Download presentation
Presentation is loading. Please wait.

1
PANCAP RCM 25 March 2010 Report of the Priority Areas Coordinating Committee (PACC) Meeting of 24 March 2010
 Meeting of 24 March 2010")
2
Priority Areas Coordinating Committee (PACC) Terms of Reference Strategic management and technical oversight of the Caribbean Regional Strategic Framework (CRSF) Primary task of 24 March 2010 meeting: Review the documentation for the PANCAP proposal to Global Fund Round 9
 Terms of Reference Strategic management and technical oversight of the Caribbean Regional Strategic Framework (CRSF) Primary task of 24 March 2010 meeting: Review the documentation for the PANCAP proposal to Global Fund Round 9")
3
Caribbean Regional Strategic Framework (CRSF) Vision “To substantially reduce the spread and impact of HIV in the Caribbean by 2012 through sustainable systems of Universal Access to HIV Prevention, Treatment, Care and Support”
 Vision To substantially reduce the spread and impact of HIV in the Caribbean by 2012 through sustainable systems of Universal Access to HIV Prevention, Treatment, Care and Support")
4
CRSF Goals 1.By 2012, to reduce the estimated number of new HIV infections by 25% 2.By 2012, to reduce mortality due to HIV by 25% 3.To reduce the social and economic impact of HIV and AIDS on households

5
Guiding Principles Political leadership Countries at the center Multisectoral approach Inclusiveness and GIPA Equity Human rights Evidence-based Sustainability

6
Strategic Approaches Regional Public Goods and Services Multisectoral response Prevention Strengthening heath systems Monitoring all that is done

7
Regional Public Goods & Services Those Goods and Services that are more efficient to provide at regional level e.g. the development of regional guidelines and protocols some training programs procurement of ARVs – OECS CAREC – special tests

8
Priority Areas of the CRSF 1.An enabling environment 2.Prevention of HIV transmission 3.Treatment, care and support 4.An expanded multisectoral response 5.Capacity development 6.Monitoring, evaluation and research

9
PANCAP Proposal to GF Round 9 - Objectives 1.To create an enabling environment that fosters universal access to HIV services 2.To reduce HIV transmission in vulnerable populations 3.To lower morbidity and mortality among PLHIV in the OECS 4.To improve human and laboratory services for health system strengthening 5.To provide better information on the epidemic and the response

10
Challenges facing PANCAP To better integrate HIV services with other programs and sectors To build sustainable capacity to continue services after project funds end To significantly reduce new HIV infections – Need to develop the infrastructure for HIV prevention To ensure that activities have the impact that is required to reduce the epidemic and sustain the response

11
PACC Report on Global Fund Round 9 Grant Negotiation Documents 25 March 2010 PANCAP RCM

12
Toward Global Fund Grant Signing Preparation of four key documents Performance Framework M&E Plan Workplan and Budget Procurement Plan March 31 – First version to Global Fund May – Revised version

13
Main Items Based on Proposal (no major changes) M&E: Indicators sharpened, measurement defined, data collection & mgmt => SR Plans Performance Framework: legal commitment; fewer indicators, mostly output level
 M&E: Indicators sharpened, measurement defined, data collection & mgmt => SR Plans Performance Framework: legal commitment; fewer indicators, mostly output level")
14
Main Items Workplan and Budget – Focus on outputs, bang for buck – Budget cut 11% (PR and SRs cut 3%-30%) – New per diem policy (GTZ - based) – Process: deeper cuts, then put some back in critical areas to ensure capacity to implement
 – New per diem policy (GTZ - based) – Process: deeper cuts, then put some back in critical areas to ensure capacity to implement")
15
Objectives 1.An enabling environment that fosters universal access to HIV services. 2.Reduced HIV transmission in vulnerable populations 3.Lower PLH morbidity and mortality (in the OECS) 4.Improved laboratory and human resources (health systems strengthening). 5.Better information on the epidemic & the response.
 4.Improved laboratory and human resources (health systems strengthening). 5.Better information on the epidemic & the response..")
16
Performance Framework

17
Impact Indicators % of young women aged 15-24 who are HIV infected (UNGASS 22) – 10% fewer: prevalence from average of 0.97 (2008) to 0.87 (2014) % of most at-risk populations (FSW and MSM) who are HIV-infected (UNGASS 23) – 10% lower: avg. FSM prevalence from 13.5% (2008) to 12.2% (2014) avg. MSM prevalence from 15.8% (2008) to 14.4% (2014)
 to 12.2% (2014) avg. MSM prevalence from 15.8% (2008) to 14.4% (2014).")
18
Outcome Indicators Number of countries with 70% of FSW reporting condom use with last client (based on UNGASS 18). [10, up from 5 in 2008] Number of countries informing that 70% of MSM report use of a condom the last time they had anal sex with a male partner (based on UNGASS 19). [10, up from 5 in 2008] Both baselines to be re-set with 2010 UNGASS data
. [10, up from 5 in 2008] Both baselines to be re-set with 2010 UNGASS data.")
19
Performance Framework Output Indicators Objective 1. An enabling environment that fosters universal access to HIV services Number of PLH from project countries trained in Peer Education (150 in 2 years) Number of PANCAP governance body meetings organized and reported on: RCM, PACC, and AGM. (8 in 2 years)
 Number of PANCAP governance body meetings organized and reported on: RCM, PACC, and AGM. (8 in 2 years).")
20
Performance Framework Output Indicators Objective 2. Reduced HIV transmission in vulnerable populations # of peer educators trained: FSW; MSM # of persons reached by peer educators: FSW; MSM # of stakeholders sensitized to MARPS issues as defined by needs of MSM, FSW populations # of NAC/CCM affiliations of regionally networked MARP entities (FSW, MSM, MY, or DU) in target countries.
 in target countries..")
21
Performance Framework Output Indicators Objective 3. Lower PLH morbidity & mortality Number of adults and children with advanced HIV infection that receive ART in the OECS states

22
Objective 4. Improved laboratory and human resources (Health Systems Strengthening) Target: HIV+ and other health system users 1.Quality in-service training for 6,000 health workers on a range of fields. UWI, $1.4 M 2.Leadership and management skills for NAP coordinators, key health service staff, others. UWI, $1.0 M 3.Improve access to quality assured, reliable, affordable lab services CMLF-CCAS, $1.9 M
 Target: HIV+ and other health system users 1.Quality in-service training for 6,000 health workers on a range of fields. UWI, $1.4 M 2.Leadership and management skills for NAP coordinators, key health service staff, others. UWI, $1.0 M 3.Improve access to quality assured, reliable, affordable lab services CMLF-CCAS, $1.9 M.")
23
Performance Framework Output Indicators Objective 4. Improved laboratory and human resources (Health Systems Strengthening) # of health care workers receiving in-service training # of persons enrolled in Caribbean Health Leadership Institute (CHLI) programme # of countries accessing selected laboratory services (CD4, PCR, viral load, etc.) and meeting agreed turnaround and quality standards
 # of health care workers receiving in-service training # of persons enrolled in Caribbean Health Leadership Institute (CHLI) programme # of countries accessing selected laboratory services (CD4, PCR, viral load, etc.) and meeting agreed turnaround and quality standards.")
24
Objective 5. Better information on the epidemic and the response Target: country level M&E, policy makers, managers, MARP & PLHIV groups, & other users of evidence 1.Technical support for M&E of NSP using agreed tools and standardized data collection for regional reporting. 2.Develop capacity & conduct evaluations of health sector M&E response in 5 countries and one pilot evaluation of an education sector response. 3.Develop in-region capacity and conduct evaluation of country responses at the end of each NSP (each 5 years, with input of peers). All CHRC, $1.5 M
. All CHRC, $1.5 M.")
25
Performance Framework Output Indicators Objective 5. Better information on the epidemic and the response # of countries with a national HIV Monitoring Evaluation Plan in place based on agreed guidelines # of countries that report at least 16 of 22 UNGASS Indicators

26
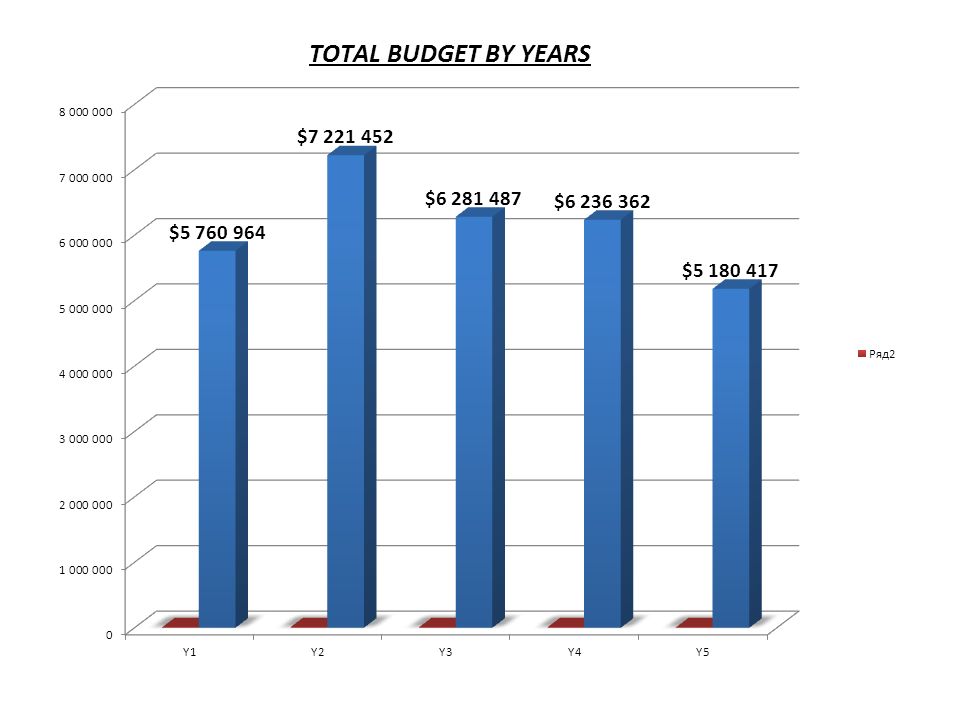
Workplan / Budget

27
Main Changes to Budget Shift resources, activities back toward Phase 2 Cuts of 11.1% (net, after first cutting deeper, then providing for missing capacities) More detail, greater consistency in costing
 More detail, greater consistency in costing")
28
Main Changes to Budget (2) PR built up Staff: management, financial, M&E M&E capacity: PMIS, training, travel to SRs Pre-signing activities 2% indirect cost / contingency Umbrella SRs built up -- COIN, PCU M&E and accounting staff Travel to oversee CPs Training for CP staff: M&E and financial reports
 PR built up Staff: management, financial, M&E M&E capacity: PMIS, training, travel to SRs Pre-signing activities 2% indirect cost / contingency Umbrella SRs built up -- COIN, PCU M&E and accounting staff Travel to oversee CPs Training for CP staff: M&E and financial reports")
29
Main Changes to Budget (3) M&E strengthening – Project Management Information System (PMIS) – Training of SRs, CPs – MESS -- M&E Systems Strengthening assessment – Harmonization, standardization of tools, protocols, templates – Advisory body based on TWG – Umbrella SR capacity building (staff, training, travel)
 M&E strengthening – Project Management Information System (PMIS) – Training of SRs, CPs – MESS -- M&E Systems Strengthening assessment – Harmonization, standardization of tools, protocols, templates – Advisory body based on TWG – Umbrella SR capacity building (staff, training, travel)")
34
Issue / Solution Governance / Steps to be taken: 1. Resources provided: Management: PR Admin to 8.8% ($2.7 M) Tracking : PR M&E to 10.9% ($3.3 M) 2. Structure: PR in charge of programme implementation, not just Admin 3. Integration: molding & steering of SRs 4. RCM / PACC: need tough oversight from first
 Tracking : PR M&E to 10.9% ($3.3 M) 2. Structure: PR in charge of programme implementation, not just Admin 3. Integration: molding & steering of SRs 4. RCM / PACC: need tough oversight from first.")
35
Issue / Solution HR size (35.7% of Phase 1): Appears bigger because of few ARVs Needed to 1) do prevention among MARPs 2) manage regional grant with independent agencies as SRs Tactic: see GF reaction before cutting further Plan B: switch some HR to consultants
: Appears bigger because of few ARVs Needed to 1) do prevention among MARPs 2) manage regional grant with independent agencies as SRs Tactic: see GF reaction before cutting further Plan B: switch some HR to consultants")
36
Next Steps Approval of RCM: minutes Incorporate comments: RCM, UNAIDS peer review Compilation of final printed & electronic versions 29-31 March Delivery to GF 31 March

37
Thank You

38
The Meeting is invited to: 1.Approve the documentation to be submitted to the Global Fund Round 9 2. Authorise the PACC to make whatever amendments are needed in the event of further changes being required by the Global Fund 3.Thank all those involved in the preparation of the PANCAP Global Fund Round 9 proposal ACTION REQUIRED BY THE RCM

Similar presentations













>")

 Support for GF proposals and grant implementation Improving access to timely, quality assured Technical Assistance.>")





