NUR 134 NEO114 M. Johnston, RN-BC, M.Ed. OB Clinical Instructor NSCC Neonatal Assessment NUR 134 NEO114 M. Johnston, RN-BC, M.Ed. OB Clinical Instructor NSCC
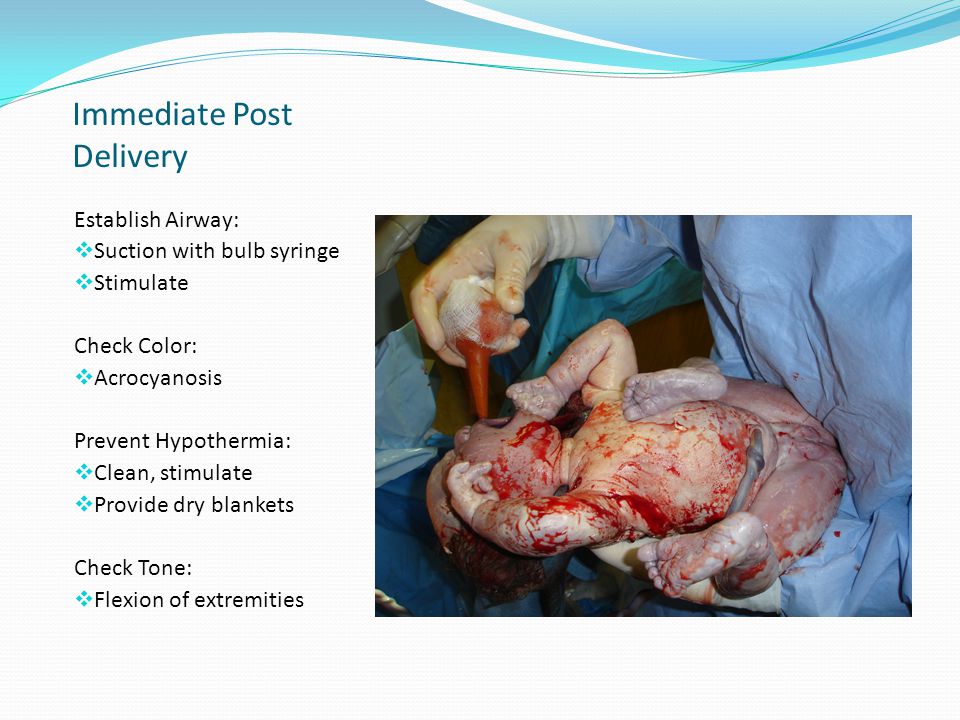
Immediate Post Delivery Establish Airway: Suction with bulb syringe Stimulate Check Color: Acrocyanosis Prevent Hypothermia: Clean, stimulate Provide dry blankets Check Tone: Flexion of extremities Suction mouth then nose, prevents infant from inhaling pharyngeal secretions by gasping as the nares are touched Frank breech position shown
Drying to prevent hypothermia Thermoregulation is balance between heat loss and heat production Cold stress increases need for oxygen and depletes glucose stores, increases resp. rate can result in metabolic acidosis Newborn has decrease ability to produce heat, blood vessels closer to surface Newborns have larger body surface to body weight Stabilize temp by placing skin to skin on mom’s abdomen and covering with warm blanket or radiant warmer Keep head covered and ambient room temperature without drafts
Apgar Scoring Five categories: score 0-2 Assessed at: 1 minute 5 minutes Rapid assessment of the newborn’s transition to extrauterine life, based on 5 physiologic states: vigorous cry, pink, HR > 100 assoc w/effective cardiopulmonary adaptation 1. Heart rate with stethoscope or palpating umb.cord 2. Resp rate based on observed movements 3. Muscle tone based on degree of flexion and extremities movement 4.Reflex Irritability based on response to bulb or catheter placed in nasopharanx 5. Color generalized: pallid, cyanotic or pink
Apgar Scoring Charts Evaluations are at 1 minute and 5 minutes Score 7-10 at 5 min. WNL healthy baby (parents need to be educated about this) if<7, do expanded Apgars every 5 minutes until >7 or transfer to SCN Score 4-6 at 5 min. moderate difficulty, close observation Score 0-3 at 5 min. severe distress usu. Transferred to NICU RN CNM or MD assigns the score Doesn’t really have long term predicative value such as development and intelligence (inappropriate use by researchers)
Apgar Scoring Dr. Virginia Apgar Apgar score was developed by Dr. Virginia Apgar as a means to evaluate the success of a newborn’s transition to extrauterine life; first rpesented in early 1950’s Also used to evaluate the effectiveness of resuscitation measures First MD to keep basic resuscitation equipment with her at all times for all deliveries First female full professor at Columbia University for Surgeons and Physicians Dr. Virginia Apgar "Nobody, but nobody, is going to stop breathing on me!"
Weight Measure length Head circumference Measurements done in metric and US System (grams and pounds) Weight normal range between 2500-4000 gms (5#8oz to 8#13 oz) Normal to lose 5-10% of weight in first few days (usu. about 6-10 oz) cause loss of excess fluid and low fluid intake 1st few days Length can be difficult to measure due to flexed position; crown to heel measurement 48-53 cm. or 19-21 in. Head circumference 33-35.5 (or 32 -36.8) cm or 13-14 in. measure widest part, occipito-frontal diameter
Newborn Exam Warm, dry surface Adequate lighting Calm infant First assessment is done immediately after birth (Apgars) then a comprehensive exam is completed within first 1-2 hours (RN) with normal newborn and again within 24 hours by provider
Check vital signs HR range 110-160 bpm Resp rate 30-60 min Temp. 36.5 – 37.5 C Heart rate auscultate apically PMI (4th intercosta,l L of midclavicular) one full minute; may be irregular, 110-160 bpm depending on activity level Respiratory rate 30-60 breathes per minute, often irregular, count for full minute when newborn quiet, periodic breathing Observe for symmetry of chest movement Temperature 36.5 - 37.5 or 97.7 – 99. Axillary
Normal Findings
Umbilical cord 3 vessels 2 arteries, 1 vein (AVA) Wharton’s jelly Check for 3 vessel cord 2 arteries - deoxygenated blood 1 vein - oxygenated blood Wharton’s jelly as protection no nerve endings
Umbilical Cord Healing 7-10 days Keep clean and dry Observe for infection Assess for hemorrhage (rare) or infection (omphalitis); stump is medium for bacterial growth Current recommendations for cord care (AWHONN 2001) cleaning with water only Usually cord clamp is removed at 24 hrs when drying and no longer bleeding Assess stump and base of cord for edema, erythema, odor and drainage with each diaper change Average cord separation is 10-14 days
Fontanels anterior posterior Sutures Fontanels occur at the junction at cranial bones where 2 or more sutures meet Sutures occur in the place where 2 cranial bones meet. Newborn’s sutures should be palpable with a small space between them; may be overlapping at birth Anterior fontanel: diamond shaped, larger than post. Closes between 12 – 18 months Posterior fontanel: triangular shaped, closes wihtin 1st 3 months of age Fontanels should be flat, not depressed or bulging
Head Molding Molding is the shaping of the fetal head by the overlapping of cranial bones to facilitate movement through the birth canal during labor
Vernix Caseosa Sebaceous gland secretions White, cheesy protective coating Develops 3rd trimester Decreases as fetus develops Protects skin from drying effects of amniotic fluid Normally found only in creases of term newborn
Milia sebaceous glands, usu Milia sebaceous glands, usu. found on face, nose and chin subsides spontaneously , reassure parents Small white spots on newborns face, nose, and chin; resemble pimples Subside spontaneously in a few days; reassure parents
Telangiectatic Nevi “Stork Bites” Telangiectatic nevi pale pink or red marks found at nape of neck, eyelids, or nose usu fair-skinned newborns Blanch when pressed fade with time
Erythema Toxicum Most common face, trunk, extremities Found in 70% of newborns Peaks at 24-48 hours old “Newborn rash or “fleabite dermititis” commonly occurs on chest, abdomen, back and buttocks term newborn, 1st 3 wks of age Thought to be inflammatory response transient , no clinical significance, requires no treatment
Lanugo Fine, downy hair Develops after 20 wks gestation Mostly disappears by 40 wks gestation
Meconium Formed during fetal life from amniotic fluid (and constituents) intestinal secretions (including bilirubin) and cells shed from mucosa 1st is sterile, then contain bacteria 1st mec. usually passed between 12-24 hrs old progressive changes in stool indicate healthy functioning GI tract
Mongolian spots Bluish black areas of pigmentation; may appear over any surface of body, most common on buttocks and back Most common in infants with dark skin (African, Hispanic, Mediterranean, Asian) also found in 5-13% Caucasians Fade gradually over months or years
Moro or Startle Reflex Hold infant in semi sitting position, allow head and trunk to fall backward (with support) Place infant on flat surface, make a loud noise Found in term infant This response is present at birth and may be seen until about 8 wks of age Symmetric abduction and extension of arms, fingers fan out and form C with thumb and forefinger; cry may be elicited Found in term infants, where the neuromuscular system is almost completely developed at birth
Normal Newborn Reflexes
Abnormal Findings
Neonatal Jaundice Physiological Pathologic Phototherapy Physiologic Jaundice occurs in about half of all healthy newborns and about 80% of preterms It arises sometime after 24 hrs after birth, yellow coloring gen. appears first on face and head then progressing towards the feet as bilirubin level rises hyperbilirubinemia caused by excessive Lab tests must be done for accuracy of the level, with attention to age of infant and degree of jaundice Pathologic Jaundice clinical jaundice evident within 24 hours after birth; if left untreated, results in acute encephalopathy Phototherapy best tmt is prevention; photometer to assure efficacy; must protect eyes, optimal skin exposure,; more at risk for fluid loss
Phototherapy
Cephalohematoma Does not cross suture line Cephalhematoma – collection of blood between skull bone and periosteum; does NOT cross the suture line; largest 2nd or 3rd day (bleeding stops) bleeding caused from pressure against maternal bony pelvis Caput Succedaneum – generalized edematous area of the scalp usually occipital area; extends ACROSS suture line and usually disappears in 3-4 days Cause – sustained pressure of vertex against cervix results in compression of vessels, slow venous return increases tissue fluids and causes edema can also be caused by vacuum extraction
Caput Succedaneum extends across the suture line usually disappears in 3-4 days Caput Succedaneum – generalized edematous area of the scalp usually occipital area; extends ACROSS suture line and usually disappears in 3-4 days Cause – sustained pressure of vertex against cervix results in compression of vessels, slow venous return increases tissue fluids and causes edema can also be caused by vacuum extraction
Tongue-tie occurs in approx. 4% of infants The frenulum attaches the underside of the tongue to the floor of the mouth, usually midway between the ventral surface and the tip A very thick or prominent frenulum (tongue tied) is quite rare presents difficulty with breastfeeding
Simian Crease (Single palmar crease) Usually associated with Downs Syndrome (Trisomy 21), but can be found in normal infants DS –combination of simian crease, short fingers, incurved little finger,, low set thumb, Overlapping of 2nd and 3rd fingers, possibility of Trisomy 18
Club Foot (Talipes Equinovarus) One of the most common congenital anomalies Incidence varies with race and sex (1:1000 births Caucasians, Asians least likely, highest African and Polynesians) Right affected more than left if unilateral Bilateral about 50% Variations in severity; may just need serial exercises and casting; orthopedic consult on day of birth
Sacral skin tag Pilonidal opening Palpate entire length of the spine to determine the presence of dorsal spinal processes and any abnormal curvatures Inspect from base of skull to coccyx, noting any skin disruptions, tufts of hair, soft or cystic masses, hemangiomas, or pilonidal dimple May be Sx of congenital spinal or neurologic anomaly Neural tube defects (pilonidal opening vs deep dimple)
Preterm Neonates SCN/NICU Preterm or premature- born before completion of 37th week gestation Late Preterm or Near Term –born between 34-37 weeks
Maternal Infant Bonding Parents share in the birth process 1st hour after critical for M/I contact, postpone everything not necessary until after 1st hour Early maternal infant contact; WHY? promotes successful breastfeeding important for developing relationship with newborn decreases postpartum depression decreases risk for hypothermia for newborn increases oxytocin and prolactin levels
Family Bonding Promote family bonding, not just with mother but fathers/partners, siblings, grandparents Childbirth practices and rituals of other cultures may not be congruent with standard practices associated with Anglo-American culture; be sensitive to cultural variations around birthing