Download presentation
Presentation is loading. Please wait.

1
Child abuse & Protection Child psychiatry 15 th dec 2015

2
Child Abuse This is defined as: deliberate infliction of harm to a child; or knowingly not preventing harm to a child. Children may be abused in the family home, in an institutional setting, or, rarely, by a stranger.

3
Most young people who are abused know their abuser. It is estimated that 1–2 children die each week due to abuse in the UK Child abuse may be categorized as: neglect; physical; sexual; emotional.

4
Neglect Is the persistent failure to meet a child's basic physical or psychological needs that is likely to result in serious impairment of the child's health and development. It may involve:

5
failing to provide adequate food; failing to protect from physical harm or danger; failure to access appropriate medical care or treatment.

6
Presentation: Failure to thrive. Consistently unkempt and dirty appearance. Repeated failure by carers to prevent accidental injury.

7
Physical Abuse Physical abuse involves any activity that causes physical harm to a child, e.g. hitting, shaking, burning, suffocating. Fabricated illness is also usually included in this category.

9
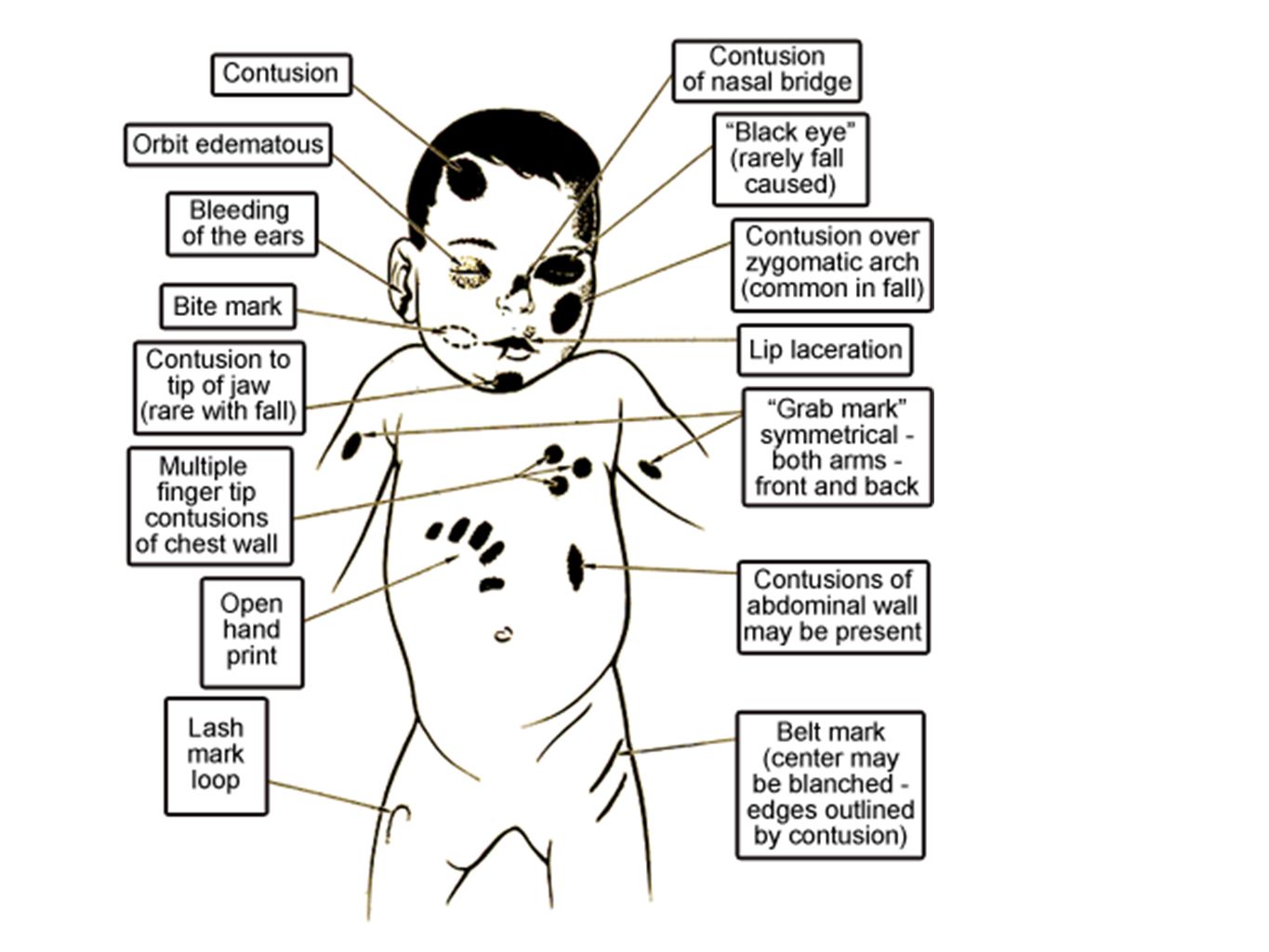
Typical presentations of physical abuse BRUISES: Symmetrical bruised eyes Bruising of soft tissues of the face, especially in small babies. Pre-mobile babies should not get bruises or other injuries Bruising of mouth or ears Finger marks on legs, arms, or chest (the latter may have associated rib fractures) Bruising of different ages Linear bruising on buttocks or back Distinct patterns of bruising, e.g. handprint marks, kicks Uncommon sites for accidents, e.g. stomach, chest, genitalia, neck
 Bruising of different ages Linear bruising on buttocks or back Distinct patterns of bruising, e.g. handprint marks, kicks Uncommon sites for accidents, e.g. stomach, chest, genitalia, neck.")
10
BURNS: Typically with clear outlines or small round burns, e.g. cigarette burns FRACTURES: It is rare for a child <1 year of age to sustain an accidental fracture. Bone disorders, e.g. osteogenesis imperfecta are rare. Consider the following:long bones (arms/legs); ribs. multiple fractures in various bones—almost always abuse BITE MARKS: Adult or child bite marks can be determined by forensic dentistry SCARS: Especially if concurrent bruising present
; ribs. multiple fractures in various bones—almost always abuse BITE MARKS: Adult or child bite marks can be determined by forensic dentistry SCARS: Especially if concurrent bruising present.")
11
POISINING: This may be accidental as a consequence of neglect, or deliberate (as in fabricated illness).
.")
12
Features that should arouse suspicion of P.A Repeated injury, no consistent explanation for how the injury occurred,patterns of injury, uncooperative hx, Inapprpriate child response( e.g. didn't cry), signs of other abuse, too young child to be consistent with the hx of injury. Unreasonable delay in presentation and parental aggression.
, signs of other abuse, too young child to be consistent with the hx of injury. Unreasonable delay in presentation and parental aggression..")
16
Investigations Skeletal survey and other imaging Infants do not localize pain; hence injuries of differing ages may be missed. X-rays must be carefully planned Alternatively, consider a radioisotope bone scan. X-rays: particularly in children aged <18 months and for some older children. Bone scan: if X-rays inconclusive. Useful for rib fractures

17
CT or MRI scan of brain: in infants and young children who present with irritability or coma. Clotting screening: Perform tests if extensive or unusual bruising, or unexplained cerebral haemorrhage. Ophthalmology examination by experienced ophthalmologist to look for evidence of retinal haemorrhages. The latter are suggestive of shaking injury.

18
Sexual Abuse This involves forcing or enticing a child or young person to take part in sexual activities whether or not the child is aware of what is happening. This may: -physical contact and penetrative or -non-penetrative acts. -non-contact activities such as looking at or being involved in pornography

19
Presentation of Sexual Abuse Children who have been victims of sexual abuse may present in a number of ways, including the following. STD: gonorrhoea; chlamydia; Trichomonas vaginalis. Pregnancy. Vaginal bleeding in prepubertal children. Behavioural changes: self-harm; withdrawal; aggression; sexualized behaviour; unexplained deteriorating school performance. Disclosure by the child. Secondary wetting and/or faecal soiling.

20
Signs of Sexual Abuse Few signs are diagnostic and there may be no findings in 50–90%. Acute signs Girls: tears in hymen; vaginal bleeding; bruising around genital area; and ‘hand’ grip marks. Boys: bruising to genital area; urethral injury; torn frenulum of penis. Anal signs: anal fissure; gaping anus; swelling of anal margin. Note: these signs may disappear rapidly.

21
Chronic signs These signs are more difficult to interpret. They include the following that may be suggestive of previous, repeated penetrative trauma: scar in posterior fourchette; old tear or scar of the hymen; attenuation of hymen (tissue rubbed or worn away).
..")
23
Emotional Abuse Persistent, emotional ill-treatment of a child that results in severe impairment in emotional development. This may involve conveying to children that they are worthless or unloved; imposing age or developmentally inappropriate expectations; causing children to frequently feel frightened and threatened. This form of abuse often coexists with other forms of ill treatment.

24
Presentations This is almost always gradual and difficult to diagnose. Symptoms are largely behavioural and may include: excessively clingy; attention- seeking behaviour;overly anxious; overly serious; anxious to please.

25
Parental behaviours are a clue to the diagnosis. Any of these must be persistent and severe and have a major impact on the child in order to reach the threshold for emotional abuse: persistently negative view of the child; inconsistent and unpredictable responses; expectations that are very inappropriate; induction of a child into bizarre parental beliefs.

26
Illnesses fabricated by Carers This is an unusual form of child abuse. It is also referred to as Munchausen syndrome by proxy (MSbP). The salient feature is that the child is harmed by being presented for medical attention with symptoms or signs that have been falsified by the carer.
. The salient feature is that the child is harmed by being presented for medical attention with symptoms or signs that have been falsified by the carer..")
27
The child is the victim of the abuse and the perpetrator is the person who fabricates the illness. Existing mental health difficulties in the perpetrator (child's natural mother in 90% of cases) have been described but are not essential for the diagnosis.
 have been described but are not essential for the diagnosis..")
28
Presentation There is a wide spectrum of severity of presentation of harm that includes: false medical story; fabrication of signs, e.g. blood on clothing, nappy or sugar in urine specimen. The most serious presentations include fabrication of illness induced by poisoning or suffocation.

29
Symptoms Children may present with one or more of a range of symptoms: seizures, collapse, coma apnoea vomiting and diarrhoea failure to thrive polyuria and polydipsia purpura recurrent fever

30
Risk factors for child abuse In the child: Disabled,wrong gender, forced and commercial sex Parent/Carer: Mental health, alcohol, drug abuse In the family:Step-parents,Domestic violence, young parental age Environment : poverty, poor housing

31
Medical involvement All health professionals have a role in ensuring that children and families receive the care, support, and services they need in order to promote child health and development. It is likely that health professionals will be the first to have contact with children or families in difficulty. Participation in child protection encompasses a range of activities.

32
Recognizing children in need of support or protection and parents who may need extra help in bringing up their children. Contributing to enquiries about a child or family. Assessing the needs of children and the capacity of parents to meet their children's needs.

33
Planning and providing support for vulnerable children and families. Participating in child protection conferences. Planning support for children at risk of significant harm. Providing therapeutic help to abused or neglected children and parents under stress. Contributing to case reviews.

34
Initial Concern Where there are concerns about a child, and when there is reasonable belief that a child is at serious risk of immediate harm, doctors should act immediately to protect the interests of the child, and this will almost always involve contacting one of the three statutory bodies with responsibilities in this area: social services; police; National Society for the Prevention of Cruelty to Children (NSPCC).
.")
35
A full report of concerns will be required. The precise action taken should be governed by the procedures set out by the local area child protection committee.

Similar presentations











; MA.>")









>")

