Download presentation
Presentation is loading. Please wait.

1
Dialysis In Kidney Disease
Carmody Sagers Anna Johnson Anna Willis Lamli Lam

2
Review of Kidney Function
Kidney is responsible for: Filtering blood Maintaining balance of fluid, electrolytes, solutes Secreting renin to control blood pressure Producing erythropoietin Producing active form of vitamin D Eliminating calcium and phosphorus Cells of glomerulus secrete renin, which acts on angiotenisongen in the lungs EPO is a crrtical determinant of erythroid activity in the bone marrow. Hormone that stimulates production of RBCs

3
So what happens in kidney failure?
High level of circulating waste products (azotemia) Decreased Glomerular Filtration Rate (GFR) Shift in fluid and electrolyte balance Cessation of production of hormones
 Decreased Glomerular Filtration Rate (GFR) Shift in fluid and electrolyte balance. Cessation of production of hormones.")
4
Severe anemia due to lack of EPO
These things lead to… Uremia Malaise Weakness Nausea and vomiting Muscle cramps and itching Neurological impairment Edema Renal osteodystrophy Severe anemia due to lack of EPO Uremia is a clinical syndrome of…the above symptoms. Caused by the high level of circulating waste products. Get edema because of the retention of sodium Renal osteodystrophy is a group of metabolic bone diseases.

5
Treatment for Renal Failure
Two options: Dialysis The process of diffusing blood through a semipermeable membrane for the purpose of removing toxic materials and maintaining the acid-base balance Two kinds: hemodialysis & peritoneal dialysis Kidney Transplant

6
Uremia BUN >100 mg/dl Creatinine 10-12 mg/dl Diagnosis
Chart from

7
As of 2008 Prevalence 547,982 U.S. residents had ESRD
205,724 of the cases resulted from diabetes 382,343 U.S. residents were receiving dialysis treatments

8
Cardiovascular Disease Congestive Heart Failure Lung disease
Comorbidities Diabetes High Blood Pressure Cardiovascular Disease Congestive Heart Failure Lung disease Peripheral Vascular Disease Malnutrition Diabetes is the number one cause of kidney failure HBP, second leading cause.

10
Normal Ca/P Metabolism
Maintenance of calcium-phosphorus homeostasis is an important and complex process Involves the interactions of parathyroid hormone (PTH), calcitonin, and active vitamin D The three main organs involved are the gut, kidney, and bone
, calcitonin, and active vitamin D. The three main organs involved are the gut, kidney, and bone.")
11
Normal Ca/P Metabolism
The kidney produces the active form of vitamin D and eliminates both calcium and phosphorus Active vitamin D promotes absorption of Ca by the gut and is needed for bone remodeling Vit D also suppresses PTH production, which is responsible for mobilizing Ca from bone

12
Normal Ca/P Metabolism
Chart from

13
Results in hyperparathyroidism, phosphate retention, and hypocalcemia
Ca/P Metabolism in CKD As GFR decreases, phosphorus is retained in the plasma and serum Ca levels decline Kidneys have a decreased ability to produce vitamin D decreased gut absorption of calcium reliance on PTH to main Ca levels through bone resorption Results in hyperparathyroidism, phosphate retention, and hypocalcemia In the diet, calcium intake must be kept high and phosphorus intake must be kept low P remains because its levels are controlled by renal excretion. Thus, when the GFR decreases more is retained Ca declines because less vit D is being produced which means less gut absorption In a healthy body, low Ca levels trigger the release of PTH and increased synthesis of vitamin D by the kidney.

14
Ca/P Metabolism in CKD Bone disease
Dependence of ca-p control on increasing levels of PTH leads to a characteristic hyperplastic demineralized bone disease called Osteitis fibrosa cystica.

15
Ca/P Metabolism in CKD FGF = fibroblasts growth factor 23.

16
Dialysis

17
What is the purpose of dialysis?
Removes waste from the blood Removes excess water from the blood Helps control blood pressure Helps balance K, Na, Ca, and HCO3 This depends on the electrolyte concentration in the dialysate Does not correct the endocrine functions of the kidney

18
Properties of solutions

19
How does dialysis work? The dialysis membrane, keeps the blood separate from the dialysis fluid. A thin layer of natural tissue (in PD) A synthetic plastic (in HD) Dialysis fluid or dialysate is a plasma-like fluid where waste and excess water go when they leave the blood These processes are called diffusion and osmosis. blood cells are too large to pass through the membrane
 Dialysis fluid or dialysate is a plasma-like fluid where waste and excess water go when they leave the blood. These processes are called diffusion and osmosis. blood cells are too large to pass through the membrane.")
20
How does dialysis work? (cont)
Excess fluid is removed from the blood through ultrafiltration. In HD, the fluid is simply drawn from the blood by the dialysis machine. The amount of water to be removed can be varied by changing the dialyzer’s settings. In PD dextrose is added to the dialysate to draw water out by osmosis. Solution containing a lot of dextrose will draw out more fluid than a weaker solution.

21
Hemodialysis vs. Peritoneal
Hemodialysis-through dialysis needles and tubing connected to your arm blood is pumped through a dialyzer (artificial kidney) that cleans the waste products from your blood then returns it to your body Peritoneal dialysis- through a catheter dialysate is pumped into the peritoneal cavity, waste products diffuse from the blood into the dialysate. This fluid is withdrawn and discarded and new solution is added.
 that cleans the waste products from your blood then returns it to your body. Peritoneal dialysis- through a catheter dialysate is pumped into the peritoneal cavity, waste products diffuse from the blood into the dialysate. This fluid is withdrawn and discarded and new solution is added.")
22
200 ml of blood goes through the machine at a time
Hemodialysis External artificial kidney (hemodialyzer) connected to a dialysis machine 200 ml of blood goes through the machine at a time Treatment 3x/week. Each treatment lasts from 3-5+ h Home dialysis treatments can be daily for h or nocturnally 3x/week for 8 h Surgery is necessary to create access to the bloodstream While you get treatment you can read, watch tv Europeans and dialysis
 connected to a dialysis machine. 200 ml of blood goes through the machine at a time. Treatment 3x/week. Each treatment lasts from 3-5+ h. Home dialysis treatments can be daily for h or nocturnally 3x/week for 8 h. Surgery is necessary to create access to the bloodstream. While you get treatment you can read, watch tv. Europeans and dialysis.")
23
Dialyzer The first successful dialyzer was made in 1945

25
Fistula- artery and vein are connected
Access to bloodstream Fistula- artery and vein are connected Looped graft- artificial vessel is inserted If patient’s blood vessels are too fragile Catheter- used until patient’s permanent access can be created or matured (can take several months) usually short term Artery and vein are connected to increase blood flow and size of vessel to accommodate increased injections
 usually short term. Artery and vein are connected to increase blood flow and size of vessel to accommodate increased injections.")
26
Access points for hemodialysis

27
Fistulas enlarged vein (usually in your arm)
created by connecting an artery directly to a vein, allows greater blood flow into the vein As a result, the vein enlarges and strengthens, making the insertion of needles for hemodialysis treatments easier. Aneurysm- localized dilation of a blood vessel Anastomosis- surgical connection between two structures

28
DaVita clinics

29
Types of Peritoneal Dialysis (PD)
Continuous Ambulatory PD (CAPD) Requires no machine Dwell time of 4-6h, 4-5x daily, 24h treatment Process of draining and refilling takes about minutes Continuous Cyclical PD (CCPD) or Automated PD (APD) machine called a cycler to fill and empty your abdomen three to five times during the night while you sleep. In the morning, you begin one exchange that lasts the entire day. You may do an additional exchange in the middle of the afternoon without the cycler to increase the amount of waste removed and to reduce the amount of fluid left behind in your body. Combo- may be chosen if you weigh over 175 lbs or if your peritoneum drains very slowly. Dwell time is how long the dialysate stays in your peritoneum.
 Requires no machine. Dwell time of 4-6h, 4-5x daily, 24h treatment. Process of draining and refilling takes about minutes. Continuous Cyclical PD (CCPD) or Automated PD (APD) machine called a cycler to fill and empty your abdomen three to five times during the night while you sleep. In the morning, you begin one exchange that lasts the entire day. You may do an additional exchange in the middle of the afternoon without the cycler to increase the amount of waste removed and to reduce the amount of fluid left behind in your body. Combo- may be chosen if you weigh over 175 lbs or if your peritoneum drains very slowly. Dwell time is how long the dialysate stays in your peritoneum.")
30
Peritoneal Dialysis

31
CAPD Exchange

32
Peritoneal Equilibration Test
Used solution is collected from one exchange to a 24h period to see the effectiveness of a dose of PD. This solution is compared to blood and urine samples from the same time period The peritoneal transport rate varies from person to person Used to see how effective the current PD schedule is in clearing the blood of urea. From all the samples, one can compute a urea clearance and a creatinine clearance rate-normalized to body surface area. The residual clearance of the kidneys is also considered. Based on these measurements, one can determine whether the PD dose is adequate. . People who have a high rate of transport absorb dextrose from the dialysis solution quickly, and they should be given a dialysis schedule that avoids exchanges with a long dwell time because they tend to absorb too much dextrose and dialysis solution from such exchanges.

33
Peritoneal Equilibration Test (cont)
If the laboratory results show that the dialysis schedule is not removing enough urea and creatinine, the doctor may change the prescription by increasing the number of exchanges per day for patients treated with CAPD or per night for patients treated with CCPD increasing the volume-amount of solution in the bag-of each exchange in CAPD adding an extra, automated middle-of-the-night exchange to the CAPD schedule adding an extra middle-of-the-day exchange to the CCPD schedule using a dialysis solution with a higher dextrose concentration

34
Choosing the right treatment
Evaluate which treatment would work best with your lifestyle There are pros and cons for each type Patients can talk with their physician about combining treatments Some people use PD every day, but get HD once a week if PD treatments are not removing enough waste from the blood

35
Pros and Cons of In-Center HD
Facilities are widely available. Trained professionals are with you at all times. You can get to know other patients. You don't have to have a partner or keep equipment in your home. Cons Treatments are scheduled by the center and are relatively fixed. You must travel to the center for treatment. This treatment has the strictest diet and fluid limits of all. You will need to take-and pay for-more medications. You may have more frequent ups and downs in how you feel from day to day. It may take a few hours to feel better after a treatment.

36
Pros Cons Pros and Cons of Home HD
You can do it at the times you choose-but you still must do it as often as your doctor orders. You don't have to travel to a center, more friendly for work and travel You gain a sense of independence and control over your treatment. Newer machines require less space and are portable. You will have fewer ups and downs in how you feel from day to day. Your diet and fluids will be much closer to normal You can spend more time with your loved ones. You must have a partner, who is also trained. Helping with treatments may be stressful to your family. You need space for storing the machine and supplies at home. You will need to learn to put in the dialysis needles. Daily and nocturnal home hemodialysis are not yet offered in all locations.

37
Advantages Disadvantages Pros and Cons of PD
Fit your treatment around your lifestyle Independence – mostly you perform the treatment yourself Fewer visits to the dialysis unit (usually once a month) Works during sleep time for some people Continuous therapy is gentler and more like your natural kidney function Portable and flexible – easy to take your treatment with you when you travel Less fluid and diet restrictions No needles Better blood pressure control You need to be well trained Permanent catheter access required Some risk of infection May show a slightly larger waistline (due to carrying fluid) Storage space required in your home Possible changes in your appearance due to medications side effects
 Works during sleep time for some people. Continuous therapy is gentler and more like your natural kidney function. Portable and flexible – easy to take your treatment with you when you travel. Less fluid and diet restrictions. No needles. Better blood pressure control. You need to be well trained. Permanent catheter access required. Some risk of infection. May show a slightly larger waistline (due to carrying fluid) Storage space required in your home. Possible changes in your appearance due to medications side effects.")
38
CAPD & CCPD CLINIC HD HOME HD Can I do dialysis at home? YES NO Can I still work or attend school full-time? NOT ALWAYS Can I still travel? POSSIBLY Do I need to have needles inserted every time? Will it make me tired? Can I arrange my dialysis at convenient times? Do I need to have equipment/supplies at home?

39
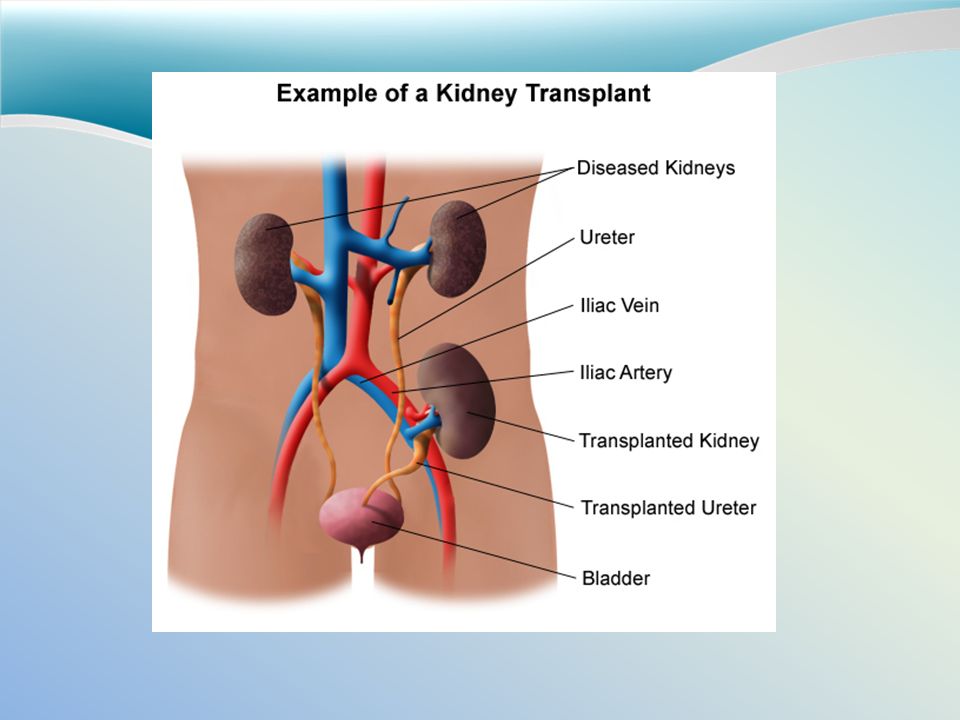
Kidney Transplantation
Hemodialysis Peritoneal Dialysis Kidney Transplantation In Center Home CAPD CCPD Deceased Living Schedule Three treatments a week for 3 to 5 hours or more. More flexibility in determining your schedule of treatments. Four to six exchanges a day, every day. Three to five exchanges a night, every night, with an additional exchange begun first thing in the morning. You may wait several years before a suitable kidney is available. If a friend or family member is donating, you can schedule the operation when you're both ready. After the operation, you'll have regular checkups with your doctor. Location Dialysis center. Home. Any clean environment that allows solution exchanges. The transplant operation takes place in a hospital. Availability Available in most communities; may require travel in some rural areas. Generally available, but not widely used because of equipment requirements. Widely available. Transplant centers are located throughout the country. However, the demand for kidneys is far greater than the supply. Equipment and Supplies No equipment or supplies in the home. Hemodialysis machine connected to plumbing; chair. Bags of dialysis solution take up storage space. Cycling machine; bags of dialysis solution. No equipment or supplies needed. Training Required Little training required; clinic staff perform most tasks. You and a helper must attend several training sessions. You'll need to attend several training sessions. You'll need to learn about your medications and when to take them. Diet Must limit fluids, sodium, potassium, and phosphorus. Must limit sodium and calories. Fewer dietary restrictions. Level of Freedom Little freedom during treatments. Greater freedom on nontreatment days. More freedom to set your own schedule. You're still linked to a machine for several hours a week. You can move around, exercise, work, drive, etc., with solution in your abdomen. You're linked to a machine during the night. You're free from exchanges during the day. Offers the greatest amount of freedom. Level of Responsibility Some patients prefer to let clinic staff perform all tasks. You and your helper are responsible for cleaning and setting up equipment and monitoring vital signs. Can be stressful on family helpers. You must perform exchanges four to six times a day, every day. You must set up your cycler every night. You must take immunosuppressants every day for as long as the transplanted kidney functions.

40
Risk factors associated
Peritonitis is still a common problem that sometimes makes continuing PD impossible. Here are some general rules: Store supplies in a cool, clean, dry place. Inspect each bag of solution for signs of contamination before you use it. Find a clean, dry, well-lit space to perform your exchanges. Wash your hands every time you need to handle your catheter. Clean the exit site with antiseptic every day. Wear a surgical mask when performing exchanges. Here are some signs to watch for: Fever Nausea or vomiting Redness or pain around the catheter Unusual color or cloudiness in used dialysis solution A catheter cuff that has been pushed out

41
Dialysis is very expensive
Cost of dialysis Dialysis is very expensive The federal government (Medicare and Medicaid) will pay 80% of the cost Private health insurance or state medical aid also help with the costs $500 a treatment
 will pay 80% of the cost. Private health insurance or state medical aid also help with the costs. $500 a treatment.")
42
Dialysis and Lifestyle
We do not yet know how long patients on dialysis will live. We think that some dialysis patients may live as long as people without kidney failure. Many patients live normal lives except for the time needed for treatments. Dialysis centers are located in every part of the United States and in many foreign countries. The treatment is standardized. Many dialysis patients can go back to work Jobs that require lots of physical labor may be too strenuous

43
It increases a patient’s risk of hospitalization and death
Compliance At least ½ of hemodialysis patients are noncompliant and 1/3 of PD patients are as well It increases a patient’s risk of hospitalization and death The reasons most linked to noncompliance are psychosocial issues, younger age and smoking Treatment regimen can be modified to increase compliance They just want to have control in their life

44
Dialysis and kidney function
Does dialysis cure kidney disease? No. Dialysis does some of the work of healthy kidneys, but it does not cure your kidney disease. You will need to have dialysis treatments for your whole life unless you are able to get a kidney transplant.

45
Dialyzer Diffusion Osmosis Ultrafiltration Fistula Dwell time Exchange
Vocabulary Review Dialyzer Diffusion Osmosis Ultrafiltration Fistula Dwell time Exchange

46
Vocabulary Review Dialyzer- external artifical kidney
Diffusion- passage of particles through a semipermeable membrane Osmosis- movement of fluid across a semipermeable membrane Ultrafiltration- additional pressure to squeeze extra fluid through the membrane Fistula- surgical linking of an artery to a vein, providing access to blood vessels Dwell time- how long dialysate is in the peritoneum Exchange- Once diffusion is complete, all fluid and waste are drained from your peritoneal cavity and replaced with fresh dialysate

47
Kidney Transplants

49
Transplants A surgical implantation of a kidney from a
Living related donor- only need one donated kidney to replace two failed kidneys Living nonrelated donor Deceased donor Tissue type between the donor and recipient need to match. Rejection of the transplant or infection secondary to immunosuppressive drugs are major complications.

50
Complications This surgery can sometimes result in: Blood clots Bleeding Leaking or blockage of the ureter Infection Failure/rejection of donated kidney

51
Organ Donors Those patients awaiting kidney transplants far outnumber the kidneys available to donate. The waiting time for a kidney transplant can be a year or longer. Becoming an organ donor is fairly easy. Registration is done at a local driver’s license bureau.

52
Medications for Transplants
Long-term medications Glucocorticol steroids Prednisone Cyclosporine Azathioprine Mycophenolate mofetil Tacrolimus Sirolimus Thymoglobulin Atgam The doses of these medications are decreased over time until a “maintenance level” is reached.

53
Corticosteroids Associated with: Accelerated protein catabolism Hyperlipidemia Sodium retention Weight gain Glucose intolerance Inhibition of normal calcium, phosphorus, and vitamin D metabolism

54
Cyclosporine and Tacrolimus
Associated with: Hyperkalemia Hypertension Hyperlipidemia

55
MNT for Transplants Protein High protein diet for the first month
g/kg In cases of fever, infection, surgical/traumatic stresses-increase protein requirement to g/kg Fluid Must be monitored closely While on dialysis, patients require a fluid restriction. Transplant patients need to maintain fluid intake Encouraged to drink 2 L/day, but overall needs will depend on urine output

56
MNT for Transplants Potassium
Cyclosporine is associated with Hyperkalemia Restrict potassium intake Usually temporary Calcium and Phosphorus Patient can get hypophosphatemia and hypercalcemia caused by bone resorption The diet should provide adequate amounts of calcium and phosphorus However, serum levels of these nutrients should be monitored periodically If hypophosphatemia does occur, supplement with phosphorus

57
MNT for Transplants Triglycerides and Cholesterol
If these are high, calorie restriction is needed for those that are overweight. Cholesterol intake less than 300 mg/day Limit total fat Patients with glucose intolerance need to limit carbohydrates and maintain a regular exercise program Sodium Moderate sodium restriction ( mEq/day) during periods of fever, infection, or traumatic stresses Helps to minimize fluid retention and controls blood pressure
 during periods of fever, infection, or traumatic stresses. Helps to minimize fluid retention and controls blood pressure.")
58
Post-Transplant Weight Gain
Very common problem This occurs with medication side effects, fewer dietary restrictions, and no physical exercise This problem can be combated by weight management counseling Avoiding/correcting this problem will contribute to the longevity of the transplanted kidney

59
Rates of Survival Living-donor kidney transplants 98% of patients live for at least one year after surgery 90% live for at least five years Deceased -donor kidney transplants 94% live for at least one year after surgery 82% live for at least five years

60
Medications for Dialysis

61
Phosphorus Medications
Commonly used are phosphate binders, including: Calcium Carbonate (TUMS, Calci-chew) Calcium Acetate (PhosLo) Sevalamer Hydrochloride (Renagel)-reduces serum phosphorus without raising serum calcium. Lanthanum Carbonate (Fosrenol) Aluminum hydroxide (AlternaGEL) Common side effects are: hypercalcemia (calcium-based binders), gastrointestinal upset, diarrhea, gas, severe constipation-which may lead to perforation of the intestine which can cause peritonitis or death.
 Calcium Acetate (PhosLo) Sevalamer Hydrochloride (Renagel)-reduces serum phosphorus without raising serum calcium. Lanthanum Carbonate (Fosrenol) Aluminum hydroxide (AlternaGEL) Common side effects are: hypercalcemia (calcium-based binders), gastrointestinal upset, diarrhea, gas, severe constipation-which may lead to perforation of the intestine which can cause peritonitis or death.")
62
Calcium A patient can develop hypocalcemia and hyperphophatemia. Because calcium is in the dialysate bath, the level of calcium can be increased or decreased. Decreased calcium would aid patients who have developed hypercalcemia from active vitamin D administration. Patients who get too much calcium can develop calciphylaxis which is when calcium phosphate is deposited in soft tissues. Calcium is increased with supplements: calcium carbonate calcium acetate calcium lactate, malate, or gluconate Calcium also increased with the mg provided in the diet. Starting calcium supplementation early can prevent hyperparathyroidism.

63
PTH lowering drugs Active vitamin D (available as calcitriol, caltrol, and calcijex)-to treat hypocalcemia. Hectorol and Zemplar-lowers PTH and raises calcium levels. Cinacalcet (calcimemetic)-a calcium imitating drug that binds to sites on the parathyroid gland which gives the gland a false impression that calcium levels are elevated.
-a calcium imitating drug that binds to sites on the parathyroid gland which gives the gland a false impression that calcium levels are elevated.")
64
Overview of Drugs Phophate binders Calcium carbonate Calcium acetate
Sevelamer hydrochloride Lanthanum carbonate Aluminum hydroxide Iron IV iron (iron dextran, Aron gluconate, iron sucrose Erythropoietin IV or IM (Epogen or EPO) Activated Vitamin D Oral (Hectorol) IV (Calcitriol) Biphosphonates Oral (Alendronate-fosamax) IV (Pamidronate)
 Activated Vitamin D. Oral (Hectorol) IV (Calcitriol) Biphosphonates. Oral (Alendronate-fosamax) IV (Pamidronate)")
65
Overview of Drugs Cont. Calcium supplements TUMS, Os-Cal, Calci-chew
Phosphorus supplements Kphos, NutraPhos, NutraPhos K Calcimimetics Cinacalcet Heavy Metal Chelator- binds aluminum and iron and is dialyzed off IV Desferal (deferoxamine or DFO) Cation Exchange Resin-for hyperkalemia Oral or rectal (sodium polystyrene sulfonate or SPS)
 Cation Exchange Resin-for hyperkalemia. Oral or rectal (sodium polystyrene sulfonate or SPS)")
66
Renal Osteodystrophy Three types: Osteomalacia (bone demineralization)
Osteitis fibrosa cystica (caused by hyperparathyroidism) Metastatic calcification of joints and soft tissues A fourth type unique to renal failure patients on active vitamin D is low turnover bone disease. This bone disease is characterized by the oversuppression of the parathyroid gland with too much active vitamin D. It causes decreased bone formation and fragile bones with very little matrix. Control these conditions with the drugs discussed above.
 Metastatic calcification of joints and soft tissues. A fourth type unique to renal failure patients on active vitamin D is low turnover bone disease. This bone disease is characterized by the oversuppression of the parathyroid gland with too much active vitamin D. It causes decreased bone formation and fragile bones with very little matrix. Control these conditions with the drugs discussed above.")
67
Medical Nutrition Therapy

68
To prevent deficiency and maintain good nutrition status
MNT Goals To prevent deficiency and maintain good nutrition status To control edema and electrolyte imbalance To prevent or retard the development of renal osteodystrophy To enable the patient to eat a palatable, attractive diet that fits his/ her lifestyle

69
Nutrient Requirement Chart
Kcal Protein Fluid Sodium Potassium Phosphorus Hemodialysis 35 kcal/kg IBW 1.2 g/kg ml/day + urine output mg/day mg/day g/day Peritoneal dialysis (PD) 30-35 kcal/kg IBW g/kg minimum of 2000 ml/day mg/day mg/day
 kcal/kg IBW g/kg. minimum of 2000 ml/day mg/day mg/day.")
70
+ Fluid from solid food: 500- 800 ml/day
Fluid Intake Limited fluid intake ml/day + amount equal to the urine output + Fluid from solid food: ml/day Deal with thirst with drinking: Sucking on a ice chips, cold sliced fruit, sour candies, using artificial saliva, or chewing “sports gum”

71
-equals 2% – 5% of body weight Peritoneal dialysis:
Goals of fluid gain Hemodialysis: - 4 to5 lb fluid gain of body weight in the vasculature between treatments -equals 2% – 5% of body weight Peritoneal dialysis: - No fluid limited

72
- no salt in cooking, avoids convenience foods
Sodium Sodium restriction mg/day - no salt in cooking, avoids convenience foods - help to reduce thirsts and fluid intake - Conditions with salt-losing tendency need 3g or more sodium per day. Diseases of conditions with salt-losing tendency: polycystic disease of the kidney, medullary kidney disease, chronic obstructive uropathy, chronic pyelonephritis, and analgesic nephropathy. 3000 mg sodium /day is needed for conditions with salt-losing tendency to prevent hypotension, hypovolemia, cramps, and further deterioration of renal function.

73
2000 mg/day for anuric patient
Potassium mg/day for ESRD 2000 mg/day for anuric patient low-sodium foods & salt substitutes contain KCl instead of NaCl Food Sources: fruits and vegetables

74
- Must rely on PTH to keep calcium level up through bone reabsorption
Calcium and Vitamin D Increase calcium - Decrease ability of kidney to covert the inactive form of vitamin D to , 1,25(OH)2D3 - Therefore cannot increase gut absorption of calcium - Must rely on PTH to keep calcium level up through bone reabsorption Vit supplement – only Active D3 form
2D3 - Therefore cannot increase gut absorption of calcium. - Must rely on PTH to keep calcium level up through bone reabsorption. Vit supplement – only Active D3 form.")
75
Restrict phosphorous intake:
1200 mg/day or less 17 mg/kg of body weight Food source of P: dairy and meat Problem: Calcium rich foods (milk) and high-protein diet are high in phosphorous Phosphate have high molecular weight Phosphate-binding medication is required Dietary restriction alone is not adequate to control serum phosphorus.
 and high-protein diet are high in phosphorous. Phosphate have high molecular weight. Phosphate-binding medication is required. Dietary restriction alone is not adequate to control serum phosphorus.")
76
A normal waste product of muscle breakdown.
Creatinine A normal waste product of muscle breakdown. Can be controlled by dialysis. Low creatinine level may indicate good dialysis or low body muscle.

77
Inability od kidney to produce EPO
Iron Inability od kidney to produce EPO EPO is a hormone that stimulates the bone marrow to produce red blood cells and an increased destruction of red blood cells secondary to circulating uremic waste products A synthetic form of EPO, periodic IV, and oral iron are used to correct the anemia.

78
Water-Soluble Vitamins
Water-soluble vitamins loss during dialysis - Dietary restriction (water-soluble vitamins are high in K+ and P foods) - loss Ascorbic acid, niacin, riboflavin, and vit. B6 - folate is highly dialyzable (supplement is recommended) - Loss of vit. B12 is minimal Fat-soluble vitamins do not loss much Folic acid 3-6 mg/day Vit. E supplement is not routinely recommended Avoid vit. K supplements
 - loss Ascorbic acid, niacin, riboflavin, and vit. B6. - folate is highly dialyzable (supplement is recommended) - Loss of vit. B12 is minimal. Fat-soluble vitamins do not loss much. Folic acid 3-6 mg/day. Vit. E supplement is not routinely recommended. Avoid vit. K supplements.")
79
Lipid Atherosclerotic cardiovascular disease is the most common cause of death among long term dialysis patients Although lipids lowering drug may have significant impact on management, treatment of hyperlipidemia still remains controversial.

80
Enteral Tube Feeding & Parenteral Nutrition
- ESRD patients usually doing well on standard formulas - Refeeding syndrome may occur when taking a low phosphorus level of the “renal” products Parenteral Nutrition - Used for malnourished patients with GI complications

81
Case Study

82
Occupation: Secretary
Case Study EJ 24 y.o.f Occupation: Secretary Chief Complaints: anorexia, n/v, weight gain, edema, malaise, SOB, pruritus, muscle cramps, inability to urinate Poor oral intake due to anorexia and n/v

83
Ht: 5’ (1.5 m) Wt: 170 lbs (77 kg) BMI: 33 IBW: 100 lbs %IBW: 170
Anthropometric Ht: 5’ (1.5 m) Wt: 170 lbs (77 kg) BMI: 33 IBW: 100 lbs %IBW: 170
 Wt: 170 lbs (77 kg) BMI: 33. IBW: 100 lbs. %IBW: 170.")
84
Abnormal Labs: Biochemical Sodium 130 (L)* Potassium 5.8 (H)*
Chloride 91 (L)* PO (H) Glucose 282 (H) BUN 69 (H)* Creatinine 12 (H)* Calcium 8.2 (L)* Cholesterol 220 (H) Triglycerides 200 (H) *indicative of kidney failure
* PO4 9.5 (H) Glucose 282 (H) BUN 69 (H)* Creatinine 12 (H)* Calcium 8.2 (L)* Cholesterol 220 (H) Triglycerides 200 (H) *indicative of kidney failure.")
85
Dry, yellowish brown skin Generalized rhonchi with rales, SOB
Clinical Overweight Lethargic Muscle weakness Dry, yellowish brown skin Generalized rhonchi with rales, SOB Edema in extremities, face, and eyes Elevated blood pressure (220/80) Normal pulse, normal bowel sounds
 Normal pulse, normal bowel sounds.")
86
Usual dietary intake Breakfast Lunch Dinner Snacks Dietary Assessment
Cold cereal, bread or fried potatoes, fried egg Lunch Bologna sandwich, potato chips, Coke Dinner Chopped meat, fried potatoes Snacks Crackers and peanut butter

87
Current calorie order: 30 kcal/kg or 2300 cal/day
Dietary Assessment Current calorie order: 30 kcal/kg or 2300 cal/day Estimated calorie needs: 23 kcal/kg or 1800 cal/day HEB: (13.7*77)+(5*152)-(6.8*24)= 1700 cal Protein needs: 0.8 gm/kg Fluid needs: 25 ml/kg or 1900 ml/day Sodium restriction 2-3 g/day Phosphorus restriction 8-12 mg/day
+(5*152)-(6.8*24)= 1700 cal. Protein needs: 0.8 gm/kg. Fluid needs: 25 ml/kg or 1900 ml/day. Sodium restriction 2-3 g/day. Phosphorus restriction 8-12 mg/day.")
88
Mom and dad both dx with type II diabetes
History Mom and dad both dx with type II diabetes Type II diabetic for 11 years Meds: Glucophage Vasotec

89
PES Statement Limited adherence to nutrition-related recommendations related to diagnosis of type II diabetes as evidenced high blood glucose levels, obesity, and stage 3 chronic kidney disease.

90
Nutritional Intervention
Reeducate on importance of adherence to diabetic diet. Assess reasons for past noncompliance. Supplement diet with nutrition shakes Encourage cessation of alcohol consumption Educate on proper diet for renal disease (low potassium, phosphorus, sodium)
")
91
Sample Diet Breakfast Snack Lunch Dinner 1 slice toast with margarine
6 oz orange juice Snack 1 cup cereal with 8 oz milk Lunch 1 ham and cheese sandwich 8 medium carrot sticks 4 graham crackers 8 apple slices Dinner 1 ½ cups stir-fried chicken with 1 cup rice 1 cup sautéed green beans 1 dinner roll with margarine ½ cup peach slices This diet is low in fluid, high in fruit and vegetables (which add potassium), high in grains (which help add calories and flavor), low in dairy (therefore low in phosphorus), and high in protein (which is wasted in dialysis). For diabetes, it is good because there are five small meals throughout the day, which helps balance blood sugar.
, high in grains (which help add calories and flavor), low in dairy (therefore low in phosphorus), and high in protein (which is wasted in dialysis). For diabetes, it is good because there are five small meals throughout the day, which helps balance blood sugar.")
92
References National Kidney foundation. Dialysis. Accessed March 20, 2012. The Renal Unit. What is a dialysis fistula. Accessed March 20, 2012. Ben Franklin Technology Partners. Improving the Success of Kidney Dialysis. Accessed March 20, 2012. National Kidney Disease Education Program. Dialysis. Accessed March 20, 2012. National Kidney & Urologic Diseases Information Clearinghouse (NKUDIC). Treatment Methods for Kidney Failure. Accessed March 20, 2012. Kutner N. Improving Compliance in Dialysis Patients: Does Anything Work? Sem Dial.14: Baxter Healthcare. Dialysis Options. Accessed March 20, 2012. Moriishi M, Kawanishi H, Tsuchiya S. Impact of combination therapy with peritoneal dialysis and hemodialysis on peritoneal function. Adv Perit Dial. 2010;26:67-70. PubMed. Dialysis. Accessed March 20, 2012. American Kidney Fund. Treating Kidney Disease . Accessed March 20, 2012.
. Treatment Methods for Kidney Failure. Accessed March 20, Kutner N. Improving Compliance in Dialysis Patients: Does Anything Work Sem Dial.14: Baxter Healthcare. Dialysis Options. Accessed March 20, Moriishi M, Kawanishi H, Tsuchiya S. Impact of combination therapy with peritoneal dialysis and hemodialysis on peritoneal function. Adv Perit Dial. 2010;26: PubMed. Dialysis. Accessed March 20, American Kidney Fund. Treating Kidney Disease . Accessed March 20,")
93
References Medline Plus. End-stage kidney disease. Accessed March 17, 2012. Wilkens KG, Juneja V. Medical nutrition therapy for renal disorders. In: Mahan LK, Escott-Stump S, ed. Krause’s Food, Nutrition, & Diet Therapy. 12th ed. Philadelphia: Elsevier; 2008: PubMed. Comorbidities in patients with end-stage renal disease. Accessed March 17, 2012. Saliba W. Calcium and phosphorus metabolism in renal failure. J Am Board Fam Med. 2009;22(5): Oregon State University. Calcium and phosphorus homeostasis. Accessed March 19, 2012. New York-Presbyterian. Transplantation: KidneyTransplant. Accessed March 16, 2012 Organ Procurement and and Transplantation Network. Donor Matching System. Accessed March 16, 2012 Mayo Clinic. Kidney Transplant. Accessed March 16, 2012 Donate Life America. Accessed March 16, 2012
: Oregon State University. Calcium and phosphorus homeostasis. Accessed March 19, New York-Presbyterian. Transplantation: KidneyTransplant. Accessed March 16, Organ Procurement and and Transplantation Network. Donor Matching System. Accessed March 16, Mayo Clinic. Kidney Transplant. Accessed March 16, Donate Life America. Accessed March 16,")
Similar presentations






activate vitamin D (renal 1-alpha hydroxylase) produces erythropoietin.>")

>")







>")

 –220 per million in 1992 –334 per million in 2000 Prevalence (number of.>")


