Download presentation
Presentation is loading. Please wait.

2
Objectives : When you complete this section ,you should be able to :
1- Explain where blood is produced in the fetuses, children& adults. 2- describe the stages of blood cells production & state the factors that influence its rate. 3- How uncommitted stem cells become committed to forming specific types of blood cells.

8
Conc. Of Hb in 100 RBC=34gr. 2.5M 1M 7-8 Carbonic anhydrase O2 V=90-95cuM

13
ERYTHROPOIESES

14
Concentration of RBC s Normal RBC count in adult male= Million/cu.mm. female= M/cu.mm. In new born infant=6-6.5 or7M/cu.mm. When RBCs increases above normal range it is called ERYTHROCYTOSIS. Causes are; pathological OR physiological ex. New born or after exercise or living at very high altitude. Pathological; polycythemia vera. When the number of RBC or their hemoglobin (Hb) concentration decreases the condition is called ANAEMIA.Normal Hb= Normochromia, low Hb concentration=Hypochromia there is No HYPERCHROMIA .
 concentration decreases the condition is called ANAEMIA.Normal Hb= Normochromia, low Hb concentration=Hypochromia there is No HYPERCHROMIA .")
17
Regulation of RBC Production
Tissue oxygenation is the basic regulator of RBC production . Anemia , Blood loss or any other cause of hypoxia increases RBC production It is the functional ability of RBCs to transport oxygen to the tissues in relation to the tissue demand for oxygen & not RBC concentration that control the rate of RBC production. Erythropoietin:90% is formed in the kidneys in response to hypoxia. It is a principle factor that stimulate RBCs production. It’s a glycoprotein, M.W. =40,000 ,in the absence of erythropoietin hypoxia has no effect or very little effect in stimulating RBCs production .Hypoxia causes marked increase in erythropoietin production &this intern increases RBC production until hypoxia is relieved.

18
Factors that decrease oxygenation
1- Low blood volume . 2- Anemia . 3- Low hemoglobin . 4- poor blood flow . 5-Pulmonary diseases . 6-Bone marrow destruction by X-ray. 7-Living at very high altitude . All of the above factors increases Erythropoietin, its important effects are : A) to stimulate the production of proerythroblasts from hemopoietic stem cells in the bone marrow .B) It causes these cells to pass more rapidly through erythroblastic stages than normally C) It speed up the production of new RBC until enough RBC carry adequate amounts of O2 to the tissues.
 to stimulate the production of proerythroblasts from hemopoietic stem cells in the bone marrow .B) It causes these cells to pass more rapidly through erythroblastic stages than normally C) It speed up the production of new RBC until enough RBC carry adequate amounts of O2 to the tissues.")
19
10% After five days

20
Norepinephrine, epinephrine, some prostaglandins stimulate the production of erythropoietin. Hypoxia is the major factor. Epinephrine, norepinephrine, prostaglandins, increases erythropoietin production.

23
Requirements for RBC Maturation
1- Vitamin B12(cyanocobalamin) OR Maturation factor. 2- Folic Acid present in Green vegetables . Both are essential for the synthesis of DNA.for formation of thymidine triphosph. Lack of them causes failure of nuclear maturation and cell division . 3-Intrinsic Factor its deficiency causes poor absorption of vit. B12 as in (pernicious Anemia): atrophic gastric mucosa fail to produce normal gastric secretions. Deficiency of (B12,Folic acid or IF) causes Macrocytic Normochromic Anemia.
 OR Maturation factor. 2- Folic Acid present in Green vegetables . Both are essential for the synthesis of DNA.for formation of thymidine triphosph. Lack of them causes failure of nuclear maturation and cell division . 3-Intrinsic Factor its deficiency causes poor absorption of vit. B12 as in (pernicious Anemia): atrophic gastric mucosa fail to produce normal gastric secretions. Deficiency of (B12,Folic acid or IF) causes Macrocytic Normochromic Anemia.")
24
Intrinsic Factor It is secreted by the parietal cells of gastric glands. It is a glycoprotein . 1-It binds with vitamin B12, protect it from digestion 2-In this state (IF+vitaminB12) bound to special receptor sites in the mucosa of the ileum. 3- Vitamin B12+IF as acomplex transported into the blood by process of pinocytosis. 4- Vitamin B12 is stored in the liver then released slowly when needed by the bone marrow for the formation of RBCs.Its deficiency OR B12 deficiency cause Macrocytic Normochromic Anemia. { 1-3μ.} is needed daily for the maturation of RBCs. The liver storage of B12 normally range between μ.
 bound to special receptor sites in the mucosa of the ileum. 3- Vitamin B12+IF as acomplex transported into the blood by process of pinocytosis. 4- Vitamin B12 is stored in the liver then released slowly when needed by the bone marrow for the formation of RBCs.Its deficiency OR B12 deficiency cause Macrocytic Normochromic Anemia. { 1-3μ.} is needed daily for the maturation of RBCs. The liver storage of B12 normally range between μ.")
25
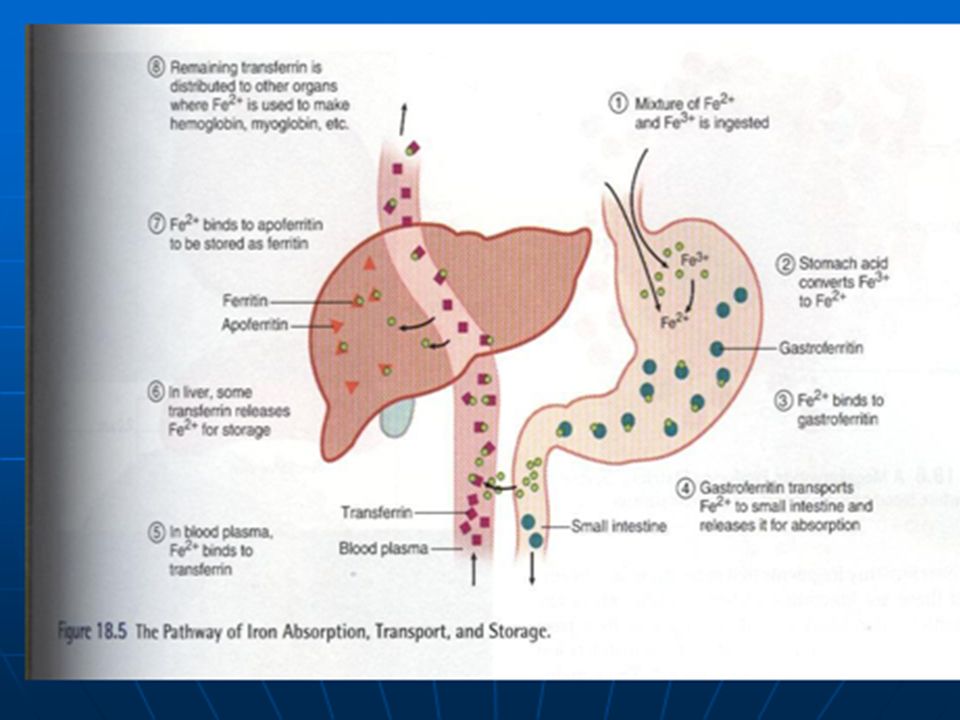
IRON METABOLISM Iron is important for the formation of
Hb,myoglobin,cytochromes (peroxidase and catalase enzymes) . Total quantity of iron=4-5 grams . 65% in the form of Hb. 4% in the form of myoglobin. 1% in the form of various heme compounds for intracellular oxidation 0.1% combined with transferrin. 15-30% stored in the liver (ferritin, hemosidrin). DAILY REQUIERMENT (INTAKE) =DAILY LOSS. In men =0.6 mg/day ,In women =1.3mg/day.
 . Total quantity of iron=4-5 grams . 65% in the form of Hb. 4% in the form of myoglobin. 1% in the form of various heme compounds for intracellular oxidation. 0.1% combined with transferrin % stored in the liver (ferritin, hemosidrin). DAILY REQUIERMENT (INTAKE) =DAILY LOSS. In men =0.6 mg/day ,In women =1.3mg/day.")
26
Transport and storage of Iron
1.Iron absorbed from the small intestine, combines with a beta globulin,apotransferrin, to form transferrin; the combination is loose. 2.sixty% of excess iron is stored in the liver in combination with apoferritin to form ferritin(storage iron) 3.Smaller quantities of excess iron is stored in an insoluble form called hemosiderin. Iron can be easily removed from ferritin when the level of iron in the plasma become very low ;but not from hemosiderin. Trasferrin molecule bind with receptors on the cell membrane of erythroblasts in the bone marrow ingested by endocytosis. Iron delivered directly into mitochonderia where heme is synthesized. Deficiency of transferrin cause failure to transport iron & causes severe hypochromic anemia
 3.Smaller quantities of excess iron is stored in an insoluble form called hemosiderin. Iron can be easily removed from ferritin when the level of iron in the plasma become very low ;but not from hemosiderin. Trasferrin molecule bind with receptors on the cell membrane of erythroblasts in the bone marrow ingested by endocytosis. Iron delivered directly into mitochonderia where heme is synthesized. Deficiency of transferrin cause failure to transport iron & causes severe hypochromic anemia")
30
Iron deficiency Iron deficiency or transferrin deficiency causes iron deficiency anemia ,the red blood cells become smaller than normal=microcytes Their hemoglobin concentration is less than normal=hypochromia.The cells in this type of anemia are Microcytic Hypochromic type.

Similar presentations




























Transportation -Gases (O 2 and CO 2 ) -Nutrients -Heat and waste -Hormones 2)Regulation.>")



i.>")

, FRSH (London) Professor of Physiology, College of Medicine & The Blood Bank,>")
![ERYTHROCYTES [RBCs] Lecture – 2 Dr. Zahoor Ali Shaikh 1.](/25/7604649/big_thumb.jpg "ERYTHROCYTES [RBCs] Lecture – 2 Dr. Zahoor Ali Shaikh 1.>")