Download presentation
Presentation is loading. Please wait.

1
How Many ECG leads Dr. Zohair Alaseri, MD FRCPc, Emergency Medicine FRCPc, Critical Care Medicine Intensivest and Emergency Medicine Consultant Chairman, Department of Emergency Medicine King Saud University Medical City, Riyadh, KSA

2
How Many ECG leads A. A. 12 B. B. 15 C. C. 16 D. D. 18 E. E. 25

3
Introduction to 15 lead ECG Introduction to 15 lead ECG Anatomical Consideration Anatomical Consideration Rt Ventricular MI, diagnosis and challenges Rt Ventricular MI, diagnosis and challenges Posterior w. MI, diagnosis and challenges Posterior w. MI, diagnosis and challenges ECG Cases ECG Cases Summary Summary How Many ECG leads Interactive presentation to cover the following

4
12-lead ECG is a less-than perfect indicator of AMI The use of the additional leads provide a more accurate reflection of the true extent of myocardial damage. How Many ECG leads Am J Emerg Med 2003;21:563-573

5
How Many ECG leads Why we need 15 lead ECG? PMI &/or RVMI are very difficult to diagnose by the regular 12 lead ECG

6
Why acute posterior (PMI) and right ventricular (RV) myocardial infarctions are likely to be under diagnosed?? Because the standard lead placement of the 12-lead ECG does not allow these areas to be assessed directly How Many ECG leads

7
Prospective comparison of 12- and 15-lead ECGs 11.7% increase in sensitivity of AMI diagnosis by STE from 47.1% to 58.8% with the use of additional leads. Zalenski RJ, Cooke D, Rydman R, et al: Assessing the diagnostic value of an ECG containing leads V4R V8 and V9 the 15-lead ECG. Ann Emerg Med 1993;22:786-793 How Many ECG leads

8
RVMI STE is less pronounced than is usually seen in the standard 12-leads of the ECG. The right ventricle is composed of considerably less muscle when compared with the left ventricle How Many ECG leads Why??

9
Posterior MI ST- Elevation is less pronounced than is typically seen Relative distance of the posterior leads from the posterior wall of the LV How Many ECG leads Why??

10
(RV) is directly imaged only by V4R and, to a lesser extent, standard precordial lead V1. posterior leads directly image the posterior wall of the LV V1 to V6 indirectly view the posterior wall of the LV

11
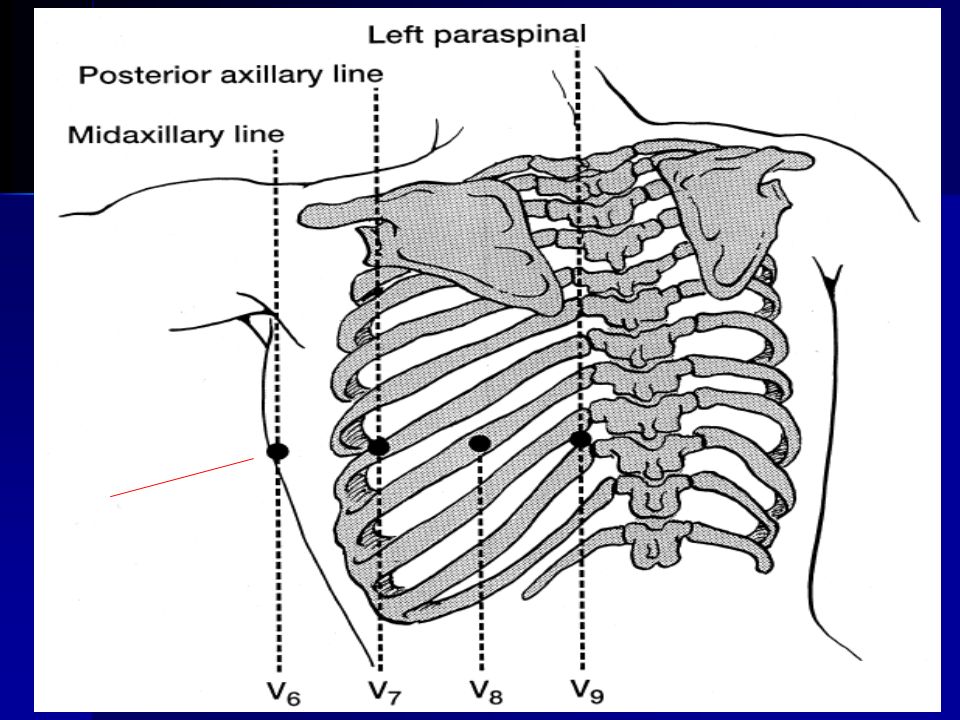
lead RV4 lead V8 lead V9

13
V1R is same as standard V2, V2R is the same as standard V1, V3R is halfway between V2R V4R, V4R is fifth intercostals space at right midclavicular line, V5R is same level as V4R in right anterior axillary line V6R is same level in right midaxillary line

14
How Many ECG leads leads V8 and V9 V4R reflects the status of the right ventricle. image the posterior wall of the left ventricle Additional leads

15
Isolated RV infarction is a rare Most RV infarctions result from occlusion of the Rt coronary artery proximal to the Rt ventricular branch. The left circumflex artery supplies the RV in approximately 10% of patients. RV infarction will present in the setting of a lateral wall AMI. RV AMI How Many ECG leads

16
Electrocardiographic studies have consistently shown that RV infarction occurs in approximately one-third of IMIs Zeymer U, Heuhaus KL, Wegscheider K, et al: Effects of fibrinolytic therapy in acute myocardial infarction with or without right ventricular involvement. J Am Coll Cardiol 1998;32:876-881 Braat SJ, Brugada P, DeZwaam C, et al: Value of the electrocardiogramin iagnosing right ventricular involvement in patientswith acute inferior wall myocardial infarction. Br Heart J 1983;49: 368-372 Klein HO, Tordjman T, Ninio R, et al: The early recognition ofright ventricular infarction: diagnostic accuracy of the electrocardiographic V4R lead. Circulation 1983;67:558-565 RV AMI Its relation with the inferior mi

17
STE in lead V4R is represented by a rightward and anteriorly oriented vector. So leftward ST-segment deviation, as is seen in leads V5 and V6 during a lateral AMI, could cancel the right-lead STE and obscure the diagnosis. Additionally, if STE is not prominent in the inferior leads, then it will be less prominent in V4R. Challenges RV AMI

18
Challenges Coexisting AMI of the left ventricle’s posterior wall can obscure the STE resulting from RV infarction in lead V1 as seen in patients with the acute inferoposterior MI with RV involvement RV AMI

19
RV infarction can be diagnosed with 80% to 100% sensitivity by STE greater than 1 mm in lead V4R Braat SJ Value of the electrocardiogramin iagnosing right ventricular involvement in patients with acute inferior wall myocardial infarction. Br Heart J 1983;49: 368-372 Klein HO The early recognition of right ventricular infarction: diagnostic accuracy of the electrocardiographic V4R lead. Circulation 1983;67:558-565 RV AMI

20
Robalino BD, Whitlow PL, Underwood DA, et al: Electrocardiographic manifestations of right ventricular infarction. Am Heart J 1989;118:138-144 STE greater than 1 mm in V4R has 100% sensitivity 87% specificity 92%predictive accuracy in detecting acute RV MI. RV AMI

21
ST-segment elevation inferior leads ST- elevation in the rt precordial chest leads, particularly V1 STE is greatest in lead III compared with the other inferior leads RBBB second- and third-degree AV blocks STE in lead V2 greater than 50% the magnitude of ST- depression (STD) in lead aVF 12-lead ECG are suggestive RV AMI
 in lead aVF 12-lead ECG are suggestive RV AMI")
22
The term posterior myocardial infarction (PMI) refers to AMI of the posterior wall of the left ventricle. Posterior MI

23
V7, posterior axillary line; V8, posterior scapular line; V9, left border of spine. Posterior Leads All in the same horizontal plane of V4 to V6

24
Usually occur in conjunction with inferior or lateral AMIs and are estimated to occur in 15% to 21% of all infarctions Posterior MI

25
(1) horizontal STD; (2) a tall, upright T wave; (3) a tall, wide R wave (4) an R/S wave ratio greater than 1.0. (5) Inferior or lateral walls MI Posterior MI PMI can be suspected if 12 ecg showes on of the following changes primarily in leads V1 and V2, V3:
 Inferior or lateral walls MI Posterior MI PMI can be suspected if 12 ecg showes on of the following changes primarily in leads V1 and V2, V3:.")
26
STE greater than 1 mm in leads V8 and V9 confirms the diagnosis of PMI Posterior MI

27
Adjusting the ischemic threshold from 1 to 0.5 mm of STE in leads V7 to V9 improved sensitivity for diagnosing PMI from 49% with the 12-lead ECG to 94% with the 15-lead ECG Wung S, Drew B: New electrocardiographic criteria for posteriorwall acute myocardial ischemia validated by a percutaneoustransluminal coronary angioplasty model of acute myocardial infarction. Am J Cardiol 2001;87:970- 974 Posterior MI

28
Khaw K, Improved detection of posterior myocardial wallischemia with the 15-lead electrocardiogram. Am Heart J 1999;138(5 Pt 1):934 – 40. There are reports of ST elevation in posterior leads in the absence of changes in anterior leads Posterior MI
:934 – 40. There are reports of ST elevation in posterior leads in the absence of changes in anterior leads Posterior MI.")
29
A prospective ECG analysis during angioplasty for single- vessel disease involving LCX or RCA found that ST segment elevation in leads II, aVF, and III is the most common ECG change during RCA occlusion (95%). Posterior ST elevation in leads V7 to V9 (68%) is the most common change during LCX occlusion. Kulkarni AU, Brown R, Ayoubi M, et al. Clinical use of posterior electrocardiographic leads: a prospective electrocardiographic analysis during coronary occlusion. Am Heart J 1996;131(4):736 – 41. 15 Leads ECG
 is the most common change during LCX occlusion. Kulkarni AU, Brown R, Ayoubi M, et al. Clinical use of posterior electrocardiographic leads: a prospective electrocardiographic analysis during coronary occlusion. Am Heart J 1996;131(4):736 – Leads ECG.")
30
ST-segment elevation in leads V8 and V9 minimal ST-segment depression with large R waves in V1 to V3 confirming (posterior wall AMI)
")
31
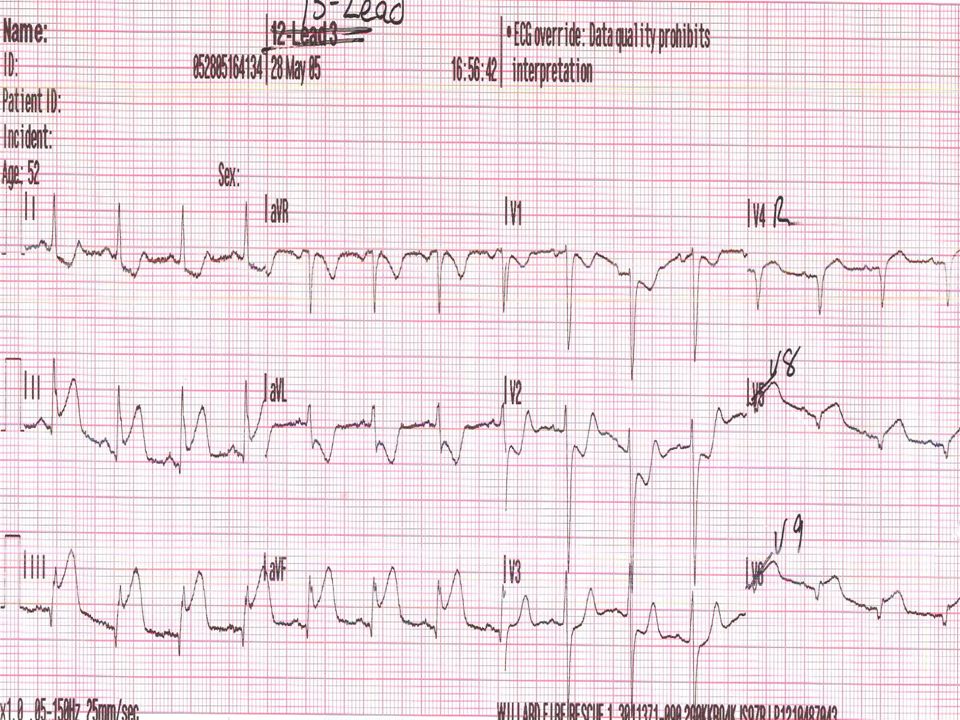
ST-segment elevation in leads II, III, and AVF, leads V8 and V9 and lead V4R consistent with an inferoposterior AMI with RV MI.

32
ST-elevation in the inferior leads & leads V1 and V4R Minimal ST- elevation in leads V8 and V9 suggestive of early posterior wall AMI. The lack of appropriate findings in leads V1 to V3 suggestive of a posterior wall AMI is explained by the presence of RVMI and related ST-elevation in the Rt precordial leads.

34
Posterior MI with reciprocal depression in V1-V3

35
a 15-lead ECG recorded before balloon occlusion in a 68-year-old male patient without a history of prior MI.

36
15-lead ECG during occlusion of a nondominant LC at the proximal site. No significant DST deviation of >1 mm was observed in the standard ECG. Isolated posterior DST elevation of 0.7 mm or 70 mV was present in V7 & V8.

37
70 y o woman presented to the ED by ambulance after being found to be unresponsive in the bathroom by her family. ST-segment depression in V1 through V4 and ST-segment elevation in isolated lead V6.

38
1-mm ST-segment elevation in leads V7 and V8, and 1.5-mm ST-segment elevation in lead V9

39
ST elevation is present in II, III, aVF, and V1; reciprocal ST depression in all other leads Acute right ventricular MI.

40
Usefulness of Three Posterior Chest Leads for the Detection of Posterior Wall Acute Myocardial Infarction Aqel RA - Am J Cardiol - 15-JAN-2009; 103(2): 159-64 A 15-lead electrocardiogram in response to LC occlusion. ST-segment elevation is evident in the posterior leads (V7 to V9) despite no significant ST elevation in the standard 12 leads.
 despite no significant ST elevation in the standard 12 leads..")
41
(A)ECG at baseline and (B)(B)during fully occlusive balloon inflation in the proximal LC artery
ECG at baseline and (B)(B)during fully occlusive balloon inflation in the proximal LC artery")
42
A 68-year-old man presented with chest pain radiating to the left arm of 3 hours ’ duration. He was diaphoretic and pale. ST-segment depression, prominent R wave, and upright T waves in leads V1 to V3 in addition, ST-segment depression was seen in the inferior and lateral leads

43
A 68-year-old man presented with chest pain radiating to the left arm of 3 hours ’ duration. He was diaphoretic and pale.

44
A 56-year-old man, history of HTN developed epigastric pain while working. pale, diaphoretic with a BP of 70 mm/Hg. ST-segment elevation ST-segment depression, prominent R wave

45
RV and Posterior MI A 56-year-old man, history of HTN developed epigastric pain while working. pale, diaphoretic with a BP of 70 mm/Hg.

46
ST-segment elevation in leads II, III, and AVF, leads V8 and V9 and lead V4R consistent with an inferoposterior AMI with RV MI.

47
15 lead ECG showing Right Ventricular MI and Posterior (recip in V1-V4)
")
48
Inferior STE & reciprocal STD STE in lead V1 is typical for RV AMI widespread STE Inferior & RV MI

49
(1) STD or suspicious isoelectric ST-segments in leads V1 – V3 (2) borderline STE in leads V5 and V6 or in leads II, III, and aVF (3) all STE inferior AMIs (STE in leads II, III, and aVF) (4) STE in leads V1 and V2 or isolated STE in lead V1. The established specific indications for using 15-lead ECGs include the following:

50
RV infarction RBBB second- and third-degree AV blocks, STE in lead V2 less than 50% the magnitude of STD in aVF. Inferior AMI presenting with hypotension The established specific indications for using 15-lead ECGs include the following:

51
Thank You

Similar presentations













>")





