in some people who were victims of child abuse or who served in military combat.16, 17 Research will determine what causes this reduction in size and what role it plays in the flashbacks, deficits in explicit memory, and fragmented memories of the traumatic event that are common in PTSD. By learning more about how the brain creates fear and anxiety, scientists may be able to devise better treatments for anxiety disorders. For example, if specific neurotransmitters are found to play an important role in fear, drugs may be developed that will block them and decrease fear responses; if enough is learned about how the brain generates new cells throughout the lifecycle, it may be possible to stimulate the growth of new neurons in the hippocampus in people with PTSD.18. Current research at NIMH on anxiety disorders includes studies that address how well medication and behavioral therapies work in the treatment of OCD, and the safety and effectiveness of medications for children and adolescents who have a combination of anxiety disorders and attention deficit hyperactivity disorder.")
196
PSYCHIATRIC MANAGEMENT
Establish and maintain a therapeutic alliance Complete the psychiatric assessment Evaluate the safety of the patient Establish the appropriate setting for treatment Evaluate the functional impairment and quality of life Coordinate the patient’s care with the other clinicians Monitor the patient’s psychiatric status Integrate measurements into psychiatric management Enhance treatment adherence Provide education to the patient and the family ECPSLLC.COM

197
Monitor psychiatric status and safety.
Monitor the patient for changes in destructive impulses to self and others. Be vigilant in monitoring changes in psychiatric status, including major depressive symptoms and symptoms of potential comorbid conditions. Consider diagnostic reevaluation if symptoms change significantly or if new symptoms emerge.

198
PE • History of the present illness and current symptoms
• Psychiatric history, including symptoms of mania • Treatment history with current treatments and responses to previous treatments • General medical history • History of substance use disorders • Personal history (e.g., psychological development, response to life transitions, major life events) • Social, occupational, and family histories • Review of the patient’s medications • Review of systems • Mental status examination • Physical examination • Diagnostic tests as indicated
 • Social, occupational, and family histories. • Review of the patient’s medications. • Review of systems. • Mental status examination. • Physical examination. • Diagnostic tests as indicated.")
199
Items to Monitor Throughout Treatment
Symptomatic status, including functional status, and quality of life Degree of danger to self and others Signs of “switch” to mania Other mental disorders, including alcohol and other substance use disorders General medical conditions Response to treatment Side effects of treatment Adherence to treatment plan

200
Selection of Treatment: Make Your First Choice Count!
Aim for remission of symptoms Choose agents with proven efficacy Use optimal dose Minimize dropout Consider efficacy/tolerability/safety profile Maximize adherence Prevent relapse/recurrence Achieve remission of symptoms! Adequate duration Key Point As clinicians, it is imperative that we do everything in our power to ensure remission of symptoms is achieved Background Treatment should be selected to quickly and appropriately aggressively treat patients to remission with the first choice of therapy Many patients treated with antidepressant medications are not given adequate doses for a long enough period. Physicians should ensure that adequate doses of medication are administered and that patients are treated for an adequate duration Poor patient adherence is a common problem contributing to nonresponse, partial response, and relapse/recurrence. Education and information should be provided to the patient and family to combat this problem. Obstacles to adherence should be prospectively identified and eliminated to the extent possible. Patients should be educated that remission, and not just an improvement in symptoms, is the goal of treatment Achievement of remission has been shown to be a modifiable factor that can influence long-term prognosis; thus, the ideal approach to chronic, recurrent disease is prevention via earlier and effective treatment Reference American Psychiatric Association. Practice Guideline for the Treatment of Patients With Major Depression. 2nd ed. Washington, DC; 2000. American Psychiatric Association. Am J Psychiatry. 2000;157(4 suppl):1-45.
:1-45.")
201
Summary and Take-Home Messages
Patients can have a high rate of nonadherence with SSRIs due to adverse events First few weeks of therapy are critical Monitor medication compliance during this time period Choose a medication that is effective and generally well tolerated across indications We hope that this presentation will support you in being even more successful in your important efforts to help persons who suffer from depression and associated anxiety symptoms.

202
Onset of Adverse Events and Efficacy
Therapeutic Effect Adverse Events Antidepressant Therapy Time Adapted from American Psychiatric Association. Am J Psychiatry. 2000;157(Suppl 4):1-45. Bull SA, et al. Ann Pharmacother. 2002;36:
:1-45. Bull SA, et al. Ann Pharmacother. 2002;36:")
203
Side effects of antidepressant medications
1. Selective serotonin reuptake inhibitors a. Gastrointestinal b. Activation/insomnia c. Sexual side effects d. Neurological e. Falls f. Effects on weight g. Serotonin syndrome h. Drug interactions i. Discontinuation syndrome

204
Side effects of antidepressant medications
2. Serotonin norepinephrine reuptake inhibitors Venlafaxine, Desvenlafaxine, Duloxitine Nausea Dry mouth Sweating Agitation Sedation Weight Sexual Dysfunction Elevated Blood Pressure

205
Side effects of antidepressant medications
4. Tricyclic antidepressants a. Cardiovascular effects b. Anticholinergic side effects c. Sedation d. Weight gain e. Neurological effects f. Falls . g. Medication interactions

206
Side effects of antidepressant medications
5. Monoamine oxidase inhibitors a. Hypertensive crises b. Serotonin syndrome c. Cardiovascular effects d. Weight gain e. Sexual side effects f. Neurological effects

207
Buspar Nausea Dizziness

208
Psychotherapy . Specific psychotherapies Implementation
Cognitive and behavioral therapies Interpersonal psychotherapy Psychodynamic psychotherapy Problem-solving therapy Marital therapy and family therapy Group therapy Implementation Combining psychotherapy and medication

209
Complementary and alternative treatments
a. St. John’s wort b. S-adenosyl methionine c. Omega-3 fatty acids d. Folate e. N-Acetyl Cysteine f. Acupuncture G. Yoga

210
Assessing response and adequacy of treatment

211
Potential Reasons for Treatment Nonresponse
Inaccurate diagnosis Unaddressed co-occurring medical or psychiatric disorders, including substance use disorders Inappropriate selection of therapeutic modalities Inadequate dose of medication or frequency of psychotherapy Pharmacokinetic/pharmacodynamic factors affecting medication action Inadequate duration of treatment Nonadherence to treatment Persistent or poorly tolerated side effects Complicating psychosocial and psychological factors Inadequately trained therapist or poor “fit” between patient and therapist

212
Treatment Should Be Discontinued Gradually
Most antidepressants need to be tapered Gradually taper dose (1 dosage level per week)1 Longer-term treatment may require slower taper1,2 Discontinuation symptoms are possible soon after stopping drugs with short half-lives1,2 Counsel patients on possible discontinuation symptoms, including: Agitation, anorexia, diarrhea, dizziness, dry mouth, insomnia, nausea, nervousness, sensory disturbances, somnolence, and sweating1 Key Point It is important to discontinue treatment by tapering the dose to minimize the potential for adverse events Background Most antidepressants need to be tapered when discontinued. The drug should be tapered over a several-week period, which will allow any symptoms or recurrence to emerge and treatment to be resumed, if needed, while the patient is still partially treated1,2 As a rule of thumb, the dose should be tapered by approximately 1 dosage level per week.1 If treatment has been long term, or if the drug has a short half-life, a slower taper may be required.1,2 Tapering the drug may also minimize discontinuation symptoms, which can occur soon after stopping drugs with short half-lives1,2 Patients should be counseled on possible discontinuation symptoms1 References 1. EFFEXOR XR® (venlafaxine HCl) Prescribing Information. 2. American Psychiatric Association. Am J Psychiatry. 2000;157(suppl 4):1-45. 1. EFFEXOR XR® (venlafaxine HCl) Prescribing Information. 2. American Psychiatric Association. Am J Psychiatry. 2000;157(4 suppl):1-45.
1. Longer-term treatment may require slower taper1,2. Discontinuation symptoms are possible soon after stopping drugs with short half-lives1,2. Counsel patients on possible discontinuation symptoms, including: Agitation, anorexia, diarrhea, dizziness, dry mouth, insomnia, nausea, nervousness, sensory disturbances, somnolence, and sweating1. Key Point. It is important to discontinue treatment by tapering the dose to minimize the potential for adverse events. Background. Most antidepressants need to be tapered when discontinued. The drug should be tapered over a several-week period, which will allow any symptoms or recurrence to emerge and treatment to be resumed, if needed, while the patient is still partially treated1,2. As a rule of thumb, the dose should be tapered by approximately 1 dosage level per week.1 If treatment has been long term, or if the drug has a short half-life, a slower taper may be required.1,2 Tapering the drug may also minimize discontinuation symptoms, which can occur soon after stopping drugs with short half-lives1,2. Patients should be counseled on possible discontinuation symptoms1. References. 1. EFFEXOR XR® (venlafaxine HCl) Prescribing Information. 2. American Psychiatric Association. Am J Psychiatry. 2000;157(suppl 4): EFFEXOR XR® (venlafaxine HCl) Prescribing Information. 2. American Psychiatric Association. Am J Psychiatry. 2000;157(4 suppl):1-45.")
213
Considerations in the Decision to Use Maintenance Treatment
Risk of recurrence Severity of episodes Side effects experienced with continuous treatment Patient preferences Number of prior episodes; presence of comorbid conditions; residual symptoms between episodes Suicidality; psychotic features; severe functional impairments

214
SPECIFIC CLINICAL FEATURES INFLUENCING THE TREATMENT PLAN
Psychiatric Factors Demographic and Psychosocial Variables Co-occurring psychiatric disorders Treatment Implications of Co-occurring General Medical Conditions

215
Co-occurring psychiatric disorders
Dysthymic disorder Affective disorders Dementia Substance use disorders Personality disorders Eating disorders

216
Treatment Implications of Co-occurring General Medical Conditions
1. Hypertension 2. Cardiac disease 3. Stroke 4. Parkinson’s disease 5. Epilepsy 6. Obesity 7. Diabetes 8. Sleep apnea 9. Human immunodeficiency virus and hepatitis C infections 10. Pain syndromes 11. Obstructive uropathy 12. Glaucoma

217
Unmet Needs in Anxiety Underdiagnosed therefore untreated
Faster improvement Fewer side effects and better tolerability Greater efficacy Long term efficacy Despite all the advances made in the treatment of depression, there remains important unmet needs. We need therapeutic agents that help address these unmet needs. Source: Datamonitor, Stakeholder Insight: MDD, Q1.2; Adult population figures from and MDD prevalence rates applied. 217

218
National Survey Dispels Notion that Social Phobia is the Same as Shyness
social phobia is not simply shyness that has been inappropriately medicalized social phobia affects a minority of youth and only a fraction of those who consider themselves to be shy the greater disability that youth with social phobia experience and the greater likelihood that they will have another disorder they are not more likely to be getting treatment compared to their peers, questioning the notion that these youth are being unnecessarily medicated. Critics of the diagnosis have suggested that psychiatrists and pharmaceutical companies publicize social phobia, also known as social anxiety disorder, in order to increase sales of psychotropic medications, especially among youth. In addition, some have debated whether social phobia is just a “medicalization” of a normal variation in human temperament. The authors found that while about half of youth identified themselves as shy, only 12 percent of shy youth also met criteria for social phobia in their lifetime. Moreover, among youth who did not identify themselves as shy, about 5 percent met criteria for social phobia, suggesting that social phobia and shyness are not necessarily directly related. Rather, the presence of social phobia may be independent of shyness in some instances. Science Update • October 17, 2011 National Survey Dispels Notion that Social Phobia is the Same as Shyness Source: iStock Normal human shyness is not being confused with the psychiatric anxiety disorder known as social phobia, according to an NIMH survey comparing the prevalence rates of the two among U.S. youth. The study was published online ahead of print October 17, 2011, in the journal Pediatrics. Background Social phobia is a disabling anxiety disorder characterized by overwhelming anxiety and excessive self-consciousness in everyday social or performance situations. Critics of the diagnosis have suggested that psychiatrists and pharmaceutical companies publicize social phobia, also known as social anxiety disorder, in order to increase sales of psychotropic medications, especially among youth. In addition, some have debated whether social phobia is just a “medicalization” of a normal variation in human temperament. In response, Marcy Burstein, Ph.D., and colleagues at NIMH examined the rate of normal shyness among youth and its overlap with social phobia using data from the National Comorbidity Survey-Adolescent Supplement (NCS-A), a nationally representative, face-to-face survey of more than 10,000 teens aged sponsored by NIMH. Social phobia was assessed using standard diagnostic criteria set by the American Psychiatric Association's Diagnostic and Statistical Manual (DSM-IV). To assess shyness, teens were asked to rate how shy they felt around peers that they did not know well. Results of the Study In addition, those with social phobia were consistently more likely to also have another psychiatric disorder in their lifetime, like depression or a behavior or drug use disorder, compared to those who identified themselves as shy. Those with social phobia also showed higher levels of impairment in work or school, or among family or peers, though they were no more likely to be receiving professional treatment than those who were shy. Finally, rates of prescribed medication use were low for all groups. Only about 2.3 percent of those with social phobia were taking the antidepressant paroxetine (commonly used to treat anxiety disorders), while 0.9 percent who described themselves as shy were taking it. In addition, those with social phobia were no more likely to be taking any prescribed psychiatric medication compared to the other groups. Significance The results suggest that social phobia is not simply shyness that has been inappropriately medicalized. Rather, social phobia affects a minority of youth and only a fraction of those who consider themselves to be shy. In addition, despite the greater disability that youth with social phobia experience and the greater likelihood that they will have another disorder, they are not more likely to be getting treatment compared to their peers, questioning the notion that these youth are being unnecessarily medicated.
, a nationally representative, face-to-face survey of more than 10,000 teens aged sponsored by NIMH. Social phobia was assessed using standard diagnostic criteria set by the American Psychiatric Association s Diagnostic and Statistical Manual (DSM-IV). To assess shyness, teens were asked to rate how shy they felt around peers that they did not know well. Results of the Study. In addition, those with social phobia were consistently more likely to also have another psychiatric disorder in their lifetime, like depression or a behavior or drug use disorder, compared to those who identified themselves as shy. Those with social phobia also showed higher levels of impairment in work or school, or among family or peers, though they were no more likely to be receiving professional treatment than those who were shy. Finally, rates of prescribed medication use were low for all groups. Only about 2.3 percent of those with social phobia were taking the antidepressant paroxetine (commonly used to treat anxiety disorders), while 0.9 percent who described themselves as shy were taking it. In addition, those with social phobia were no more likely to be taking any prescribed psychiatric medication compared to the other groups. Significance. The results suggest that social phobia is not simply shyness that has been inappropriately medicalized. Rather, social phobia affects a minority of youth and only a fraction of those who consider themselves to be shy. In addition, despite the greater disability that youth with social phobia experience and the greater likelihood that they will have another disorder, they are not more likely to be getting treatment compared to their peers, questioning the notion that these youth are being unnecessarily medicated.")
219
About half of adults with an anxiety disorder had symptoms of some type of psychiatric illness by age 15, a NIMH-funded study shows. Results from a small clinical trial suggest that it might be possible, using computer-based training, to help children with anxiety shift their attention away from threat. Normal human shyness is not being confused with the psychiatric anxiety disorder known as social phobia, according to an NIMH survey comparing the prevalence rates of the two among U.S. youth.

220
Anxiety as a personality trait appears to be linked to the functioning of two key brain regions involved in fear and its suppression, according to an NIMH-funded study. Differences in how these two regions function and interact may help explain the wide range of symptoms seen in people who have anxiety disorders. The study was published February 10, 2011 in the journal, Neuron.

221
Youth with obsessive compulsive disorder (OCD) who are already taking antidepressant medication benefit by adding a type of psychotherapy called cognitive behavior therapy (CBT), according to an NIMH-funded study published September 21, 2011, in the Journal of the American Medical Association.
 who are already taking antidepressant medication benefit by adding a type of psychotherapy called cognitive behavior therapy (CBT), according to an NIMH-funded study published September 21, 2011, in the Journal of the American Medical Association.")
222
Anxiety Linked to Smarts in Brain Study Tendency to worry may have evolved along with intelligence in humans, researchers say

223
Health Tip: When Your Child is Stressed
Stress is a fact of life, and children are no less immune than their parents. How can you recognize if your child is "stressed out?" The American Academy of Pediatrics mentions these possible warning signs: Having physical problems, such as stomach ache or headache. Appearing agitated, tired or restless. Seeming depressed and unwilling to talk about his or her feelings. Losing interest in activities and wanting to stay at home. Acting irritable or negative. Participating less at school, possibly including slipping grades. Exhibiting antisocial behavior (stealing or lying), avoiding chores or becoming increasingly dependent on his or her parents.
, avoiding chores or becoming increasingly dependent on his or her parents.")
224
Mental Stress May Be Harder on Women's Hearts
Researchers Find Blood Flow to Women's Hearts Doesn't Increase in Face of Stress

225
Psychoeducation: Perhaps one of the most difficult aspects of coping with Social Phobia is simply understanding what it is, where it came from, why it's so hard to change, and how it keeps coming back with a vengeance. Psychoeducation involves you and your therapist working together to develop a better way to understand your Social Phobia, and subsequently, how to work with it. Cognitive Restructuring: As discussed earlier, individuals with Social Phobia frequently hold negative beliefs about themselves and others, which often show up as unhelpful thoughts in social situations. Cognitive restructuring is an important component of CBT, and it involves working with your therapist to identify these thoughts and look for patterns within them. As you become skilled at noticing these thoughts, you then develop strategies for gaining flexibility in your thinking and considering more helpful ways of looking at your experiences. In Vivo Exposure: In vivo (real life) exposure is another core element of CBT for Social Phobia. You and the therapist identify situations that you avoid because of Social Phobia, and then gradually enter these situations while accepting your anxiety and allowing it to naturally dissipate. While this step probably sounds quite intimidating, it is important to know that exposure is done at a very gradual, planned pace, and that your therapist will support you throughout the process. Many clients report exposure practices as being among the most useful elements in their treatment. Interoceptive Exposure: Some individuals with Social Phobia are fearful not only of social situations, but also of the anxious physical sensations (such as blushing, shaking, sweating, etc.) that can accompany them. Interoceptive exposure practices deliberately bring about these sensations through such activities as wearing a warm sweater to induce sweating in social situations. Just as exposure to feared situations leads to reductions in situational fear, exposure to feared sensations will lead to a reduction in anxiety over experiencing these feelings in social situations. Social Skills Training: In the midst of a tense social situation, many people with Social Phobia fear that they do not have the necessary social skills to successfully navigate the exchange. While this may be due to negative self-talk and self-consciousness (rather than an actual lack of skill), many people find it helpful to discuss such topics as carrying on conversations, being assertive, and effective listening. Social skills training provides a chance to work on these areas in therapy.
 exposure is another core element of CBT for Social Phobia. You and the therapist identify situations that you avoid because of Social Phobia, and then gradually enter these situations while accepting your anxiety and allowing it to naturally dissipate. While this step probably sounds quite intimidating, it is important to know that exposure is done at a very gradual, planned pace, and that your therapist will support you throughout the process. Many clients report exposure practices as being among the most useful elements in their treatment. Interoceptive Exposure: Some individuals with Social Phobia are fearful not only of social situations, but also of the anxious physical sensations (such as blushing, shaking, sweating, etc.) that can accompany them. Interoceptive exposure practices deliberately bring about these sensations through such activities as wearing a warm sweater to induce sweating in social situations. Just as exposure to feared situations leads to reductions in situational fear, exposure to feared sensations will lead to a reduction in anxiety over experiencing these feelings in social situations. Social Skills Training: In the midst of a tense social situation, many people with Social Phobia fear that they do not have the necessary social skills to successfully navigate the exchange. While this may be due to negative self-talk and self-consciousness (rather than an actual lack of skill), many people find it helpful to discuss such topics as carrying on conversations, being assertive, and effective listening. Social skills training provides a chance to work on these areas in therapy.")
226
Anxiety Disorder Association of American (ADAA)
The ADAA brings together professionals from many disciplines including psychiatrists, psychologists, social workers, physicians, nurses, etc. Through networks, the ADAA increases awareness about anxiety disorders, provides education resources, offers access to care, and supports research.

228
Yoga Accupuncture Warm bath, soothing music, exercise, massage, stay away from caffeine, Alcohol?, balance diet, avoid eating to relieve stress, appropiate meal times Alternative and Supplemental Medication Books/Autotapes Podcast Meditation and Mindfullness

230
Concluding Thoughts — There is a clear and pressing need for faster, robust and well tolerated therapy/therapies. Thinking is rapidly changing and evolving – combination strategies from treatment initiation may be the new frontier for patients who need greater efficacy than antidepressant monotherapy. Personalized medicine may be needed to address genetic differences in depressed individuals to achieve and maintain remission. 230

232
EDUCATIONAL RESOURCES FOR PATIENTS AND FAMILIES
Healthy Minds, Healthy Lives National Alliance on Mental Illness National Institute of Mental Health National Center for Complementary and Alternative Medicine Postpartum Support International MentalHelp.net

233
rx http://www.ocfoundation.org/CBT.aspx#ERP
OCD cannot be prevented. However, early diagnosis and treatment can help reduce the time a person spends suffering from the condition

236
An Important Law- The Yerkes Dodson Law

237
Another Bell Curve- Courtesy of Our Good Buddies Yerkes-Dodsen

238
Generalized Anxiety Disorder
General characteristics Prevalence and age of onset Comorbidity with other disorders

239
Generalized Anxiety Disorder: Psychosocial Causal Factors
The psychoanalytic viewpoint Classical conditioning to many stimuli The role of unpredictable and uncontrollable events A sense of mastery: immunizing against anxiety

240
Some Stats Andrews, Wahlberg, Montgomery (1993)
")
241
Employment

242
Depression

243
ANXIETY Galina Gerasimova Raeanne Perri Marisa Sevilla Joe Shen
Grace Velasquez ANXIETY

244
Overview What is Anxiety?
What are the different types of anxiety disorders? What are the causes? What are the symptoms? What are the treatments? Professional Resources available.

245
Anxiety Disorders One-Year Prevalence (Adults)
Anxiety Statistics Anxiety Disorders One-Year Prevalence (Adults) Percent Population Estimate* (Millions) Any Anxiety Disorder 13.3 19.1 Panic Disorder 1.7 2.4 Obsessive-Compulsive Disorder 2.3 3.3 Post-Traumatic Stress Disorder 3.6 5.2 Any Phobia 8.0 11.5 Generalized Anxiety Disorder 2.8 4.0 * Based on 7/1/98 U.S. Census resident population estimate of million, age 18-54
 Percent. Population Estimate* (Millions) Any Anxiety Disorder Panic Disorder Obsessive-Compulsive Disorder Post-Traumatic Stress Disorder Any Phobia Generalized Anxiety Disorder * Based on 7/1/98 U.S. Census resident population estimate of million, age")
246
Allopathic Treatments
Medications (Drug Therapy): Behavioral Therapy Cognitive Behavioral Therapy Psychodynamic Psychotherapy
: Behavioral Therapy. Cognitive Behavioral Therapy. Psychodynamic Psychotherapy.")
247
Medications Buspirone: shown to be effective but usually takes 3-4 weeks, particularly useful in elderly patients Benzodiazepines: include Xanax and Valium, act rapidly and successfully but can be addictive and loses effectiveness over time Side Effects: dizziness, headaches, nausea, impaired memory

248
Behavioral and Cognitive Therapy
Teaches patient to react differently to situations and bodily sensations that trigger anxiety Teaches patient to understand how thinking patterns that contribute to symptoms Patients learn that by changing how they perceive feelings of anxiety, the less likely they are to have them Examples: Hyperventilating, writing down list of top fears and doing one of them once a week, spinning in a chair until dizzy; after awhile patients learned to cope with the negative feelings associated with them and replace them with positive ones

249
Psychodynamic Psychotherapy
Psychodynamic therapy is a general name for therapeutic approaches which try to get the patient to bring to the surface their true feelings, so that they can experience them and understand them. Psychodynamic Psychotherapy uses the basic assumption that everyone has feelings held in the subconscious which are too painful to be faced. We then come up with defenses (such as denial) to protect us knowing about these painful feelings. Psychodynamic psychotherapy assumes that these defenses have gone wrong and are causing more harm than good, making you seek help. It tries to subdue them, with the intention that once you are aware of what is really going on in your mind the feelings will not be as painful. Takes an extremely long time and is labor intensive
 to protect us knowing about these painful feelings. Psychodynamic psychotherapy assumes that these defenses have gone wrong and are causing more harm than good, making you seek help. It tries to subdue them, with the intention that once you are aware of what is really going on in your mind the feelings will not be as painful. Takes an extremely long time and is labor intensive.")
250
Acupuncture Caused by the imbalance of chi coming about by keeping emotions in for too long Emotion effects the chi to move in an abnormal way: when fearful it goes to the floor, when angry the neck and shoulders tighten Redirects the chi into a balanced flow, releases tension in the muscles, increases flow of blood, lymph, and nerve impulses to affected areas Takes weekly sessions

251
Aromatherapy Calming Effect: vanilla, orange blossom, rose, chamomile, and lavender Reducing Stress: Lavender, sandalwood, and nutmeg Uplifting Oils: Bergamot, geranium, juniper, and lavender Essential Oil Combination: 3 parts lavender, 2 parts bergamot, and 1 part sandalwood

252
Exercise Benefits: symbolic meaning of the activity, the distraction from worries, mastery of a sport, effects on self image, biochemical and physiological changes associated with exercise, symbolic meaning of the sport Helps by expelling negative emotions and adrenaline out of your body in order to enter a more relaxed, calm state to deal with issues and conflicts

253
Meditation Cultivates calmness to create a sense of control over life
Practice: Sit quietly in a position comfortable to you and take a few deep breaths to relax your muscles, next choose a calming phrase (such as “om” or that with great significance to you), silently repeat the word or phrase for 20 minutes
, silently repeat the word or phrase for 20 minutes.")
254
Nutrition and Diet Therapy
Foods to Eat: whole grains, bananas, asparagus, garlic, brown rice, green and leafy veggies, soy products, yogurt Foods to Avoid: coffee, alcohol, sugar, strong spices, highly acidic foods, foods with white flour Keep a diary of the foods you eat and your anxiety attacks; after awhile you may be able to see a correlation East small, frequent meals

255
Vitamins B-Vitamins stabilize the body’s lactate levels which cause anxiety attacks (B-6, B-1, B-3) Calcium (a natural tranquilizer) and magnesium relax the nervous system; taken in combination before bed improves sleep Vitamin C taken in large doses also has a tranquilizing effect Potassium helps with proper functioning of adrenal glands Zinc has a calming effect on the nervous system
 and magnesium relax the nervous system; taken in combination before bed improves sleep. Vitamin C taken in large doses also has a tranquilizing effect. Potassium helps with proper functioning of adrenal glands. Zinc has a calming effect on the nervous system.")
256
Self Love The most important holistic treatment of all
Laugh: be able to laugh at yourself and with others; increases endorphin levels and decreases stress hormones Let go of frustrations Do not judge self harshly: don’t expect more from yourself than you do others Accept your faults

257
Additional Links Anxiety Screening Tools
Anxiety Disorders Association of America (ADAA) Freedom From Fear ( National Institute of Mental Health ( U.S. Dept. of Health & Human Services (
 Freedom From Fear ( National Institute of Mental Health ( U.S. Dept. of Health & Human Services (")
258
What is Anxiety? According to Kaplan and Sadock
Anxiety is “a diffuse, unpleasant, vague sense of apprehension, often accompanied by autonomic symptoms such as headache, perspiration, palpitations, tightness in the chest, mild stomach discomfort, and restlessness, as indicated by an inability to sit or stand still for long.”

259
Fear, Anxiety and Worry Normal emotional responses
Clear adaptive purpose In anxiety disorders, these normal responses become excessive, persistent, easily triggered, and disruptive to the person’s life.

260
Major Anxiety Disorders
Panic Disorder Generalized Anxiety Disorder Post Traumatic Stress Disorder Social Phobia Specific Phobia Obsessive Compulsive Disorder (OCD) Substance Induced Anxiety Disorder
 Substance Induced Anxiety Disorder.")
261
Epidemiology of PTSD Prevalence is 1% in the general population, and can be as high as 25% in those who have experienced trauma In combat veterans, prevalence is 20% Very high prevalence in women who are victims of sexual trauma

262
PTSD Costs Patients with PTSD are frequent users of the health care system Patients usually present to primary care physicians with somatic complaints After panic disorder, PTSD is the most costly anxiety disorder

263
Social Phobia Fear of being exposed to public scrutiny
Fear of behaving in a way which will be humiliating or embarrassing Symptomatic resemblance to panic disorder with anticipatory anxiety (person may be anxious/worrying far in advance of the event) Extensive phobic avoidance
 Extensive phobic avoidance.")
264
Social Phobia Distinction: anxiety only occurs when the patient is subject to the scrutiny of others (public speaking, oral exam, eating in the cafeteria) Phobic stimulus is avoided or endured with intense anxiety Fear and avoidant behaviors interfere with person’s normal routine or cause marked distress
 Phobic stimulus is avoided or endured with intense anxiety. Fear and avoidant behaviors interfere with person’s normal routine or cause marked distress.")
265
Epidemiology: Social Phobia
Prevalence rates vary depending on study; overall range is 3 –13% of the population Onset in adolescence Prevalence greater in females, but greater for males in clinical samples Frequent comorbidity with depression and substance abuse

266
Obsessive Compulsive Disorder (OCD)
Obsessions: recurrent, intrusive, unwanted thoughts (i.e. fear of contamination) Compulsions: behaviors or rituals aimed at reducing distress or preventing a dreaded event (i.e. compulsive handwashing)
 Compulsions: behaviors or rituals aimed at reducing distress or preventing a dreaded event (i.e. compulsive handwashing)")
267
OCD Symptoms Recurrent obsessions and/or compulsions are severe enough to consume more than one hour/day Person recognizes the obsession as a “product of his/her own mind”, rather than imposed from the outside, and that they are unreasonable or excessive

268
OCD Symptoms The obsessions are “ego-dystonic” (not enjoyable for the ego), as opposed to “ego-syntonic” (the ego likes it)
, as opposed to ego-syntonic (the ego likes it)")
269
Common Obsessions Contamination Repeated doubts Order
Aggressive or horrific images Sexual/pornographic imagery Scrupulosity

270
Obsessions and Common Compulsive Responses
Contamination: cleaning, hand washing, showering Repeated doubts: checking, requesting or demanding reassurances from others, counting Order: checking, rituals, counting Aggressive or horrific images, checking, prayers, rituals Sexual/Pornographic imagery: prayer/rituals

271
Epidemiology of OCD Lifetime prevalence is 2-3% in the general population Mean age of onset is mid-twenties, although men may develop symptoms earlier Less than 5% of patients develop disease after age of 35 years Chronic course, stress can exacerbate symptoms

272
Substance Induced Anxiety Disorder
Prominent symptoms of anxiety that are judged to be the direct physiological consequence of a drug or abuse, a medication or toxin exposure

273
Panic Attacks and Panic Disorder
Agoraphobia without a history of panic disorder Panic Disorder without agoraphobia Panic Disorder with agoraphobia

274
Post Traumatic Stress Disorder
Characterized by the re-experiencing of an extremely traumatic event accompanied by symptoms of increased arousal and by avoidance of stimuli associated with the trauma Symptoms present for at least one month If event just occurred and/or symptoms present for less than one month, a diagnosis of Acute Stress Disorder is given

275
Specific Phobia Clinically significant anxiety provoked by exposure to a specific feared object or situation, often leading to avoidance behavior

276
Obsessive Compulsive Disorder
Characterized by obsessions that cause marked anxiety or distress and/or compulsions that serve to neutralize anxiety

277
Substance Induced Anxiety Disorder
Anxiety Disorder not otherwise specified

278
E 00 Separation Anxiety DisorderE 01 Panic DisorderE 02 AgoraphobiaE 03 Specific PhobiaE 04 Social Anxiety Disorder (Social Phobia)E 05 Generalized Anxiety DisorderE Substance-Induced Anxiety DisorderE 12 Anxiety Disorder Attributable to Another Medical ConditionE 13 Anxiety Disorder Not Elsewhere ClassifiedPanic Attack
E 05 Generalized Anxiety DisorderE Substance-Induced Anxiety DisorderE 12 Anxiety Disorder Attributable to Another Medical ConditionE 13 Anxiety Disorder Not Elsewhere ClassifiedPanic Attack")
Similar presentations



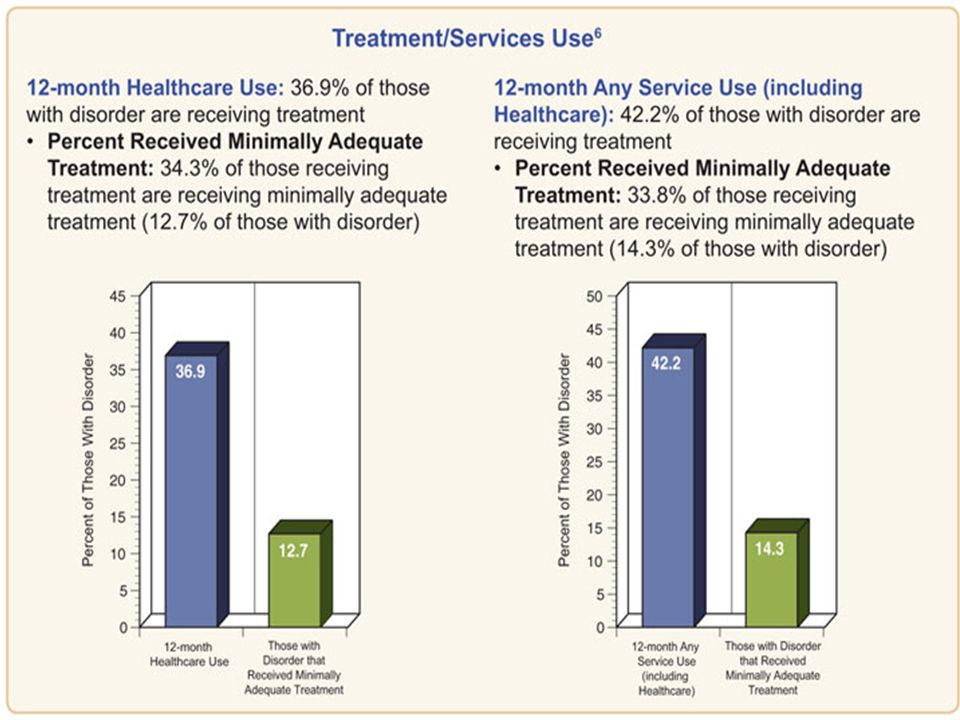










 What is it? Extremely worried about things like health, money, family/friend problems even when.>")














 What is it? –Everyone double checks things sometimes. For example, you might double check to make sure.>")
