Download presentation
Presentation is loading. Please wait.

1
RADIATION AND Pregnancy: an update
A/Prof Sandra Lowe .

2
The impact of radiation dose on management of following conditions:
Diagnosis of pulmonary embolus Breast cancer Motor vehicle accident with suspected pelvic and sternal frcatures Flight from Paris to Tokyo Suspected carotid artery dissection

3
Terminology Radiation doses are expressed as Gray or mGy 1Gy=100 rad
Dose limits are expressed as Sieverts, which takes into account weighting factors for the particle type to reach the equivalent absorbed dose Nuclear medicine and PET: dose is delivered as MBq

4
Occupational Limits 100 mSV/5 yrs; <50mSv in any 1 year
pregnancy, this should be minimised, aim < 1mSv microwave ovens, video display terminal, mobile phones = 0

6
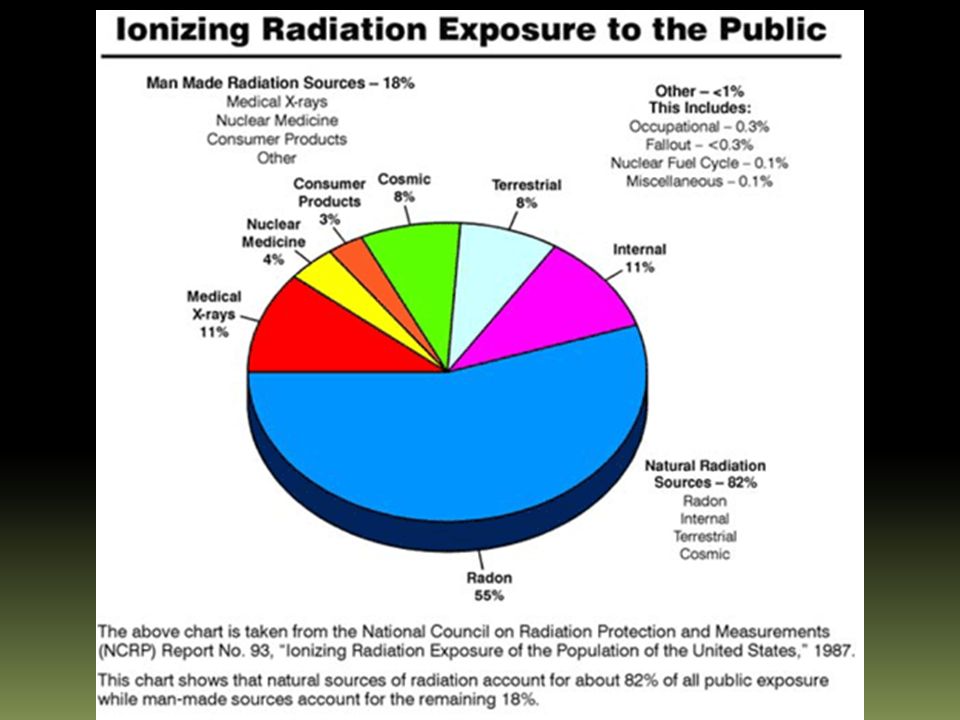
Background radiation

7
Air Travel short haul flight - 0.001-0.003mSv/hr
long haul flight mSV/hr

8
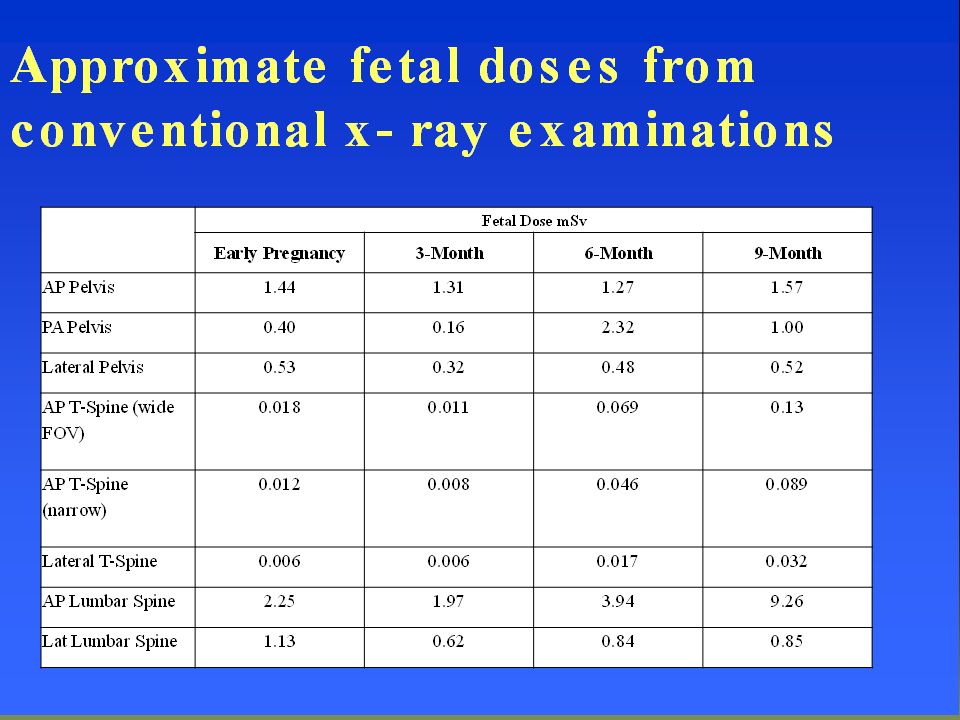
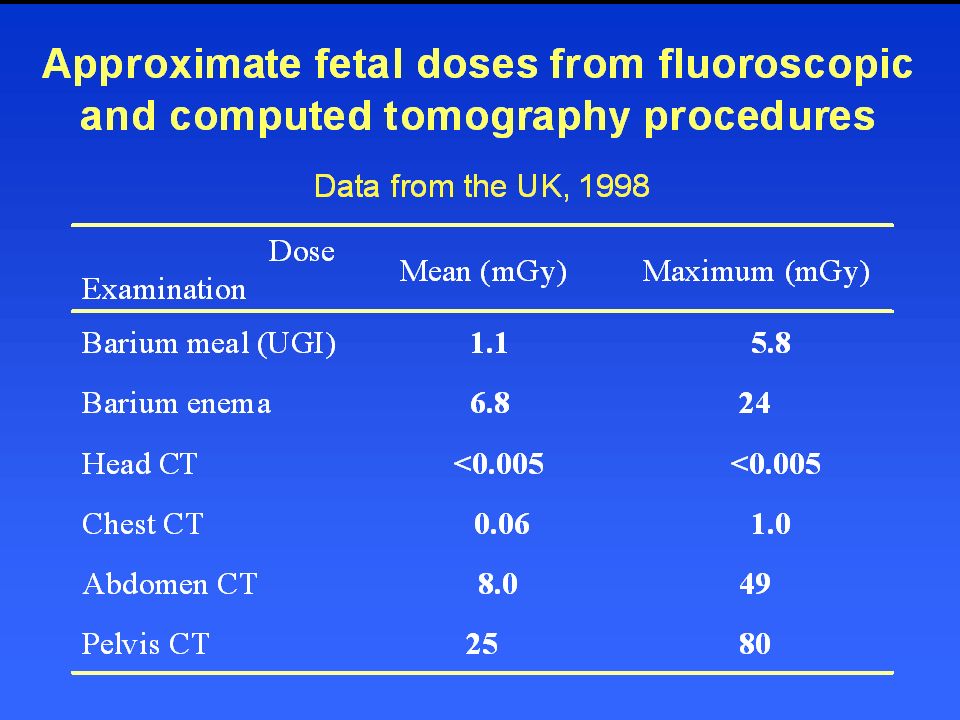
Diagnostic Radiography
X-ray CT Scanning Nuclear medicine/PET MRI

9
Fetal absorbed dose : Varies with type of procedure
technique eg digital versus conventional, fluroscopy dose eg Single shot IVP maternal factors - “thickness” fetal factors - gestation

10
Protraction and fractionation
decreases the severity and increase the threshold for deleterious tissue reactions Eg of protracted radiation: exposure while flying some occupational exposures exposure to a radionuclide with a long half-life. Eg of fractionation multiple diagnostic x-ray procedures over a period of hours or days radiation therapy during pregnancy to body areas other than the abdomen eg breast over a period of weeks.

13
CT Contrast agents Significant iodine load may induce blockade of fetal thyroid non-ionic contrast agents cross placenta and inhibit Type II and III deiodinases which can reduce intracellular T3 no evidence of teratogenicity and fetal thyroid does not become functional until weeks

14
New technology to reduce fetal dosage eg chest CT
European Journal of Radiology. 83(7): , 2014 Jul. Technique Fetal Dose T3 (mSv) Impact on fetal dose T3 Standard chest CT 8DR 64DR with DASC + ATCM + ASiR 0.22 0.13 42% 64DR with DASC + ATCM + ASiR + +Bismuth-antimony shields .04 69% Maternal dose 4.0 2.5 DR: detector row DASC: dynamic adaptive section collimation ATCM: automatic tube current modulation AsiR: adaptive statistical iterative reconstruction
: , 2014 Jul. Technique. Fetal Dose T3 (mSv) Impact on fetal dose T3. Standard chest CT. 8DR. 64DR with DASC + ATCM + ASiR 42% 64DR with DASC + ATCM + ASiR + +Bismuth-antimony shields 69% Maternal dose DR: detector row DASC: dynamic adaptive section collimation ATCM: automatic tube current modulation AsiR: adaptive statistical iterative reconstruction")
15
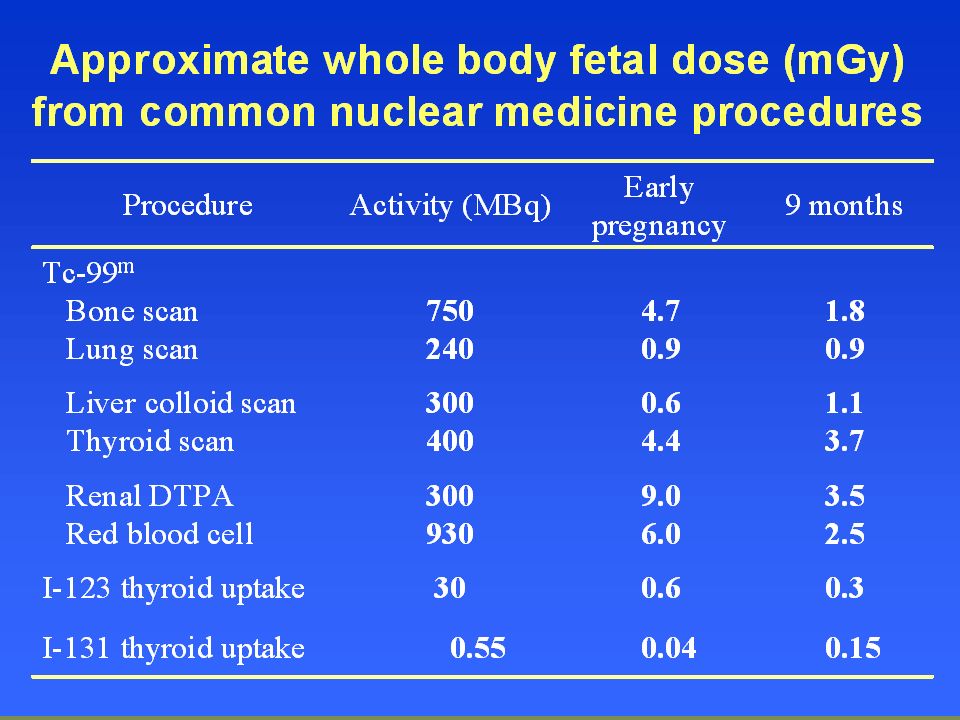
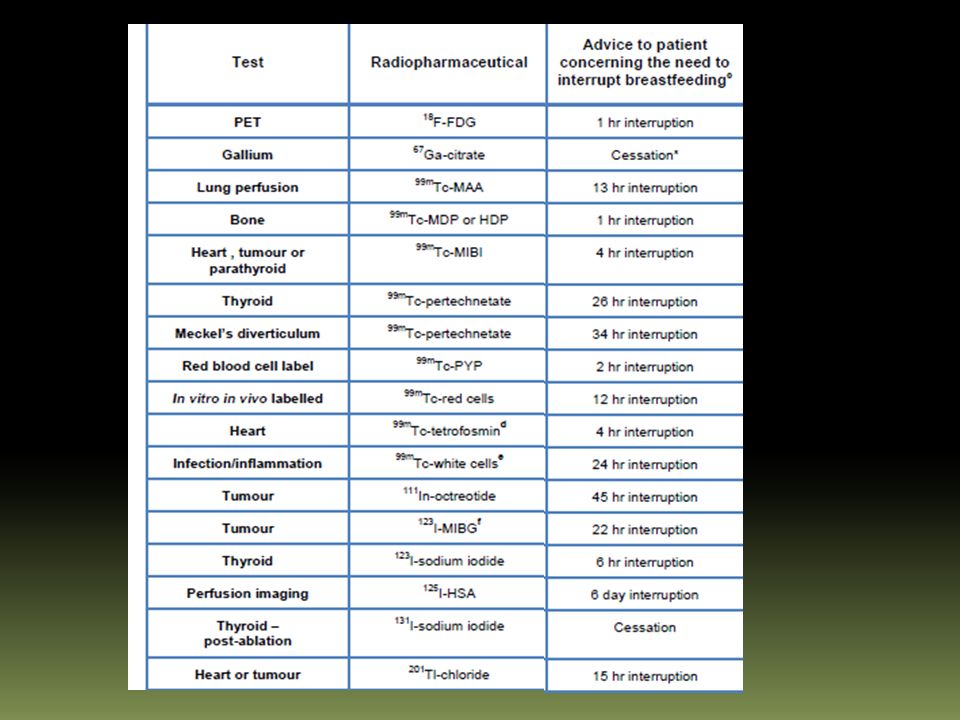
Fetal absorbed dose for nuclear medicine procedures
dose-can be modified external radiation from site placental transfer + fetal uptake maternal excretion eg bladder

17
Thyroid scanning with I131 and I123
Readily crosses placenta Preferentially taken up by fetal thyroid from 12 weeks Fetal thyroid dose mGy/mBq versus fetal whole body dose mGy/mBq prior to 12 weeks Significant risk of fetal thyroid damage

19
MAGNETIC RESONANCE IMAGING
Non-ionising, electromagnetic radiation 3 different forms: static magnetic field gradient magnetic field radiofrequency fields Potential for heat effect: postulated risk with >0.5° within fetus at vulnerable time eg 10 mins ultrasound in one spot not demonstrated with MRI

20
SOGC Clinical Practise Guideline 2014

21
Positron Emission Tomography (PET)
The absorbed dose to the pregnant model is less influenced by the gestation for most organs or tissues, but the anatomic changes of the maternal body increases the effective dose for some radiotracers. The absorbed dose is nonuniformly distributed in the fetus and would be 1.03–2 times higher in the fetal brain than in other fetal soft tissues. Have to add CT dose if co-registering

22
Three-dimensional visualization of computational pregnant female phantoms showing front views at early pregnancy, 3-mo pregnancy, 6-mo pregnancy, and 9-mo pregnancy. Uterine and placenta were set transparent in 3-, 6-, and 9-mo pregnant phantoms to exhibit fetus. Three-dimensional visualization of computational pregnant female phantoms showing front views at early pregnancy, 3-mo pregnancy, 6-mo pregnancy, and 9-mo pregnancy. Tianwu Xie, and Habib Zaidi J Nucl Med 2014;55: (c) Copyright 2014 SNMMI; all rights reserved
 Copyright 2014 SNMMI; all rights reserved.")
23
Fetal absorbed dose (A) and maternal effective dose (B)
18F-FDG, 18F-FDOPA, and 68Ga-DOTANOC for different pregnant phantoms. Fetal absorbed dose (A) and maternal effective dose (B) of 11C (realistic maximum model), 18F-FDG, 18F-FDOPA, and 68Ga-DOTANOC for different pregnant phantoms.
 and maternal effective dose (B) of 11C (realistic maximum model), 18F-FDG, 18F-FDOPA, and 68Ga-DOTANOC for different pregnant phantoms.")
24
Does fetal radiation cause
chromosomal damage? mental retardation? malignancy? epilepsy? miscarriage?

25
Event Background Risk Mental Retardation 0.5-1%
Congenital Malformation 3% Growth Retardation Miscarriage 15% Genetic disease 11% Lifetime risk of fatal cancer 23%

26
Heritable disease and radiation
”there is little to no evidence among the offspring of childhood, adolescent, and young adult cancer survivors; atomic bomb survivors; residentially-exposed populations; or radiation-exposed workers for an excess of cytogenetic syndromes, single-gene disorders, malformations, stillbirths, neonatal deaths, cancer, or cytogenetic markers that would indicate an excess of heritable genetic mutations in the exposed parents ” Brent RL 2014

27
Fetal radiation risk Related to the stage of pregnancy and absorbed dose Theoretically most significant during organogenesis and in the early fetal period, somewhat less in the 2nd trimester, and least in the 3rd trimester First 3 weeks post-conception, embryo relatively radiation resistant

28
Teratogenicity Threshold of 100-200 mGy or higher
Fetal doses of 100 mGy are not reached even with 3 pelvic CT scans or 20 conventional diagnostic x-ray examinations These levels can be reached with fluroscopically guided interventional procedures of the pelvis

29
Central nervous system effects
During 8-25 weeks post-conception the CNS is particularly sensitive to radiation Fetal doses > 100 mGy can result in some reduction of IQ (intelligence quotient) Fetal doses in the range of 1000 mGy can result in severe mental retardation and microcephaly, particularly during 8-15 weeks and to a lesser extent at weeks
 Fetal doses in the range of 1000 mGy can result in severe mental retardation and microcephaly, particularly during 8-15 weeks and to a lesser extent at weeks.")
30
Genetic Damage Excess risk of genetic disease estimated at % per 10 mGy exposure. No radiation induced transmissible gene mutations demonstrated in humans

31
IUGR Recent study of women exposed to dental Xrays during pregnancy Population based case-control study Exposure > than 0.4 mGy occurred in 10 term low- birth-weight pregnancies and was associated with an adjusted OR for a TLBW (<2.5kg) of 3.61 (95% CI, , P= .005). Hypothesis: risk related to maternal thyroid exposure but biologically not plausible and TFTs not measured JAMA 2004, 291:
 of 3.61 (95% CI, , P= .005). Hypothesis: risk related to maternal thyroid exposure but biologically not plausible and TFTs not measured. JAMA 2004, 291:")
32
Intrauterine Death No increase in miscarriage/stillbirth in Atomic bomb survivors or nuclear accidents No evidence that diagnostic radiation causes intrauterine death

33
Oncogenesis Epidemiological studies - variable results
Methodological problems- retrospectivity small study size case and control selection estimation of radiation dose outcome parameters Cohort v case-control studies

34
Oxford Survey of Childhood Cancer
Case-control Now includes >15,000 pairs Risk of leukaemia age < 10 : abdo radiation RR 1.92 [1.12, 3.28] no abdo radiation RR 1.19 [0.65, 2.16] Risk of all malignancies < age 10 abdo radiation RR 2.28 [1.31, 3.97] no abdo radiation RR 1.15 [0.68, 1.94]

35
Oncogenesis Meta-analysis of all case-control studies:
Relative risk may be as high as 1.4 (40% increase over normal incidence) with a fetal dose of 10 mGy OSCC suggests linear risk with no lower limit ERR 0.3 [0.1, 0.6] for 1 ‘film’ ERR 1.0 [0.5, 3.0] for 5 ‘films
 with a fetal dose of 10 mGy. OSCC suggests linear risk with no lower limit. ERR 0.3 [0.1, 0.6] for 1 ‘film’ ERR 1.0 [0.5, 3.0] for 5 ‘films.")
36
Oncogenesis For an individual exposed in utero to 10 mGy, the absolute risk of cancer at ages 0-15 is about 1 excess cancer death per 1,700 NOTE: the risk of leukemia is greater in “unirradiated” siblings of leukemics (1:720) than in patients subjected to diagnostic radiation (1:2,000)
 than in patients subjected to diagnostic radiation (1:2,000)")
37
Probability of bearing healthy children as a function of radiation dose
5 Higher Possible >100 99.1 97 100 99.4 50 99.6 10 99.7 1 Probability of no cancer (0-19 years) Probability of no malformation Dose to conceptus (mGy) above natural background
 Probability of no malformation. Dose to conceptus (mGy) above natural background.")
38
The impact of radiation dose on management of following conditions:
Diagnosis of pulmonary embolus Breast cancer Motor vehicle accident with suspected pelvic and sternal frcatures Flight from Paris to Tokyo Investigation for phaeochromocytoma

39
Investigation of suspected pulmonary embolus
In pregnancy, rate of non-diagnostic V⁄Q scans is lower (3–24%) than out of pregnancy and equivalent to the rate of non-diagnostic CTPA If other lung pathology suspected-CXR, CTPA Urgency-CTPA V/Q better resolution small PE
 than out of pregnancy and equivalent to the rate of non-diagnostic CTPA. If other lung pathology suspected-CXR, CTPA. Urgency-CTPA. V/Q better resolution small PE.")
40
Procedure Fetal Dose (mSv) Maternal Dose (mSv) CXR 0.001-0.01 <.01
V scan Q scan 1 Multislice CTPA T1 T3 20-60 Pulm angiography >0.5 5-30 Niemann T 2010 Insights Imag 1,6:361.

41
Maternal dose Latest data suggests even greater sensitivity of breast tissue than previously recognised Tissue weighting factor doubled with recent research

42
Postpartum CTPA preferred-do not need to discard breast milk
After V/Q: express and store breast milk for 12 hours

43
Breast cancer Diagnostic and Radiotherapy issues
Mammogram – undetectable Radiotherapy: 3.9 cGy for a 46 Gy total tumor dose. Need specific counselling about oncogenic risk

44
Management of trauma Local guidelines are important for ER
Eg Royal Melbourne Hosp Observational study N= 74 obstetric trauma patients Motor vehicle collisions (81%), assaults (8%), and falls (7%). 39% did not undergo imaging during their initial ER assessment Remaining 61% : plain x-rays were often used to avoid CT compliance rate with guidelines was only 18.8% ie only 6 patients had the recommended radiologic assessment
, assaults (8%), and falls (7%). 39% did not undergo imaging during their initial ER assessment. Remaining 61% : plain x-rays were often used to avoid CT. compliance rate with guidelines was only 18.8% ie only 6 patients had the recommended radiologic assessment.")
45
Need to calculate cumulative dose
Pelvic and chest xrays Around mGy Abdo CT 8 mGy Need to calculate cumulative dose Balance risk with benefit of detecting a ruptured spleen etc

46
Long distance flight <0.16 mSv Protracted Avoid solar flares!!
According to the National Oceanographic and Atmospheric Administration (NOAA), radiation dose from solar flares can reach as high as 200 µSv h-1 for up to a few hours at commercial aircraft altitudes. This would give a radiation dose of up to 400–600 µSv h-1 during a two-to-three-hour solar flare. Although this is a higher radiation dose than is normally experienced, such solar flares are expected to occur only a few times during the 11-year solar cycle and the great majority of passengers simply won't be in the air when one occurs. Even for those passengers who are exposed to this level of radiation, the expected effects still are not significant—this level of radiation exposure is similar to receiving an x ray and is far less than what you get in a computerized tomography scan.
, radiation dose from solar flares can reach as high as 200 µSv h-1 for up to a few hours at commercial aircraft altitudes. This would give a radiation dose of up to 400–600 µSv h-1 during a two-to-three-hour solar flare. Although this is a higher radiation dose than is normally experienced, such solar flares are expected to occur only a few times during the 11-year solar cycle and the great majority of passengers simply won t be in the air when one occurs. Even for those passengers who are exposed to this level of radiation, the expected effects still are not significant—this level of radiation exposure is similar to receiving an x ray and is far less than what you get in a computerized tomography scan.")
47
Investigation of Pheochromocytoma

48
Conclusions Medical exposures should be justified for each patient before they are performed (more benefit than risk) After it is decided to do a medical radiation procedure, the fetal radiation dose should be reduced while still obtaining the required diagnostic information eg alter procedure, shielding, dose monitoring

49
Informed consent The pregnant patient or worker has a right to know the magnitude and type of potential radiation effects that might result from in- utero exposure Communication should be related to the level of risk. Communication that risk is negligible is adequate for very low dose procedures (<1 mSv to the fetus) If fetal doses are above mSv, a more detailed explanation should be given
 If fetal doses are above 5-10 mSv, a more detailed explanation should be given.")
50
Summary Diagnostic imaging beyond the abdomen/pelvis generally safe
Risk of radiation at diagnostic levels is probably limited to an increase in childhood malignancy If Linear No Threshold is assumed - Excess absolute risk of cancer with pre-natal irradiation, 0.006% per mGy compared with a risk of % for a dose received just after birth NRPB

Similar presentations