Download presentation
Presentation is loading. Please wait.

1
Red blood cell disorders.
By: Abiodun Mark Akanmode MD.

2
Erythropoiesis. This is the production of RBC from the bone marrow.
It is dependant on the release of EPO from the interstitial cells of the renal cortex. EPO is also produced ectopically in renal cell carcinoma and hepatorenal carcinoma. Stimuli for the release of EPO include: -hypoxemia(decreased arterial Po2) -severe anemia. -high altitude. -decreased O2 sat eg. Co poisoning. Increased O2 content suppresses EPO release eg. polycythemia.
 -severe anemia. -high altitude. -decreased O2 sat eg. Co poisoning. Increased O2 content suppresses EPO release eg. polycythemia.")
4
Reticulocytes. Retic cells or reticulocytes are newly released RBCs from he bone marrow. They are peripheral markers of effective erythropoesis. Retic cells are easily identified in a blood smear as threadlike RNA filaments can be seen in them on staining.

5
Reticulocyte count Absolute reticulocyte count: It’s just the straight-up percentage of red cells that are reticulocytes (normal is <3%). Using the absolute count can give a falsely elevated % in anemic pts. Corrected reticulocyte count: The corrected reticulocyte count = reticulocyte % x (actual Hct/45). Corrected retic count > 3% represents effective erythropoeisis ie good BM response to anemia. Corrected retic count < 3% indicates poor bone marrow response to anemia i.e. ineffective erythropoeisis.
. Corrected retic count > 3% represents effective erythropoeisis ie good BM response to anemia. Corrected retic count < 3% indicates poor bone marrow response to anemia i.e. ineffective erythropoeisis.")
6
Hematopoesis sites. In the fetus, blood production begins in the yolk sac and subsequently moves on to the liver and finally the bone marrow by the 5th-6th mth of gestation. Extramedullary hematopoesis refers to the production of blood cells outside the bone marrow. Common sites of EMH include the spleen & liver. Common causes include: -Intrinsic bone marrow disease. -Accelerated erythropoeisis.

7
Complete blood count components.
Hemoglobin, Hematocrit, RBC count. RBC indices, RBC distribution width. Wbc count, Differentials & Platelet count. Evaluation of peripheral blood smear morphology.

8
Red blood cell indices. Mean corpuscular volume (MCV): This refers to the average volume of RBCs. Frequently used to classify anemia: -Microcytic anemia: MCV <80. -Normocytic anemia: MCV Macrocytic anemia: MCV>100. Mean corpuscular hemoglobin concentration(MCHC):This refers to the mean HB concentration in RBCs. Decreased MCHC is seen in condition with decreased Hb synthesis e.g. microcytic anemias, here the rbc have decreased area of central pallor(hypochromasia) Increased MCHC is seen in conditions like hereditary spherocytocis, here rbc lack central pallor(hyperchromasia)
:This refers to the mean HB concentration in RBCs. Decreased MCHC is seen in condition with decreased Hb synthesis e.g. microcytic anemias, here the rbc have decreased area of central pallor(hypochromasia) Increased MCHC is seen in conditions like hereditary spherocytocis, here rbc lack central pallor(hyperchromasia)")
9
Red blood cell indices. Random blood cell distribution width(RDW):This measures variation in the sizes of peripheral RBCs. Size variation in RBC is called anisocytosis. Iron deficiency anemia is the most common microcytic anemia with an increased RDW.

10
Iron studies. Ferritin: soluble iron binding storage protein also helps to keep iron in its non toxic form. Its synthesized by the bone marrow macrophages and hepatocytes. Serum iron levels correlate with ferritin stores in the macrophages. Synthesis of ferritin increases during inflammation reaction due to the release of interleukin-6. Decreased serum ferritin in diagnostic of iron deficiency anemia. Hemosiderin is a breakdown product of ferritin.

11
Iron studies. Serum iron: The amount of circulating iron bound to transferrin. Transferrin are iron-binding blood plasma glycoproteins synthesized by the liver. Decreased serum iron is seen in iron deficiency anemia, While increased serum iron is seen in iron overload condition such as hemochromatosis.

12
Iron studies Serum Total Iron Binding Capacity(TIBC):This correlates with the concentration of transferrin. What is the relationship between ferritin stores, transferrin synthesis and and TIBC?

13
Hemoglobin electrophoresis.
This is used to detect hemoglobinopathies which includes: -Abnormalities in globin chain structure -Abnormalities in globin chain synthesis. Types of normal Hb: -HbA. -HbA2 -HbF. Types of abnormal Hb. -Sickle Hb. -HhB. -Hb Barts.

14
Anemia. This is defined as the reduced oxygen carrying capacity of blood. Laboratory findings: -Decreased Hb, Hct, Rbc conc sat and PO2 are normal. Anemia is a sign of an underlying disease not a diagnosis. Clinical features: -Fatigue, dyspnea with exertion, inability to concentrate and dizziness. -Pulmonary valve flow murmur. -Pallor of skin & conjunctiva.

15
Anemia. Microcytic anemia.
Types: -Thalassemia. -Iron deficiency anemia. -Chronic disease anemia/Anemia of chronic disease. -Sideroblastic anemia. All are associated with a defect in Hb Synthesis.

17
Iron deficiency anemia.
This is the most common nutritional disorder in the world. Iron deficiency can result from: -Dietary lack -Impaired absorption. -Increased requirement. -Chronic blood loss.

18
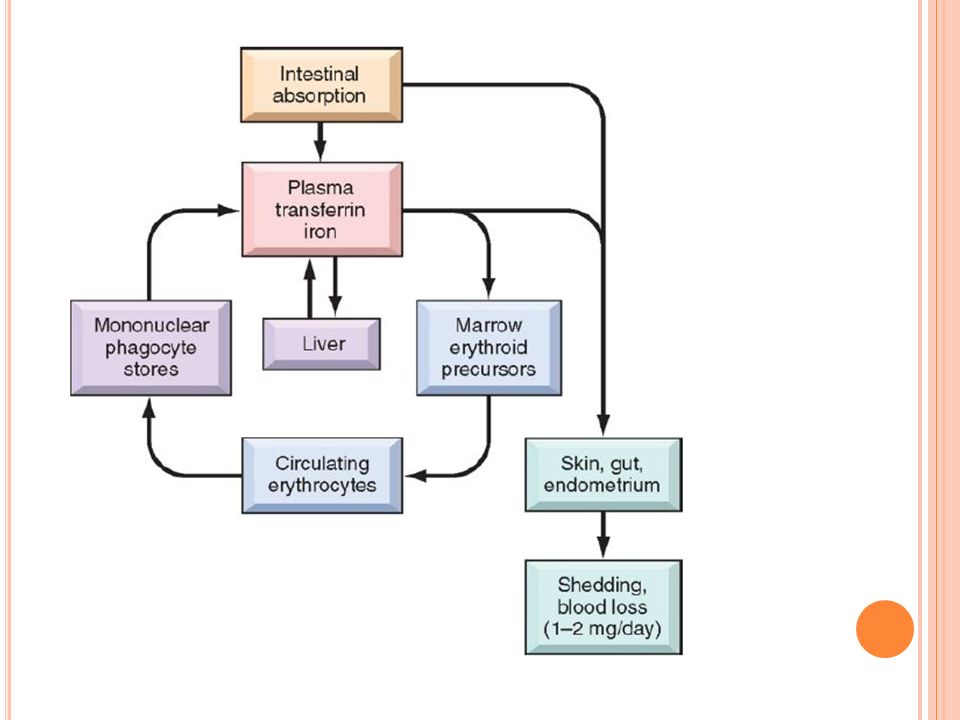
Iron balance Iron balance is highly maintained by regulating the absorption of dietary iron in the proximal duodenum. The normal daily western diet contains about 10-20mg of iron most of which is animal derived and the rest plant derived. Total body iron is about 2gm in females and about 6gms in males. 80% of all functional iron is found in hemoglobin, myoglobin and iron containing enzymes. Iron is both essential for cellular metabolism and its also highly toxic in excess.

21
Iron absorption regulation.
Hepcidin is a small circulating peptide that is synthesized by the liver. It is the master iron regulatory hormone and it determines whether iron is absorbed from the duodenum or whether iron is released from macrophages. Increased transferrin bound iron increased hepcidin synthesis down regulation of ferropotin 1accumulation of iron in enterocytes which is eventually shed into the bowel. Also reduced levels of ferropotin 1 causes iron blockage in the macrophages, so less iron is release for binding to transferrin and vice versa.

22
Clinical findings in iron deff anemia.
Chronic iron deficiency: -Esophageal webs: causes dysphagia to solid foods. -Achlorydia. -Glossitis & angular cheilosis. -Spoon shaped nails(koilonychia) Pallor of conjunctiva and palmer creases. Craving for Ice (pica)
 Pallor of conjunctiva and palmer creases. Craving for Ice (pica)")
24
Lab findings in iron deff anemia.
Decreased MCV. Decreased serum iron and iron saturation. Decreased serum ferritin. Increased TIBC and RDW.

25
Treatment for iron deff anemia.
Ferrous sulphate orally. Hct Should increase 0.5% to 1%/day. Lack of response indicates: -Noncompliance. -Continued blood loss. -Iron is not being absorbed.

26
Anemia of chronic diseases.
This is the most common variant of anemia in hospitalized patients. Common causes include: chronic alcoholism, malignancy and chronic inflammation. Pathogenesis a. Decreased heme synthesis. b. Decreased renal production and/or response to EPO c. Increased liver synthesis and release of hepcidin

27
Anemia of chronic diseases.
Lab findings in ACD: ↓iron, TIBC, %saturation; ↑ferritin. Treatment: a. Treat the underlying disease causing the inflammation. b. In some cases, giving EPO increases the Hb concentration. c. Hepcidin antagonists (recent treatment modality)
")
28
Thalassemia. These is a heterogeneous group of disorders caused by a mutation that ↓synthesis of α- or β-globin chains of the adult hemoglobin HbA. Heme synthesis is unaffected. Common among populations in Mediterranean, African, and Asian regions in which malaria is endemic

29
ß-Thalassemia Normal β-globin chain synthesis is designated β.
β0 mutations - no β-globin chains are produced β+ mutations - reduced (but detectable) β-globin synthesis
 β-globin synthesis.")
30
Clinical and Genetic Classification of Thalassemias

31
Mutations in ß-thalassemia
Mutations leading to aberrant RNA splicing most common no mature mRNA, complete failure of β-globin production (β0) New splice junctions in abnormal positions normal & abnormal splicing, some normal β-globin mRNA (β+) In β-globin promoter ↓transcription, some normal β-globin is synthesized (β+) “Stop” codons - No synthesis of β-globin (β0)
 New splice junctions in abnormal positions. normal & abnormal splicing, some normal β-globin mRNA (β+) In β-globin promoter. ↓transcription, some normal β-globin is synthesized (β+) Stop codons - No synthesis of β-globin (β0)")
32
Mechanisms of Anemia in ß-thalassemia
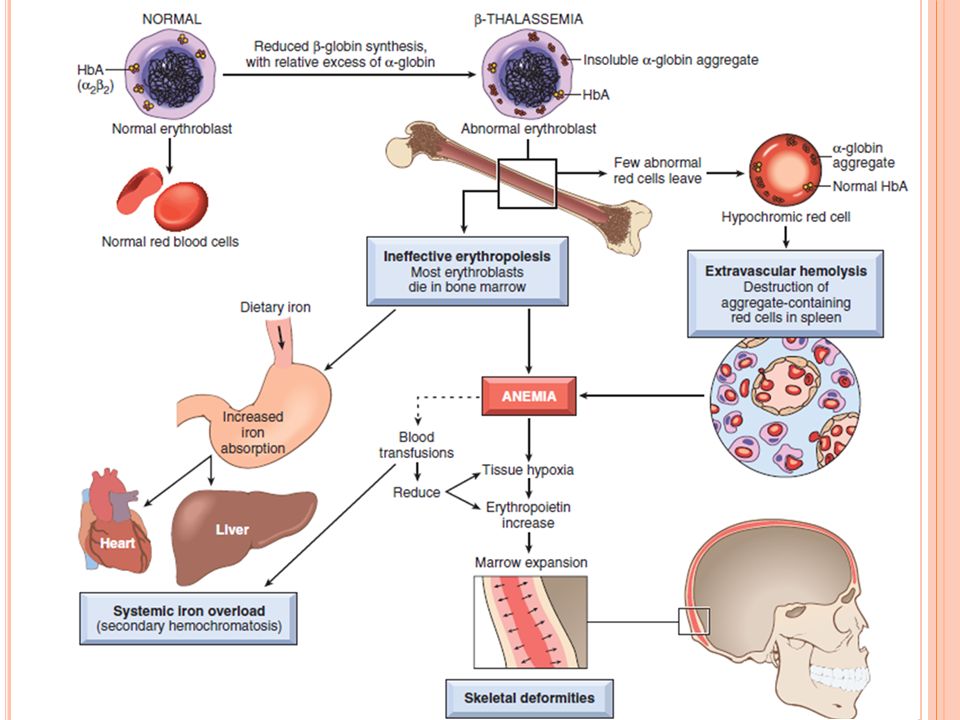
Reduced β-globin synthesis - ↓ HbA formation leads to poorly hemoglobinized red cells (HYPOCHROMIC MICROCYTIC ANEMIA) Excess of unpaired α chains form insoluble precipitates, that damage membranes of red cells and their precursors
 Excess of unpaired α chains form insoluble precipitates, that damage membranes of red cells and their precursors.")
33
Mechanisms of Anemia in ß-thalassemia
Damaged erythroid precursors die by apoptosis Ineffective Erythropoiesis (associated with increased absorption of dietary iron leading to iron overload) Shortened RBC life span due to extravascular hemolysis Relative Folate deficiency The increased iron absorption is caused by inappropriately low levels of hepcidin, which is a negative regulator of iron absorption
 Shortened RBC life span due to extravascular hemolysis. Relative Folate deficiency. The increased iron absorption is caused by inappropriately low levels of hepcidin, which is a negative regulator of iron absorption.")
34
Clinical Features INEFFECTIVE ERYTHROPOIESIS AND HEMOLYSIS
Expanded marrow fills intramedullary space & invades bony cortex - Impaired Bone Growth, Skeletal Deformities Extramedullary hematopoiesis & hyperplasia of mononuclear cells - Splenomegaly, Hepatomegaly, Lymphadenopathy Ineffective erythropoietic precursors consume nutrients - Growth Retardation and Cachexia Severe hemosiderosis

35
Thalassemia: X-ray film of the skull showing new bone formation on the outer table, producing perpendicular radiations resembling a “crewcut”

37
Morphology β-thalassemia major (Mediterranean Anemia / Cooley Anemia)
Peripheral blood smears show marked microcytosis, hypochromia, poikilocytosis (variation in cell size), and anisocytosis (variation in cell shape) Nucleated red cells (normoblasts) are also seen β-Thalassemia intermedia and HbH disease are associated with peripheral smear findings that lie between these two extremes
, and anisocytosis (variation in cell shape) Nucleated red cells (normoblasts) are also seen. β-Thalassemia intermedia and HbH disease are associated with peripheral smear findings that lie between these two extremes.")
38
Morphology β-thalassemia minor and α-thalassemia trait
Peripheral blood smears show small (microcytic) and pale (hypochromic) RBCs but regular in shape Target cells β-Thalassemia intermedia and HbH disease are associated with peripheral smear findings that lie between these two extremes
 and pale (hypochromic) RBCs but regular in shape. Target cells. β-Thalassemia intermedia and HbH disease are associated with peripheral smear findings that lie between these two extremes.")
39
Clinical Course β-Thalassemia major
Manifests post-natally (when HbF synthesis diminishes) Growth retardation begins in infancy Repeated blood transfusions make survival into 2nd/3rd decade possible, but lead to iron overload (secondary hemosiderosis) Treatment of choice: Bone marrow transplantation at early age. β-Thalassemia minor. often asymptomatic mild microcytic hypochromic anemia normal life expectancy Cardiac dysfunction from secondary hemochromatosis can be fatal (unless patients are treated aggressively with iron chelators)
 Growth retardation begins in infancy. Repeated blood transfusions make survival into 2nd/3rd decade possible, but lead to iron overload (secondary hemosiderosis) Treatment of choice: Bone marrow transplantation at early age. β-Thalassemia minor. often asymptomatic. mild microcytic hypochromic anemia. normal life expectancy. Cardiac dysfunction from secondary hemochromatosis can be fatal (unless patients are treated aggressively with iron chelators)")
40
-Thalassemia More common in South East Asians and Africans
Deletions involving one or more of the α-globin genes Severity of disease is proportional to missing α-globin genes Loss of a single α-globin gene SILENT CARRIER STATE, No anemia Deletion of all four α-globin genes - lethal in utero (HYDROPS FETALIS) HbH and Hb Bart have an abnormally high affinity for oxygen, which renders them ineffective at delivering oxygen to the tissues
 HbH and Hb Bart have an abnormally high affinity for oxygen, which renders them ineffective at delivering oxygen to the tissues.")
41
-Thalassemia trait 2 gene deletions
Hb and Hct are reduced but RBC count is normal to increased Asians: from a single chromosome (α/α −/−), children of these individuals are at higher risk of HbH disease or Hydrops Fetalis Blacks: one from each of the two chromosomes (α/− α/−) Symptomatic α-thalassemia is relatively common in Asian populations and rare in black African populations
, children of these individuals are at higher risk of HbH disease or Hydrops Fetalis. Blacks: one from each of the two chromosomes (α/− α/−) Symptomatic α-thalassemia is relatively common in Asian populations and rare in black African populations.")
42
-Thalassemia (HbH Disease)
Caused by loss of three α-globin genes . β4 tetramers (HbH) HbH has an abnormally high affinity for oxygen, which renders it ineffective at delivering oxygen to the tissues. Also prone to oxidation and forming intracellular inclusions
 HbH has an abnormally high affinity for oxygen, which renders it ineffective at delivering oxygen to the tissues. Also prone to oxidation and forming intracellular inclusions.")
43
-Thalassemia (HYDROPS FETALIS)
Deletion of all four α-globin genes - lethal in utero Hb Barts - excess γ-globin chains form tetramers (γ4) Incompatible with life, fetus shows severe pallor, generalized edema and massive hepatosplenomegaly (similar to HDN) Intrauterine transfusion may be lifesaving, Hematopoietic stem cell transplantation can be curative
 Incompatible with life, fetus shows severe pallor, generalized edema and massive hepatosplenomegaly (similar to HDN) Intrauterine transfusion may be lifesaving, Hematopoietic stem cell transplantation can be curative.")
44
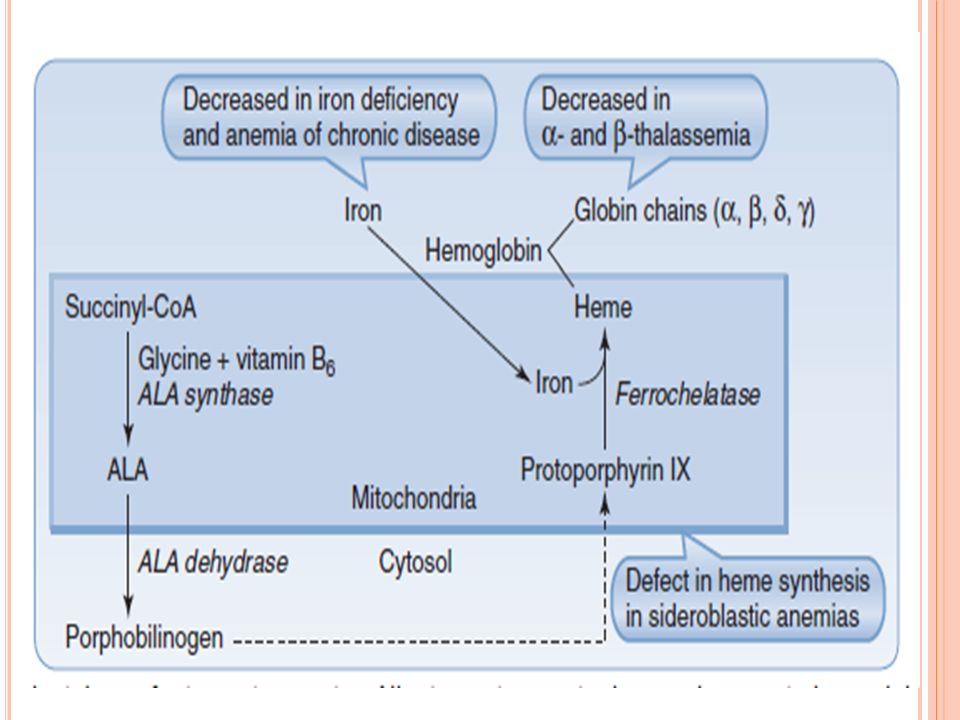
Sideroblastic anemia Epidemiology:
a. Chronic alcoholism (most common cause) b. Pyridoxine (vitamin B6) deficiency c. Lead (Pb) poisoning d. X-linked recessive (XR) disease. Pathogenesis: defect in heme synthesis within the mitochondria of developing RBCs in the bone marrow. Iron accumulates in mitochondria, which produces ringed sideroblasts.
 b. Pyridoxine (vitamin B6) deficiency. c. Lead (Pb) poisoning. d. X-linked recessive (XR) disease. Pathogenesis: defect in heme synthesis within the mitochondria of developing RBCs in the bone marrow. Iron accumulates in mitochondria, which produces ringed sideroblasts.")
45
Sideroblastic anemia Ringed sideroblasts in a bone marrow aspirate.
Dark blue iron granules around the nucleus of developing normoblasts (arrows) represent iron trapped within mitochondria and indicate a defect in mitochondrial heme synthesis (sideroblastic anemia).
 represent iron trapped within. mitochondria and indicate a defect in mitochondrial. heme synthesis (sideroblastic anemia).")
46
Laboratory findings a. Increased serum iron, iron saturation, and ferritin. b. Normal to decreased MCV and decreased TIBC. c. Ringed sideroblasts in a bone marrow aspirate

Similar presentations










. Complete Blood Count ( CBC)>")
 Hb is found in RBCs its main function is to transport O2 to tissues. Structure: 2 parts : heme + globin Globin: four globin chains (2 α.>")




 Hb is found in RBCs its main function is to transport O2 to tissues. Structure: 2 parts : heme + globin Globin: four chains. Heme: porphyrin.>")





