Download presentation
Presentation is loading. Please wait.

1
20 Cardiovascular Disease and Physical Activity chapter

2
Learning Objectives Find out the major causes of death in the United States and how a lack of physical activity contributes to these conditions Understand the concept of risk factors and be able to identify the major risk factors for coronary artery disease (CAD) and hypertension Learn how atherosclerosis, hypertension, and CAD develop (continued)
 and hypertension Learn how atherosclerosis, hypertension, and CAD develop (continued)")
3
Learning Objectives (continued) Discover what specific physiological alterations resulting from exercise training reduce the risk of death from CAD, hypertension, and other cardiovascular diseases Learn what blood pressure changes result from endurance exercise training in moderately hypertensive individuals Find out if there is any risk of death with endurance exercise training
 Discover what specific physiological alterations resulting from exercise training reduce the risk of death from CAD, hypertension, and other cardiovascular diseases Learn what blood pressure changes result from endurance exercise training in moderately hypertensive individuals Find out if there is any risk of death with endurance exercise training")
4
The Leading Causes of Death in the United States in 2003 Data from American Heart Association, 2006.

5
Prevalence of Cardiovascular Disease In 2003 >1.2 million heart attacks ~480,000 deaths due to heart attacks ~1 in 5 deaths was attributable to CAD 1 in 2.7 deaths was attributable to cardiovascular diseases ~467,000 coronary artery bypass surgeries ~1,244,000 angioplasties Over 2,000 heart transplants

6
Factors Contributing to Decline in Deaths Improved public awareness (e.g., concept of risk factors) Increased use of preventive measures, including lifestyle changes Better and earlier diagnosis Improved drugs for specific treatment Better emergency and medical care
 Increased use of preventive measures, including lifestyle changes Better and earlier diagnosis Improved drugs for specific treatment Better emergency and medical care")
7
Cardiovascular Diseases Coronary artery disease (CAD) Hypertension Stroke Heart failure Peripheral vascular disease Valvular, rheumatic, and congenital heart disease
 Hypertension Stroke Heart failure Peripheral vascular disease Valvular, rheumatic, and congenital heart disease")
8
The Leading Causes of Death From Cardiovascular Disease Data from American Heart Association, 2006.

9
Coronary Artery Disease Coronary artery disease (CAD): involves atherosclerosis in the coronary arteries Atherosclerosis: progressive narrowing of the arteries due to plaque formation Ischemia: a deficiency of blood flow to the heart caused by CAD Angina pectoris: chest pain Myocardial infarction: a heart attack due to ischemia leading to irreversible damage and necrosis
: involves atherosclerosis in the coronary arteries Atherosclerosis: progressive narrowing of the arteries due to plaque formation Ischemia: a deficiency of blood flow to the heart caused by CAD Angina pectoris: chest pain Myocardial infarction: a heart attack due to ischemia leading to irreversible damage and necrosis")
10
Atherosclerosis Not a disease of the aged Pathological changes in the blood vessels begin in infancy and progress during childhood Rate of progression is determined by genetics and lifestyle factors (smoking, diet, physical activity, and stress)
")
11
Progressive Formation of Plaque in a Coronary Artery

13
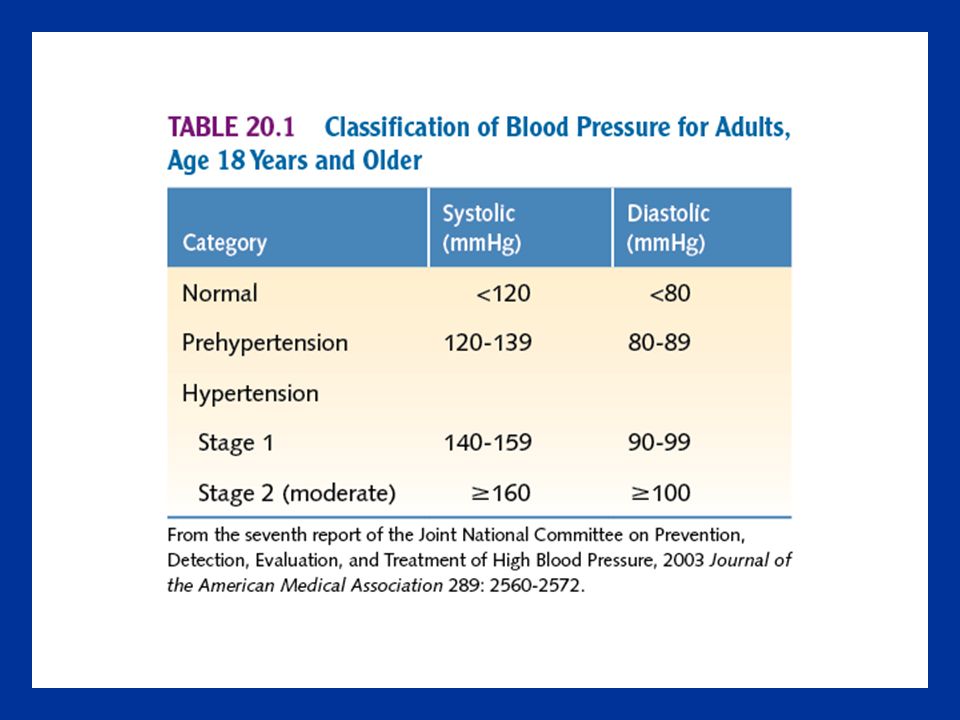
Hypertension In children: blood pressures above the 90th or the 95th percentile About one in every three adult Americans has hypertension Causes the heart to work harder Strains the systemic arteries and arterioles Can cause pathological hypertrophy of the heart Can lead to atherosclerosis, heart attacks, heart failure, stroke, and renal failure

14
Stroke Cardiovascular disease that affects the cerebral arteries Ischemic stroke –Cerebral thrombosis: a blood clot forms in a cerebral vessel, most often at the site of atherosclerotic damage –Cerebral embolism: an undissolved mass of material breaks loose from another site in the body and lodges in a cerebral artery Hemorrhagic stroke –Cerebral hemorrhage: rupture of one of the cerebral arteries –Subarachnoid hemorrhage: surface vessel on the brain ruptures, bleeding into the space between the brain and the skull

15
Congestive Heart Failure Heart muscle becomes too weak and cannot maintain adequate cardiac output It can result from damage to heart from: hypertension, atherosclerosis, valvular heart disease, viral infections, and heart attack Blood backs up in veins, causing systemic and pulmonary edema Can progress to irreversible damage, requiring a heart transplant

16
Other Cardiovascular Diseases Peripheral vascular disease Arteriosclerosis Valvular heart disease Rheumatic heart disease Congenital heart disease

17
The Three Layers of an Artery Wall

18
Pathophysiology of CAD Early theory: 1.Local injury induces dysfunction of the endothelium 2.Blood platelets and monocytes adhere to the exposed connective tissue 3.Platelets release platelet-derived growth factor that promotes smooth muscle cell migration from the media to the intima 4.Plaque forms at the site of injury 5.Lipids are attracted to the plaque

19
Changes in the Arterial Wall With Injury

20
Pathophysiology of CAD Newer theory: 1.Monocytes attach themselves to endothelial cells 2.Monocytes differentiate into macrophages and ingest oxidized LDL-C, becoming enlarged foam cells to form fatty streaks 3.Smooth muscle cells accumulate under the foam cells 4.Endothelial cells slough off, exposing underlying connective tissue 5.Platelets attach to exposed tissue

21
Illustration of Fissure or Rupture of an Unstable Plaque in a Coronary Artery

22
Plaque Composition Composition of the plaque and its fibrous cap is critical Small plaques (where there is typically less than 50% occlusion of the artery) that have thin fibrous caps and are heavily infiltrated with foam cells are the most dangerous
 that have thin fibrous caps and are heavily infiltrated with foam cells are the most dangerous")
23
Pathophysiology of Hypertension More than 90% of people with hypertension have essential hypertension Risk factors –Heredity, including race –Increasing age and male sex –Sodium sensitivity –Excessive alcohol consumption and use of tobacco products –Obesity and overweight –Diabetes or insulin resistance –Physical inactivity –Oral contraceptives –Pregnancy –Stress

24
Primary Risk Factors for CAD Tobacco smoking Hypertension Abnormal blood lipids and lipoproteins Physical inactivity Obesity and overweight Diabetes and insulin resistance

27
Proposed CAD Markers C-reactive protein (CRP): produced in the liver and smooth muscle cells within coronary arteries in response to injury or infection Fibrinogen: blood protein integral in the process of blood clotting Homocysteine: amino acid used to make protein Lipoprotein(a): similar to LDL-C; may reduce the ability to dissolve blood clots
: produced in the liver and smooth muscle cells within coronary arteries in response to injury or infection Fibrinogen: blood protein integral in the process of blood clotting Homocysteine: amino acid used to make protein Lipoprotein(a): similar to LDL-C; may reduce the ability to dissolve blood clots")
28
Lipoproteins Lipoproteins: proteins that carry blood lipids Low-density lipoproteins (LDL-C) High-density lipoproteins (HDL-C) Very low-density lipoproteins (VLDL-C) Ratio of total cholesterol to HDL-C is possibly the most accurate lipid index of risk for CAD –>5.0 = increased risk –<3.0 = low risk
 High-density lipoproteins (HDL-C) Very low-density lipoproteins (VLDL-C) Ratio of total cholesterol to HDL-C is possibly the most accurate lipid index of risk for CAD –>5.0 = increased risk –<3.0 = low risk")
29
Controllable Risk Factors for Hypertension Insulin resistance Obesity and overweight Diet (sodium, alcohol) Use of oral contraceptives Use of tobacco products Stress Physical inactivity
 Use of oral contraceptives Use of tobacco products Stress Physical inactivity")
30
Metabolic Syndrome Hypertension, coronary artery disease, obesity, and diabetes are linked through the common pathway of insulin resistance Metabolic syndrome, syndrome x, and insulin resistance syndrome are terms used to describe this interrelationship Obesity and/or insulin resistance could be the trigger that starts metabolic syndrome

31
Percentages of the U.S. Population at Increased Risk for Coronary Artery Disease Based on Primary Risk Factors Reproduced from Caspersen, C.J.: Physical activity and coronary heart disease. Physicians Sportsmedicine 1987; 15(11): 43-44.
:")
32
Reducing Risk Through Physical Activity Epidemiological evidence Physiological adaptations with training that might reduce risk Risk factor reduction with exercise training

33
Epidemiological Evidence Physical inactivity doubles the risk of CAD Low-intensity physical activity is sufficient to reduce the risk of this disease Health benefits do not require high-intensity exercise More vigorous exercise likely provides even greater benefits

34
Physical Activity vs. Physical Fitness Dose–Response Curve Reprinted, by permission, from P.T. Williams, 2001, "Physical fitness and activity as separate heart disease risk factors: A metaanalysis," Medicine and Science in Sports and Exercise 33: 754-761.

35
Aerobic Training Adaptations Produce larger coronary arteries which increases the capacity for blood flow to the heart Increased cardiac pumping capacity Improved collateral circulation in the heart Improved endothelial function Reduce blood pressure (~7 mmHg) in individuals with mild to moderate hypertension Improves cholesterol ratio Weight reduction Improves insulin sensitivity Stress management
 in individuals with mild to moderate hypertension Improves cholesterol ratio Weight reduction Improves insulin sensitivity Stress management")
36
Comparison of the Left Main Coronary Artery in (a) Sedentary and (b) Exercising Monkeys on Atherogenic Diets
 Sedentary and (b) Exercising Monkeys on Atherogenic Diets")
37
Reducing the Risk of Hypertension Through Exercise People who are active and those who are fit have reduced risk for developing hypertension Increased plasma volume that accompanies physical training does not increase blood pressure due to training-induced increased capillarization and increased venous capacity Resting blood pressure decreases by training in people with hypertension

38
Risk of Heart Attack and Death During Exercise Deaths during exercise are rare, although typically highly publicized Deaths during exercise in people over 35 usually are caused by a cardiac arrhythmia resulting from atherosclerosis Deaths during exercise in people under age 35 are usually caused by hypertrophic cardiomyopathy, congenital coronary artery abnormalities, aortic aneurysm, or myocarditis

39
Risk of Primary Cardiac Arrest During Vigorous Exercise and at Other Times Throughout a 24 h Period Data from D.S. Siscovick et al., 1984, "The incidence of primary cardiac arrest during vigorous exercise," New England Journal of Medicine 311: 874-877.

Similar presentations





, fibrous material and.>")













 Atheroma as the presence of fatty material within the walls of arteries. The link between atheroma and the increased.>")
