Download presentation
Presentation is loading. Please wait.

1
Pregnancy and Anaemia Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics, Phd (physio) Mahatma Gandhi Medical college and research institute puducherry, India
 Mahatma Gandhi Medical college and research institute puducherry, India.")
2
Definitions and terms Anaemia is defined as qualitative or quantitative reduction in circulating haemoglobin mass resulting in reduced O 2 carrying capacity of the blood to the vital organs and tissues. 11 gm % first and third trimester but reduction of 0.5 Gm% in second trimester 10 gm% in India

3
Why should we know this ?? According to W.H.O, the prevalence of Anaemia in pregnancy in south East Asia is around 56%. In India incidence of anaemia pregnancy has been noted as high as 40-80%. Nurses study in kumbakonam – a few years back – more than 95 % were having Hb of 9 or below !!

4
Why should we know this ?? Maternal and foetal problems About 4-16% of maternal death is due to anaemia. Poor weight gain, CCF, PIH, dysfunctional labour, PROM etc., Postnatal sepsis and subinvolution strong association between moderate-to-severe anaemia at 28 weeks gestation (on average) and greater severity of blood loss at delivery and postpartum. prematurity, low birth weight, poor Apgar score, foetal distress, neonatal distress requiring prolonged resuscitation
 and greater severity of blood loss at delivery and postpartum. prematurity, low birth weight, poor Apgar score, foetal distress, neonatal distress requiring prolonged resuscitation.")
5
Classification mild degree (9-11 g%), ( 9- 10 for us !!) moderate (7-9 g%), severe (4-7 g%) and very severe (<4 g%).
, ( for us !!) moderate (7-9 g%), severe (4-7 g%) and very severe (<4 g%).")
6
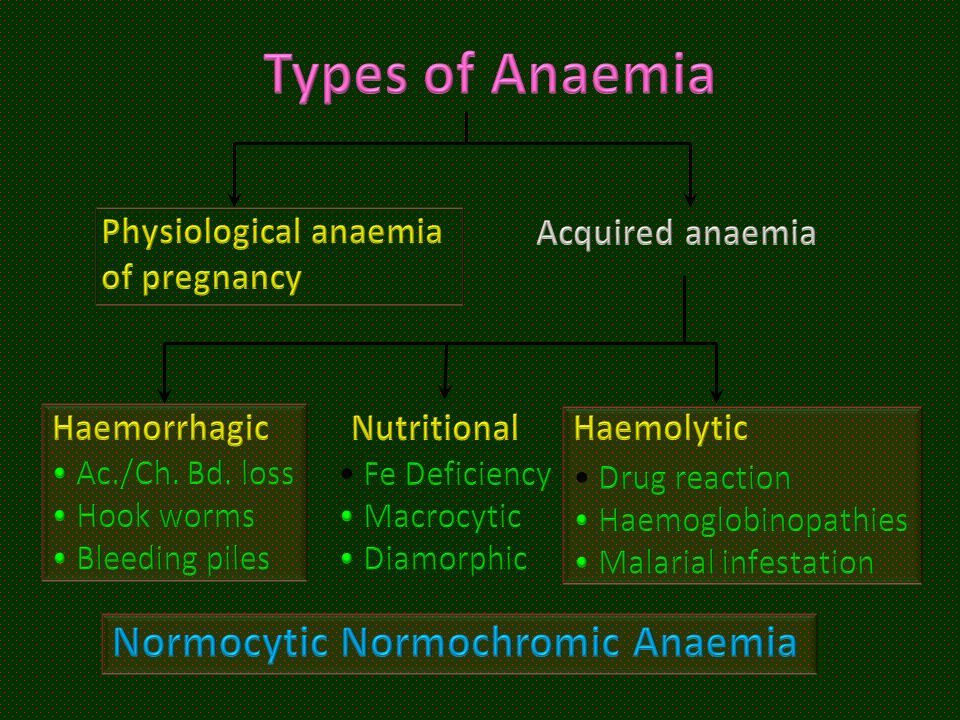
Etiology A. Physiological anaemia of pregnancy Acquired: a. Nutritional- Iron deficiency, folate deficiency, B-12 deficiency, etc. b. Infections- Malaria, hookworm infestation, etc c. Haemorrhagic- Acute or chronic blood loss d. Bone marrow suppression- Aplastic anaemia, drugs, etc. e. Renal disease C. Genetic - haemoglobinopathies – sickle cell disease,thalassaemia, etc

8
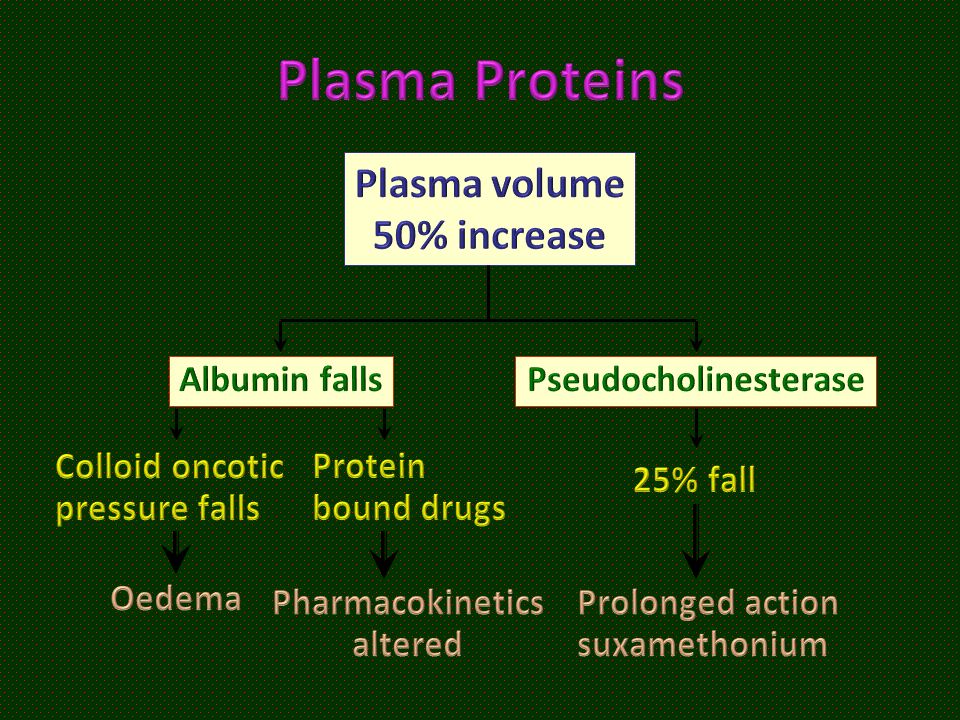
Normal changes Maternal blood volume begins to increase early at 6th week and continues to rise by 45-50% till 34 weeks of gestation, returning to normal by 10-14 days postpartum. RBC increase – but less (only 30 – 35 % ) Plasma volume increase So physiological anaemia- never above 15 % decrease
 Plasma volume increase So physiological anaemia- never above 15 % decrease.")
9
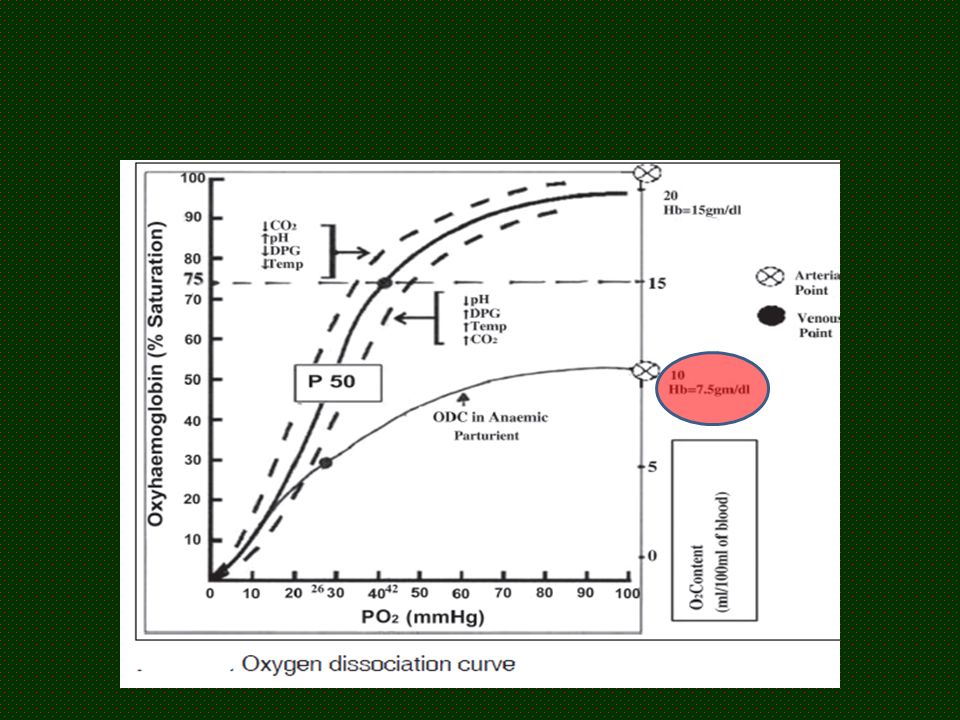
Compensatory factors (Anaemia in Pregnancy) Increase in cardiac output -- More than 10 liters – CCF may ensue. Increase in 2, 3 DPG levels result in shift of ODC to the right which facilitates greater unloading of O 2 to the tissues. Decrease blood viscosity: The change in blood rheology promotes microcirculation in the tissues and provides better oxygenation. Release of renal erythropoietin leading to stimulation of erythroid precursors in bone marrow A-- BCDE

13
Signs and symptoms

14
Why should there be such a problem here?? A pregnant woman requires about 2 to 4.8 mg iron every day. To have it from the dietary sources she must consume 20-48 mg of dietary iron. practically impossible in India because of average vegetarian diet does not contain more than 10-15 mg of iron Nutritional prophylaxis : 60 mg elemental iron and 500 micrograms of folicacid daily for 100 days to all pregnant women

15
Pregnancy with anaemia management

16
Severe anemia

17
Iron therapy

18
Complications of Parenteral iron

19
ANAESTHETIC CONSIDERATIONS

20
Preoperative assessment History Clinical signs Investigations should include a complete haemogram, reticulocyte count, peripheral smears and blood grouping RFT and ECG

21
Do we need to transfuse preop ??

22
Is there a minimum Hb ?? Hb > 10 – don’t transfuse Hb < 6 – transfuse 7-8-9 wait and decide on surgery, clinical conditions, urgency,ongoing bleeding, threat of bleeding etc.. Clinical

23
Controversial !! Should there be a symptom based transfusion Or Should there be Hb based transfusion ??

24
Moderate anaemia

25
Choice of anaesthesia !! Avoidance of hypoxia Maintain cardiac output Maintain ODC Goals

26
The essence of GA

27
Regional anaesthesia Preloading is ?? required since the patient has to deal with auto- transfusion after baby delivery. Use of low dose bupivacaine in combination with fentanyl Aorto-caval compression effects can be exaggerated. Mechanical manoeuvres such as lateral table tilt, pelvic wedge and manual displacement can be used to overcome IVC compression. If vaso pressors are required; phenyl ephrine is a good choice. No tachy !!

28
Regional anaesthesia Avoid use of intravenous fluids to treat hypotension, instead use vasopressors. Head down tilt can be tried but lungs should be continuously auscultated to rule out lung congestion and overload.

29
Regional anaesthesia Oxygen administration should be continued throughout surgery and postoperatively. After delivery if the SpO2 falls and there are lung signs and tachypnoea, diuretics should be considered to offload the volume overload

30
Regional anaesthesia Sedation to keep the patient calm and prevent anxiety induced tachycardia. Patient and fluid warming devices to prevent fall in core temperature and shivering. Good analgesic plan to prevent postoperative pain and neuro- endocrine response. Transversus abdominis plane block is a good choice.

31
Aggressive blood replacement of blood loss Hgb <6 g/dL – Transfusion recommended except in exceptional circumstances ●Hgb 6 to 7 g/dL – Transfusion generally likely to be indicated

32
●Hgb 7 to 8 g/dL – Transfusion should be considered in postoperative surgical patients, including those with stable cardiovascular disease, after evaluating the patient’s clinical status ●Hgb 8 to 10 g/dL – Transfusion generally not indicated, considered (eg, those with symptomatic anemia, ongoing bleeding, acute coronary syndrome with ischemia) ●Hgb >10 g/dL – Transfusion generally not indicated except in exceptional circumstances
 ●Hgb >10 g/dL – Transfusion generally not indicated except in exceptional circumstances")
33
The best is Consider clinical scenes and judge Prevent by deworming, oral iron antenatally

34
Clinical tips In pregnancy, pre-autologous deposit is not recommended. Cell salvage is recommended for women in whom an intraoperative blood loss of more than 1500 ml is anticipated Protocol for management of OBS. Hge. PRC in cases with antibodies Cytomegalovirus (CMV) seronegative red cells should be provided for elective transfusions in pregnancy but standard, leucodepleted units may be used in an emergency
 seronegative red cells should be provided for elective transfusions in pregnancy but standard, leucodepleted units may be used in an emergency.")
35
Communicate with transfusion specialist

36
Sickling Anaesthetic management aims at avoidance of hypoxemia, hypovolemia, hypothermia and acidosis along with provision of good analgesia. Hb of > 8 gm with HbA of more than 40 %

37
Thalassaemias Thalassaemias are a diverse group of microcytic, haemolytic anaemias wherein there is a reduced synthesis of one or more of the polypeptide globin chains. Chronic anaemia, iron overload for the heart and difficult airway

38
Summary Definition Incidence Two classifications A-BCDE Pre op Goals Technique – GA / RA

Similar presentations






< 11g/dl. Chronic.>")











, Dip. Diab. DCA, Dip. Software statistics Ph D (physiology) Mahatma Gandhi medical college and research institute,>")
 Children >")