Download presentation
Presentation is loading. Please wait.

1
Public Health, Health Promotion & Population Health
Week 3 & 4: Sept

2
Health Promotion Health Promotion “A process of enabling people to increase control over and improve their health” (WHO, 1984) Focuses on… Broader determinants of health Intersectoral approaches Environmental change Policy and organizational levels Outcomes such as “social conditions” Empowering individuals and changing systems (Minkler, 1989)
")
3
“Change will demand the attention of all individuals, NGOs, business, communities, all levels of government and all sectors of our Canadian society. Success will require leadership from our prime minister and first ministers, from our mayors, municipal leaders, community leaders, and the leaders of our Aboriginal peoples. A whole-of-government approach is required with intersectoral action embracing business, volunteers, and community organizations. This will not be easy, but it can and must be done. We cannot afford to do otherwise.” A Healthy, Productive Canada, Senate of Canada, 2009

4
INTERSECTORAL “The complexities of the social, political, economic and environmental factors that influence health and inequities in health and the fact that most of these determinants lie outside of the exclusive jurisdiction of the health sector, necessitate working across sectors of government and society.” Health equity through intersectoral action: An analysis of 18 case studies, PHAC and WHO, 2008

5
How has the field of health promotion evolved?
The Public Health Era ( ) Medical Model ( s) Health Promotion Era Lalonde, “A New Perspective on the Health of Canadians” Alma Ata Declaration, 1978 WHO adopts ‘Health for All by the Year 2000’, 1980s focus other health determining factors, particularly the environment
 Medical Model ( s) Health Promotion Era. Lalonde, A New Perspective on the Health of Canadians Alma Ata Declaration, WHO adopts ‘Health for All by the Year 2000’, 1980s focus other health determining factors, particularly the environment.")
6
How has the field of health promotion evolved?
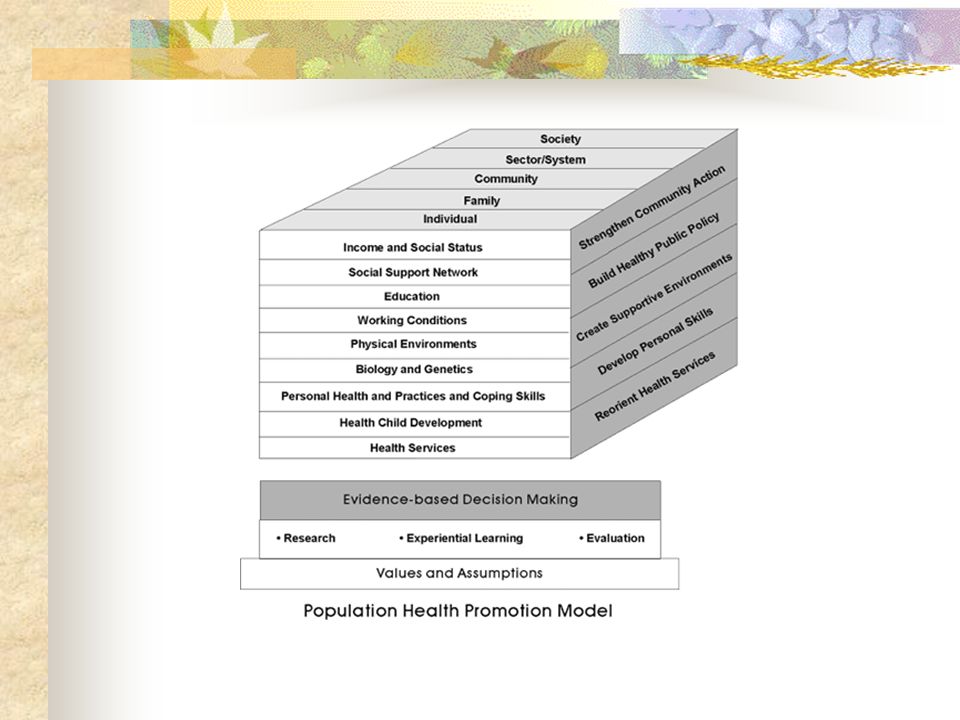
WHO, Ottawa Charter for Health Promotion Epp, Achieving Health for All: A Framework for Health Promotion Strategies for Population Health, 1994 Population Health Promotion Model 1996

7
How has the field of health promotion evolved?
Themes of “Decentralization” &“Participation” Integrated programs vs. sum of a number of small scale programs Multiple goals and sectors Active participation of both health and non-health sectors consumer demand community coalitions

8
Lalonde Report (1974) “A New Perspective on the Health of Canadians” Lalonde, 1974 Term ‘health promotion’ used for the first time Identified factors other than health care that contribute to health No structural reform-health promotion added to the medical system Led to lifestyle campaigns-healthy eating, seatbelt, impaired driving

9
Health Field Concept (1974)
Human Biology Lifestyles Health 4 fields for health improvement -- Environment Organization of Medical Care

10
Health Promotion Touchstones
International Conference on Primary Health Care Canada’s Health Promotion Directorate established Declaration of Alma-Alta health is a human right gov’ts responsible for health of citizens people have a duty to participate in health decisions

11
Health Promotion Touchstones
WHO adopted Health for all by the year 2000 Primary health care emphasis Broad definition of Health Values for health articulated

12
Health Promotion Touchstones
First International Conference on Health Promotion held in Ottawa Ottawa Charter for Health Promotion as means towards “Health for All”

13
Ottawa Charter for Health Promotion, 1986 What is the significance?
Defined health promotion as “the process of enabling people to increase control over and to improve their health” Defined health as “a resource for everyday life” Belief that the health sector alone cannot create health – intersectoral coordination

14
Ottawa Charter Five strategies for action: build healthy public policy
strengthen community action develop personal skills create supportive environments reorient health services Includes in definition of health promotion -- -- creation of policies and environments that support healthful decisions and the -- tailoring of health services to promote preventive, and not just clinical care.

15
Prerequisites for Health
Peace Shelter Education Food Income Stable ecosystem Sustainable resources Social justice and equity

16
Ottawa Charter for Health Promotion, 1986 What is the significance?
5 strategies for action Build healthy public policy Strengthen community action Develop personal skills Create supportive environments Reorient health services

17
2nd International Conference on Health Promotion, Adelaide
Final Conference Statement “Peace and social justice, nutritious food and clean water, a useful role in society and an adequate income, conservation of resources and the protection of the ecosystem, are prerequisites for health and social development. The vision of healthy public policy is for achievement of these fundamental conditions for healthy living.”

18
Achieving Health for All: A framework for health promotion
Jake Epp -- National Minister of Health Companion document to the Ottawa Charter Outlined realistic actions for government READ overhead SWITCH to FRAMEWORK DIAGRAM Three Challenges -- reduce inequities -- increase prevention of disease -- enhance coping Three Health Promotion Mechanisms -- to take care of yourself -- Self Care -- to take care of your family and community -- Mutual Aid -- to take care of your environment -- Healthy Environments Three Implementation Strategies -- fostering public participation -- strengthening community health services -- coordinating healthy public policy

19
Epp Report “. . . We cannot invite people to assume responsibility for their health and then turn around and fault them for illnesses and disabilities which are the outcome of wider social and economic circumstances.” The Epp Report, 1986 “It’s not that lifestyle choices such as good nutrition and exercise don’t matter – they do. But a substantial body of evidence has shown that the broader determinants of health have an impact on our lives that is just as strong, if not stronger.” -- stepping it up, Health Council of Canada, 2010

20
Achieving Health for All, Epp 1986 What is the significance?
Outlined realistic action for government Three challenges Reduce inequities Increase prevention of disease Enhance coping Health promotion mechanisms identified Companion document to Ottawa charter Epp. Health promotion mechanisms – self care, mutual aid, healthy environments

21
Achieving Health for All Framework (Epp Paper)
")
22
Strategies for Population Health, 1994 What is the significance?
First time “population health” term is used The document Summarized the determinants of health Provided a framework to guide policy development Gave strategic direction for cooperation and action Population Health: Strategies address the entire range of factors that determine health Strategies are designed to effect the entire population

24
The Determinants of Health
Income & Social Status Social Support Networks Education Employment & Working Conditions Physical Environment Biology & Genetic Endowment Personal Health Practices & Coping Skills Healthy Child Development Health Services Gender Culture

25
Population Health & Health Promotion
Created a rift between health promotion and population health Population Health Promotion Model

27
Primary Health Care Renewal
Action for Healthier Nova Scotians – 2003 To improve health by a primary health care system that is: Community-based, family-focused, person-centred Comprehensive Responsive & flexible Accessible Integrated, collaborative & innovative Accountable Sustainable

28
Bangkok Charter for Health Promotion in a globalized world, 2005
To complement & build upon Ottawa Charter Strategies Advocate Invest Build Capacity Regulate and legislate Partner Commitments to health for all Make the promotion of health: Central to global development agenda Core responsibility for all government Key focus of communities and civil societies Advocate for health based on human rights and solidarity Invest in sustainable policies, actions, and infrastructure to address the determinants of health Build capacity – policy dev. leadership, health promotion practice, knowledge transfer and research, and health literacy Reg. and leg. – ensure high level of protection from harm and enable equal opportunity for health and well being for all people Partner – with public, private , NGOs and civil society to create sustainable actions Commitment == psychological and designation of institutional resources

29
Inequity or Inequality?
Refers to health differences that may be reduced but not eliminated; may be due to genetics or aging. Inequity Refers to differences that are unfair and preventable; action can be taken to reduce inequities Stepping it Up, Health Council of Canada, 2010

30
Inequities in Health Status
Does higher income and social status provide a buffer or defence against disease? Does lower income and social status undermine the body’s defenses? Single most important determinant of health

31
Why Higher Income=Better Health?
Higher income improves ability to: purchase basic needs such as housing & food make more choices and feel more in control Feeling of being in control is basic to good health.

32
Inequity and Illness www.unnaturalcauses.org
Unnatural Causes: Is inequality making us sick? Video series – brief online intro

33
Income & Social Status Perceived Health Status
47% of Canadians in the lowest income bracket rate their health as very good or excellent compared to 73% in the highest income group Lower Income Canadians doubly worse off shorter life expectancies higher burden of ill health during shorter lifetimes Compared with higher income groups, regardless of their age, sex, race or place of residence Influences the degree of control in which people have over their life circumstances

34
Income and Social Status
Top 20% income bracket vs. bottom 20% Men live 6 years longer expect 14 more years disability-free life Women live 3 years longer expect 8 more years disability-free life Review After rent incomes of food bank users in 2002 ½ of what they were in 1993 Income differences account for 23.7% excess in premature CVD deaths among Canadians – Dennis Raphael SWITCH to opaque projector for Whitehall graphs

35
Costs of Poverty In 2005, overall poverty rate – 11% Canadians
BUT 26% lone-parent families; 21% work-limited; 19% recent immigrants; 17% off-reserve aboriginals 11.5% of children under 18 live in poverty OECD indicates rate in Canada is 15% Lowest income quintile (working poor & on social assistance) rates of DM & CVD double those in the richest quintile Income inequality growing in Canada over past 10 years Now higher than the OECD average Disproportionate – inequity OECD – Organization for Economic co-operation and Development growing poverty rates x10 years – even though had been declining for 20 years – AND higher than OECD average
 rates of DM & CVD double those in the richest quintile. Income inequality growing in Canada over past 10 years. Now higher than the OECD average. Disproportionate – inequity. OECD – Organization for Economic co-operation and Development. growing poverty rates x10 years – even though had been declining for 20 years – AND higher than OECD average.")
36
Health Care Costs of Health Inequity
Saskatoon Study Residents from lower SES areas use disproportionate levels of doctor, medication and hospital services Mainly due to higher prevalence of disease Consume 35% more health care resources than higher income $179 million more than middle-income groups

37
Health Care Costs of Health Inequity
Winnipeg study Eliminating gap between richest & poorest neighbourhoods could reduce Heart attacks by 22% Hip fractures by 20% Health care costs by $62 million in 1999 or 15% of physician & hospital expenses PHAC working on report on health status & health care cost by income level in Canada To be released in 2011

38
Economic Downturn: Coping strategies
Economy tops list of concerns (22%) Job security second (13%) Cut household expenses Out-of-home entertainment (63%) Spend less for new clothes (55%) Switch to cheaper grocery brands (55%) Eat at home more often now Breakfast (23%); Pack Lunch (26%); Dinner (39%) Look for deals Only buy when on sale (44%); use coupons (23%); stock up at sales (18%) Today – expenditures on food constitute the largest single category for the world at large – -- 21% in Western developed nations -- 50+% in developing nations (Paul Rozin, APA journal, 1996) Canadians surveyed – second on list was job security (13%) Nielsen, 2009
 Job security second (13%) Cut household expenses. Out-of-home entertainment (63%) Spend less for new clothes (55%) Switch to cheaper grocery brands (55%) Eat at home more often now. Breakfast (23%); Pack Lunch (26%); Dinner (39%) Look for deals. Only buy when on sale (44%); use coupons (23%); stock up at sales (18%) Today – expenditures on food constitute the largest single category for the world at large – -- 21% in Western developed nations % in developing nations (Paul Rozin, APA journal, 1996) Canadians surveyed – second on list was job security (13%) Nielsen,")
39
Debt, Obesity, Food Access
German study of household spending during economic downturns People borrow to make ends meet 7.6% over-indebted (over 6 million people) Higher prevalence of overweight, obesity, depression, tobacco use Authors noted Depression could lead to increased food intake Eating offers compensation & gratification Less money may limit leisure & sporting activities resulting in less energy expenditure Obesity might affect job prospects First time indebtedness has been shown to be linked to negative health outcomes -- younger, less educated, lower income -- higher prevalence of overweight, obesity, depression and tobacco use Muster, et al., (in press), BMC Public Health
 Higher prevalence of overweight, obesity, depression, tobacco use. Authors noted. Depression could lead to increased food intake. Eating offers compensation & gratification. Less money may limit leisure & sporting activities resulting in less energy expenditure. Obesity might affect job prospects. First time indebtedness has been shown to be linked to negative health outcomes. -- younger, less educated, lower income. -- higher prevalence of overweight, obesity, depression and tobacco use. Muster, et al., (in press), BMC Public Health.")
40
Social Support Networks
Support from families, friends and communities Believing that one is valued as a provider of support for others in need Helps people solve problems, deal with adversity and give them a sense of control Results in feelings of satisfaction, well-being and comfort Social Support Affects: Mortality (death rate) Psychological/emotional health Physical health Health perceptions How individuals and families manage disease and illness
 Psychological/emotional health. Physical health. Health perceptions. How individuals and families manage disease and illness.")
41
Social Supports and Health
Most NB health protecting feature is perception of available support Quality more NB than quantity Importance placed on support networks varies with situation Healthiest support relationship is reciprocal 1. My family and friends will always be there for me when I need help 2. My family may be far away, but I can always count on them when I need help. 3. My family and friends have been there for me in the past to share my joys and sorrows. 4. Members of my family will support me when I need it and come to me for support when they need it. My family and friends know they can always confide in me and ask me for advice.

42
Connectedness & Health
Review of 148 studies (n=300,000+) by Brigham Young University on quality of life Clear that stronger social relationships increased chance of survival by 50% Effect consistent across age, sex, health status Social support likely a ‘buffer’ against stress -- provides emotional and tangible resources to help us deal with adverse events and illness -- being part of a social network gives us meaningful roles that boost self-esteem and purpose in life improve health -- “We take relationships for granted. We’re like fish that don’t notice the water.” – Timothy Smith, one of the researchers Low Social Support has been associated with non-adherence at 1-year point to CVD diet suggesting greater risk for CVD -- study of Family Intervention Trial for Heart Health (FIT Heart) -- cardiac patients (n=458) 66% female; 35% non-white; mean age 50 years -- low SS had 2.7 times greater odds of being non-adherent to diet at 1 year vs those with higher SS Aggarwal, B., Liao, M., Allegrante, J.P., & Mosca, L. (2010). Social support level is associated with non-adherence to diet at 1 year in the Family Intervention Trial for Heart Health (FIT Heart). Journal of Nutrition Education and Behavior, 42(6),
 by Brigham Young University on quality of life. Clear that stronger social relationships increased chance of survival by 50% Effect consistent across age, sex, health status. Social support likely a ‘buffer’ against stress. -- provides emotional and tangible resources to help us deal with adverse events and illness. -- being part of a social network gives us meaningful roles that boost self-esteem and purpose in life improve health. -- We take relationships for granted. We’re like fish that don’t notice the water. – Timothy Smith, one of the researchers. Low Social Support has been associated with non-adherence at 1-year point to CVD diet suggesting greater risk for CVD. -- study of Family Intervention Trial for Heart Health (FIT Heart) -- cardiac patients (n=458) 66% female; 35% non-white; mean age 50 years. -- low SS had 2.7 times greater odds of being non-adherent to diet at 1 year vs those with higher SS. Aggarwal, B., Liao, M., Allegrante, J.P., & Mosca, L. (2010). Social support level is associated with non-adherence to diet at 1 year in the Family Intervention Trial for Heart Health (FIT Heart). Journal of Nutrition Education and Behavior, 42(6),")
43
Social Cohesion -- Roseto Effect
Study showed a loss of social solidarity mutual dependence AND homogeneity (similarity due to common descent) led to more deaths from heart attacks READ -- Roseto synopsis from binder (C-2.20-C-2.21
 led to more deaths from heart attacks. READ -- Roseto synopsis from binder (C-2.20-C")
44
Education & Literacy Higher education = greater health
More opportunities for jobs, job security, and job satisfaction Improves the ability for individuals to understand the information that will keep them healthy Supporting Evidence self-rated health status activity limitations fewer workdays lost to illness or injury Equips people with the skills for problem solving National Population Health Survey 19% of participants with less than high school education rated their health as excellent compared to 30% of University graduates

45
Working Conditions Variety of factors relate health to employment and working conditions What are some of these factors? Hazards/safety issues injuries unemployment.fear of unemployment status control of participation in decision-making interactions with co-workers job demands physical environment (air, temp, lights, furniture, etc.) degree of supportiveness for healthy choices (food exercise, day care, job sharing, flex hours) adequate salary and benefits stress levels
 degree of supportiveness for healthy choices (food exercise, day care, job sharing, flex hours) adequate salary and benefits. stress levels.")
46
Underemployment and Overemployment
Both issues of concern Skills not being used Workers around after lay-offs typically have to work harder or longer than in the past

47
Employment & Working Conditions
People that have more control over their working environment tend to have lower stress levels and often live longer Supporting Evidence Between the proportion of Canadian Workers who were very satisfied with their work declined; Females = 58% 49% Women aged were most likely to report higher work stress than the average Canadian worker

48
Unemployment and Health
Longer term unemployment die prematurely suicide rates cardiovascular disease rates Spouses and children of unemployed workers emotional and behavioral problems Recovery of physical and mental health after unemployment is neither immediate nor complete.

49
Determinants & Obesity
US study released Dec/2010 Poor women more likely to be obese Education level linked for both sexes NCHS study, 2010 N=5000 – part of national surveillance studies

50
Physical Environments
Natural Human-built Natural -- land, air, water Human-built -- housing, workplaces, community facilities, communicaiton links, transportation, indoor air quality

51
Housing and Health Children’s health affected by
overcrowded, poor-quality housing Children of low income families more likely to live in poor-quality housing Children from poorest families almost twice as likely to live in housing needing major repairs than those from wealthiest families. Over 18% Cnds live in substnd housing 1 in 5 renters spend 50%+ income on housing

52
Personal Health Practices
Individual decisions people make that directly affect their health Knowledge, behaviours, attitudes, values Behaviours people choose to do or not do in daily lives EXAMPLES?? Smoking, food choices, activity patterns

53
Healthy Child Development
Prenatal & early childhood experiences key Child development greatly affected by housing, neighborhood, family income, and level of parents‘ education, access to nutritious foods, physical recreation, genetic makeup and access to dental and medical care Supporting Evidence Experiences from conception to 6 yrs have the most important influence of any time on the life cycle on the connecting and sculpting of the brains neurons. 90% Canadian families lack access to affordable licensed childcare

54
Gender Gender roles defined by culture
Sex-specific difference in disease are biology based Impact of gender NOT due to biology but to societal attitudes E.g., differences in income and social status between men and women have major impact on health. These differences are NOT due to biology but to societal attitudes. Roles, personality traits, attitudes, behaviours, values, relative powers, and influences society assigns to the two sexes Supporting Evidence Women are 3 times more likely than men to be poor

55
Culture Whole complex of shared values, beliefs, practices
Binds people together Gives sense of who we are & where we belong Shapes our actions Supporting Evidence Infant mortality rates among First Nations people between 1979 & 1994 were twice as high compared to the Canadian pop. as a whole Complex of relationships, knowledge, languages, social institutions, beliefs, values & ethical

56
Culture How we interact with health care system
Participation level in prevention and health promotion programs Access to health information Health-related lifestyle choices Understanding of health and illness 1. Comfortable with technology or traditional medicine? -- traditionally use health system or rely on family? -- “allowable” to interact with health professional of diff gender 2. What are customs related to food prep? Which V/F or meats eaten? -- timing of meals? -- fasting days? 3. Is info presented in culturally appropriate manner? -- What is literacy level? -- transportation available? Child care available? -- Is asking for help part of culture? 4. Does culture attach high status to risk-taking recreational activities? -- what items are considered food? -- does culture support recreational fitness activities? 5. Are beliefs fatalistic or do they believe they have some control?

57
Culture Determines much of our defn of food, its symbolic meanings, uses, and the social context in which it is consumed or avoided Culture is in dynamic interaction with biology, the physical environment, and other social and economic forces David Himmelgreen, 2002, Nutritional Anthropology 25(1), 2-12. 1. Defn of Nutritional Anthropology This interaction and its effects on food choice will be further explored when we discuss ecological models in the next section.
, Defn of Nutritional Anthropology. This interaction and its effects on food choice will be further explored when we discuss ecological models in the next section.")
58
Biology and Genetics Genetic endowment appears to predispose certain individuals to a particular disease or health problem Genes can be turned on or off by the environment ASK for examples -- rheumatoid arthritis/ lupus -- cystic fibrosis -- obesity -- diabetes – NW ON Cree dx at a rate 5x Cnd nat’l avg (less active lifestyle, new foods, more stress) -- colon, prostate, breast cancer -- heart disease, stroke Visible minorities earn 30% less than whites 2X as likely to be poor Women, aboriginal people, Cnds of colour, & New Cnds especially vulnerable
 -- colon, prostate, breast cancer. -- heart disease, stroke. Visible minorities earn 30% less than whites. 2X as likely to be poor. Women, aboriginal people, Cnds of colour, & New Cnds especially vulnerable.")
59
Spirituality That which gives meaning to life
Not solely based on religious beliefs Evidence blood pressure control strengthened immune system coping with disease & death recovery & survival self-worth and self esteem

60
Health Services Health services, particularly those designed to maintain and promote health, prevent disease, and to restore health and function contribute to population health Supporting Evidence Disease & injury prevention activities in areas such as immunization and mammography are showing positive results Facilitate community development, empowerment, health promotion Prevent disease & injury Educate re: risks and choices Ensure safe food, water, air Help maintain independence Treat & cure emergency injury or illness

61
Interrelated Determinants
“Income is a determinant of health in itself, but it is also a determinant of the quality of early life, education, employment and working conditions, and food security. Income is also a determinant of the quality of housing, the need for a social safety net, the experience of social exclusion, and the experience of unemployment and employment insecurity across the lifespan.” Social Determinants of Health, Dennis Raphael, 2009

62
Population Health Underlying Assumptions
Health determined by complex interactions Health of population closely linked to distribution of wealth Strategies address entire range of determinants Focusing on population leads to greater health gains Improving health a shared responsibility Health is determined by the complex interactions between individual characteristics, social and economic factors and physical environments. The health of a population is closely linked to the distribution of wealth across the population. Strategies to improve population health must address the entire range of factors that determine health. Important health gains can be achieved by focusing interventions on the health of the entire population (or significant sub-populations) rather than individuals. Improving health is a shared responsibility that requires the development of healthy public policies in areas outside the traditional health system.
 rather than individuals. Improving health is a shared responsibility that requires the development of healthy public policies in areas outside the traditional health system.")
63
INTERSECTORAL Best practices for addressing poverty point to a broad, integrated approach that engages community partners as well as all orders of government . . . Reducing poverty: An action plan for Newfoundland and Labrador, 2006 Poverty reduction strategies in some P/T involve gov’t wide integrated approach based on the principles of social inclusion and collaboration NS – working on gov’t wide child obesity strategy

64
Population Health Promotion Model What is the significance?
Health Promotion is a process for enabling people to take control over & improve their health Population Health addresses the relationship between the determinants of health & how determinants influence the health of entire populations

65
Population Health Promotion Model What is the significance?
Integrates health promotion and population health Uses sectors of population health, the determinants of health, and strategies from the Ottawa Charter to guide action Who? What? How? Focuses on “whole populations” and “all factors that determine health” Requires collaborative action Activity

66
Tips for Better Health: Compare & Contrast
Don’t smoke Follow a balanced diet Be physically active Manage stress Drink alcohol in moderation Cover up in the sun Practice safe sex Don’t be poor Don’t have poor parents Don’t work in stressful low paid manual job Don’t live in damp, low quality housing Be able to take vacation Don’t live next to a busy highway Making the point of the determinants of health and which ones we might have control over and which ones we don’t and are considered our social determinants of health. Which do you hear most often as determinants of health Which do you think the evidence suggests is the most effective approach

67
Hmmm . . . “. . . It is unacceptable for a wealthy country such as Canada to continue to tolerate such disparities in health.” Senate of Canada, 2009 “Canada was once an innovative leader in promoting the importance of the determinants of ehalth, starting in 1974 with a landmark report, A new Perspective on the health of Canadians – LaLonde Report.

68
Disease Prevention Primary Prevention Secondary Prevention
How to avoid disease Control of incidence Secondary Prevention How to cure it Control of duration and hence prevalence Tertiary Prevention How to appease it Control of further complications Primary -- includes health promotion, some protection initiatives such as immunization, environmental control measures, nutrition and genetic counseling - deals with people in a pre-disease state or with inapparent disease status Secondary -- includes screening (for risk -- use of growth charts, cholesterol testing, waist circumference), early diagnosis (to detect and treat disease early -- pap smear, HIV testing, occult blood screening) - deals with people without apparent disease state (preclinical) and those with manifest early clinical disease Tertiary -- aims to minimize disability and restore function and productivity of patient (renal dialysis); - includes rehabilitation and palliative care - deals with people in early to advanced clinical disease states Public health will work mainly at the primary prevention level, but with some secondary preventive activities. Community health will work mainly at the secondary prevention level but with some primary preventive services
, early diagnosis (to detect and treat disease early -- pap smear, HIV testing, occult blood screening) - deals with people without apparent disease state (preclinical) and those with manifest early clinical disease. Tertiary -- aims to minimize disability and restore function and productivity of patient (renal dialysis); - includes rehabilitation and palliative care. - deals with people in early to advanced clinical disease states. Public health will work mainly at the primary prevention level, but with some secondary preventive activities. Community health will work mainly at the secondary prevention level but with some primary preventive services.")
69
What are the differences between health promotion and disease prevention?
Health -absence of disease & medical model Aimed at high-risk groups One-shot strategy Strategies focus on individuals and groups Responsibility of health professionals Health Promotion Health – positive and multi-dimensional concept & participatory model of health Aimed at total population in it’s environment Many strategies and sectors

70
What are the differences between health promotion and disease prevention?
Language focus – deficits Goal – problem prevention People as problems Eurocentric Strategy – program, content External control Philosophy – control Meets bureaucratic needs Feelings despair Health Promotion Language focus – assets, strengths Goal – healthy development People as resources Multicultural, inclusive Strategy – people, places Internal control Meets peoples’ needs Feelings hope, motivation

71
Population Health & Health Promotion: Conceptual Differences
Focus on action – strategies for health Health ‘for the sake of’ health Grassroots, community oriented action Focus on qualitative or self-perceived indicators of health Population Health Conceptual framework for action and understanding Gone political – links to economy & productivity Influence agenda of policy and decision makers Focus on epidemiology & physiological processes to quantify determinants of health

72
Health promotion vs. Disease prevention
Tensions between two are NOT irreconcilable Needs reorientation of planners of top-down programs Systematically consider community empowerment goals within planning framework To “unpack” health promotion at each stage of planning, implementation, evaluation To unpack empowerment at each stage of planning – need to ask specific questions Objective setting – How are the programme objectives and community empowerment objectives accommodated together within the programme? Lavarack, & Labonte, 2000, Health Policy and Planning, 15 (3),
,")
73
Key Differences between down-stream and up-stream approaches
Root/metaphor Approach/ orientation Defn of Problem Main methods to effect change Role of outside agents

74
Key Differences between down-stream and up-stream approaches Lavarack, & Labonte, 2000
Main decision makers Community control of resources Community ownership evaluation

75
Health promotion strategies used in community nutrition…
Environmental Measures Health Education Advocacy Mass Comm./ Social Marketing Health Promotion Strategies Policy/ Legislation Self-help / Mutual Aid Economic Support Comm. Organization (Obert, 1986 in Davis, 1989)
")
76
What is Public Health? Protect & restore health through application of science, practical skills & collective actions. Scope includes Infectious diseases Chronic diseases Accidents READ defn DEFN – focuses on protecting and promoting people's health through actions of society -- health promotion, e.g., increasing F/V consumption, reducing tobacco exposure, promote healthy weights attitudes/behaviours -- health protection -- e.g., food safety issues - protection of the safety of the food supply through Food and Drugs Act, reduce consumption of known contaminants in foods -- posting notices re: contaminated shellfish or training for safe food handling -- prevention -- reduce risk of chronic disease and disability (CVD, CA, osteoporosis), reducing incidence of LBW babies through high risk prenatal program. -- surveillance and data systems -- information gathering on causes of death and disability (CVD #1 killer in Canada), surveys of food consumption patterns (Nutrition Canada ; provincial surveys - NS Nt Survey of early ‘90s);
, reducing incidence of LBW babies through high risk prenatal program. -- surveillance and data systems -- information gathering on causes of death and disability (CVD #1 killer in Canada), surveys of food consumption patterns (Nutrition Canada ; provincial surveys - NS Nt Survey of early ‘90s);")
77
What is Public Health? Looks at person BEFORE he/she becomes a patient – Upstream Approach Strategies focused on: Health promotion optimal health Health protection exposure to known contaminants Disease/accident prevention risk of chronic disease/disability/accidents Surveillance and data systems patterns of behaviours/attitudes While walking along the banks of a river, a passerby notices that someone in the water is drowning. After pulling the person ashore, the rescuer notices another person in the river in need of help. Before long, the rier is filled with drowning people, and more rescuers are required to assist the initial rescuer. Unfortunately, some people are not saed, and some victims fall back into the rivver after they have been pulled ashore. At this time, one of the rescuers starts walking upstream. “Where are you going?” the other rescuers ask, disconcerted. The upstream rescuer replies, “I’m going upstream to see why so many people keep falling into the river.” As it turns out, the bridge leading across the river upstream has a hole through which people are falling. The upstream rescuer realizes that fixing the hole in the bridge will prevent many people from ever falling into the river in the first place. FROM p. 4-5, Prevention is Primary. Strategies for community well-being. Cohen, Chavez, Chehimi (2007)
")
78
Public Health & Community Nutrition
Assesses needs Plans, organizes, manages, directs, coordinates & evaluates nt services Establishes linkages These defns differ from those in the text -- difference in American and Canadian perspectives and semantics PHNutrition (from ADA, Self-assessment tool for public health nutritionists -- generally refers to the larger picture while Community Nutrition refers to the more specifically targeted programs Now lets look at the Australian defn -- (from Hughes, R & Somerset S (1997). Definitions and conceptual frameworks for public health and community nutrition: A discussion paper. Australian Journal of Nutrition and Dietetics, 54(1),
. Definitions and conceptual frameworks for public health and community nutrition: A discussion paper. Australian Journal of Nutrition and Dietetics, 54(1),")
79
Public Health & Community Nutrition
Art & science of promoting population health status via sustainable & equitable improvements in the food & nutrition system Based on public health principles comprehensive and collaborative activities inter-sectoral in scope Again, this defn gives the population focus -- broader community --

80
Public Nutrition Roots: food insecurity & malnutrition in developing countries Developed countries: slow progress to improve nutrition of large population segments obesity, diabetes, CVD, nutrition related cancers, food insecurity Address population not individual levels - first appeared in literature in mid 1990’s - despite all the advances in biological knowledge accumulated over the last decades there is worldwide ever more increases in …

81
Population Health & Public Nutrition
Population Health Approach Public Nutrition Approach Focus on the health of population Focus on the nutrition of populations Address the determinants of health and their interactions Address the determinants of nutrition and their interactions Demonstrate accountability for health outcomes Demonstrate accountability for nutrition outcomes

Similar presentations




















 Overview of Social Determinants of Health Dennis Raphael School of Health Policy and Management York.>")