Download presentation
Presentation is loading. Please wait.

1
Shock: A State of Hypoperfusion
Chapter 9 Shock: A State of Hypoperfusion

2
Overview Hypoperfusion Causes of Hypoperfusion
Physiologic Response to Shock Assessment Management of Hypoperfusion Activity: Divide the class into groups of four to five students. Assign one or more groups to answer the questions in the case “Industrial Accident.” Assign one or more groups to answer the questions in the case “Pneumonia.” Bring the class back together and have each of the groups report on their responses. Suggested Responses to “Industrial Accident”: 1. If the patient’s bleeding continues unabated, he will become hypoperfused, leading to shock and eventually to death. 2. Initially the patient may complain of thirst and have pale, clammy skin. As the shock continues, his muscles, guts, and kidneys will shut down and shunt blood to the core organs. Eventually, if the bleeding continues, the patient’s heart will beat faster (tachycardia) and the patient will breathe faster (tachypnea). 3. Entanglement of an extremity is a surgical emergency. Surgical emergencies are best treated in a trauma center. When this patient is disentangled from the machinery, he should be transported immediately, with lights and siren, to a trauma center. Suggested Responses to “Pneumonia” 1. While the patient is not bleeding externally, fluids are being lost internally. This loss of fluid creates hypovolemia and then hypoperfusion. The cause of the fluid loss is infection (septic shock). 2. It is not unreasonable to think that an elderly woman whose body is stressed by any infection could have had a heart attack (myocardial infarction), leading to pump failure and hypoperfusion. While an EMT is not expected to come to this conclusion, the point emphasizes the importance of closely monitoring the patient and transporting her to the emergency department.
 and the patient will breathe faster (tachypnea). 3. Entanglement of an extremity is a surgical emergency. Surgical emergencies are best treated in a trauma center. When this patient is disentangled from the machinery, he should be transported immediately, with lights and siren, to a trauma center. Suggested Responses to Pneumonia 1. While the patient is not bleeding externally, fluids are being lost internally. This loss of fluid creates hypovolemia and then hypoperfusion. The cause of the fluid loss is infection (septic shock). 2. It is not unreasonable to think that an elderly woman whose body is stressed by any infection could have had a heart attack (myocardial infarction), leading to pump failure and hypoperfusion. While an EMT is not expected to come to this conclusion, the point emphasizes the importance of closely monitoring the patient and transporting her to the emergency department.")
3
Hypoperfusion Hypoperfusion means inadequate perfusion
Hypoperfused tissue is no longer being given enough oxygen and will stop working optimally All cells and organs within the body need oxygen to function optimally. When cells and organs receive inadequate levels of oxygen their function will be impaired and they may stop functioning altogether.

4
Hypoperfusion The brain is the most sensitive organ in the body to decreases in blood and oxygen supply After just a few seconds of no blood flow, the brain will cease to function optimally, resulting in loss of consciousness or other signs of neurologic compromise.

5
Causes of Hypoperfusion
Three basic components of the circulatory system can affect perfusion: Fluid Container Pump This simple description of cardiovascular anatomy and physiology is useful when identifying the causes of shock. The fluid of the cardiovascular system is the blood If there is not enough fluid (blood) to fill the container (blood vessels), hypoperfusion will result Hypovolemic and hemorrhagic shock are examples of shock resulting from a fluid problem
 to fill the container (blood vessels), hypoperfusion will result. Hypovolemic and hemorrhagic shock are examples of shock resulting from a fluid problem.")
6
Causes of Hypoperfusion
The fluid Hypoperfusion will occur if There is not enough blood in the system The blood in the system is not carrying enough oxygen The fluid of the cardiovascular system is blood. Alterations in the amount of blood within the system or the oxygen carrying capacity of blood within the system may result in hypoperfusion.

7
Causes of Hypoperfusion
Hypovolemic shock When body fluids are lost and not adequately replenished, the total body fluid volume is low When shock results from an actual loss of blood, it can be specifically called hemorrhagic shock Other means of fluid loss are excessive vomiting, diarrhea, sweating, or urinating Hypovolemic shock results when body fluids are lost and not adequately replenished. The condition of low fluid volume is described as hypovolemia. This can be the result of a loss of blood, or fluids lost through vomiting, diarrhea, or sweating.

8
Causes of Hypoperfusion
The container Blood vessels have the ability to significantly alter their diameter by contraction or relaxation of the smooth muscles in their walls This can be harmful in some circumstances, such as anaphylactic, septic, or neurogenic shock Blood vessels are able to constrict narrowing the size of the vessel or dilate widening the size of the vessel. Alteration in the size of the blood vessels will alter the total capacity of the system. The blood vessels’ ability to change their size can be very advantageous; however, in the case of shock it can cause significant problems.

9
Causes of Hypoperfusion
Anaphylactic shock The result of a severe allergic reaction Causes vasodilation and subsequent hypotension Patient will have urticaria (hives), airway swelling, and hypotension During an anaphylactic reaction blood vessels close to the skin will dilate resulting in reddened areas of the skin, leakage of plasma from white blood cells will result in edema, blood vessels throughout the system can dilate causing an increase in the capacity of the system resulting in a drop in pressure. Anaphylactic shock can cause pronounced hypotension. The EMT’s goal is to reverse these affects of the reaction.
, airway swelling, and hypotension. During an anaphylactic reaction blood vessels close to the skin will dilate resulting in reddened areas of the skin, leakage of plasma from white blood cells will result in edema, blood vessels throughout the system can dilate causing an increase in the capacity of the system resulting in a drop in pressure. Anaphylactic shock can cause pronounced hypotension. The EMT’s goal is to reverse these affects of the reaction.")
10
Causes of Hypoperfusion
Septic shock Severe infection may lead to generalized blood vessel dilation, with a drop in blood pressure and diminished perfusion Certain types of bacteria can produce toxins that prevent the vessels from constricting appropriately, causing them to leak Septic shock is the result of severe infection. In this form of shock the blood vessels also dilate and cause an increase in the capacity of the system which in turn lowers blood pressure within the system. The patient with septic shock may present with flushed and warm skin. The EMT should transport this patient to the hospital for definitive treatment.

11
Causes of Hypoperfusion
Neurogenic shock Is caused by a loss of control of the smooth muscles in the vessel walls May occur as a result of spinal cord injury where the vessels no longer have the ability to constrict when appropriate Also termed spinal shock Hypoperfusion resulting from spinal cord injury and disruption of the nerve control to the blood vessels is called neurogenic shock. Neurogenic shock may occur as a result of spinal cord injury where the vessels no longer have the ability to constrict when appropriate; all of the vessels supplied by the injured nerves will dilate. This in turn increases the capacity of the system and lowers blood pressure.

12
Causes of Hypoperfusion
The pump Inadequate pumping action of the heart can result in hypoperfusion If the pump does not have enough power to generate adequate forward flow, the amount of blood pumped will be smaller The smaller volume will result in a lower cardiac output Another main cause of hypoperfusion is problems with the pump (heart). At times the heart is not able to pump adequate amounts of blood due to disease processes or traumatic injuries.
. At times the heart is not able to pump adequate amounts of blood due to disease processes or traumatic injuries.")
13
Causes of Hypoperfusion
Cardiogenic shock If the heart muscle is damaged, as during a heart attack, it does not pump to full capacity Shock that results from inadequate cardiac pumping is called cardiogenic shock Cardiogenic shock will often result from damage to the heart muscle resulting from a heart attack. The EMT should attempt to improve oxygenation. The patient suffering from cardiogenic shock benefits from timely care and transport to a hospital.

14
Physiologic Response to Shock
Compensated shock The body attempts to compensate for hypoperfusion by: Increasing the volume of blood pumped with each stroke or the heart rate Increasing respiratory rate Adjusting blood flow to only core areas (shunting) When the body recognizes hypoperfusion, it responds to it in several ways to compensate. Increasing either the volume of blood pumped with each stroke or the heart rate to maximize the available blood supply Increasing respiratory rate to improve oxygenation of the blood Adjusting blood flow to only core areas (shunting); this is accomplished by constricting arteriolar circulation in certain areas. Blood flow to the skin is sacrificed first, followed by blood flow to the abdominal organs. Blood flow to the heart and lungs is maintained until shock is profound. Blood flow to the brain is maintained at all costs.
 When the body recognizes hypoperfusion, it responds to it in several ways to compensate. Increasing either the volume of blood pumped with each stroke or the heart rate to maximize the available blood supply. Increasing respiratory rate to improve oxygenation of the blood. Adjusting blood flow to only core areas (shunting); this is accomplished by constricting arteriolar circulation in certain areas. Blood flow to the skin is sacrificed first, followed by blood flow to the abdominal organs. Blood flow to the heart and lungs is maintained until shock is profound. Blood flow to the brain is maintained at all costs.")
15
Physiologic Response to Shock
Compensated shock Signs and symptoms Pale Cool Clammy Weakening peripheral pulses Elevated heart rate Elevated respiratory rate Nausea Altered mental status If the EMT knows how the body compensates for hypoperfusion, he can recognize the extent of a patient’s illness by a careful examination.

16
Physiologic Response to Shock
Decompensated shock Systolic blood pressure drops to less than 90 mm Hg The body is no longer able to compensate for an event When hypotension is noted, the patient is considered to be in decompensated shock and must be aggressively managed for survival to be possible Once systolic blood pressure drops to less than 90 mm Hg, the condition is termed decompensated shock. Decompensated shock will lead to multiple organ failure and death unless the source of the problem is quickly corrected and the hypoperfused state reversed.

17
Physiologic Response to Shock
Irreversible shock Prolonged periods of decompensated shock resulting in the failure of multiple organs Patients with irreversible shock often do not survive If multiple body organs are without oxygen for enough time to cause permanent damage, the patient is unlikely to have a good outcome.

18
Stop and Review What is hypoperfusion?
What are the three main causes of hypoperfusion? List the signs and symptoms associated with compensated shock. What is the tell-tale sign of decompensated shock? Refers to inadequate blood flow and oxygenation of body tissues and organs. Hypoperfusion is caused by a loss of fluid volume, increase in capacity of the system without an increase in capacity of fluid volume, and failure of the heart to pump adequately. The signs and symptoms of compensated shock are: Pale Cool Clammy Weakening peripheral pulses Heart rate will be elevated Respiratory rate will be elevated Nausea Altered mental status 4. When the patient is hypotensive the patient is no longer able to compensate and is in decompensated shock.

19
Assessment In assessing a patient, be careful to look for signs of compensated shock If you don’t look for it, you won’t find it It is necessary to begin to treat the patient in shock before she decompensates and becomes hypotensive Treating for shock early before signs and symptoms become obvious is preferred. It is not good practice to wait until signs of hypotension develop to confirm a diagnosis of shock.

20
Assessment The look test Ensure your own safety and adequate PPE
Form general impression The EMT will base his immediate priorities in patient care and scene management on this initial impression of the patient.

21
Assessment Mental status ABCs Assess for AVPU
Once ABCs have been assessed, look for signs of hypoperfusion Assess the patient’s mental status. The patient who is able to communicate is not experiencing any alterations in brain function. Assess the patient’s airway, breathing, and circulation. Look for signs of hypoperfusion.

22
Assessment Vital signs Orthostatic vital signs
Obtain a complete set of vital signs Orthostatic vital signs Vital signs measured in two different positions Positive tilt test Vital signs measured in two different positions are called orthostatic vital signs. Orthostatic vital signs are useful for determining borderline shock patients. Vital signs are taken lying and then standing.

23
Management of Hypoperfusion
The treatment of shock is geared toward restoring adequate oxygenation, ventilation, and circulation The EMT must maximize perfusion while rapidly transporting the patient to a hospital, where definitive treatment will be available Most patients with signs of hypoperfusion have conditions that are not definitively treated by BLS. These patients should be transported as a high priority patient. A call to have an ALS intercept meet the crew en route would be advisable.

24
Management of Hypoperfusion
Oxygen Apply high-flow 100% oxygen in any stage of shock Control bleeding Locate source of bleeding and control it in whatever way possible Trendelenburg Elevate the legs and utilize the force of gravity to increase the blood volume in the thorax and abdomen Using oxygen, controlling bleeding, and placing the patient in Trendelenburg position are effective BLS means to manage hypoperfusion.

26
Management of Hypoperfusion
MAST/PASG Military anti-shock trousers or a pneumatic anti-shock garment A device that may support blood pressure in certain circumstances MAST/PASG improves the blood supply to the upper body and vital organs MAST/PASG improves the blood supply to the upper body and vital organs. It is separated into three sections that may be individually inflated to support blood pressure.

27
Management of Hypoperfusion
MAST/PASG Indications Severe hypotension (systolic BP less than 50 mm Hg Hypotension (systolic BP less than 90 mm Hg) because of severe pelvic injuries Use of MAST/PASG is controversial, and its use is debated in the medical literature. Consult local protocols and read the NAEMSP position paper entitled “Use of Pneumatic Anti-Shock Pants.”
 because of severe pelvic injuries. Use of MAST/PASG is controversial, and its use is debated in the medical literature. Consult local protocols and read the NAEMSP position paper entitled Use of Pneumatic Anti-Shock Pants.")
28
Management of Hypoperfusion
MAST/PASG Contraindications (absolute) Penetrating thoracic injury Pulmonary edema Do not use PASG in cases of penetrating thoracic injury or pulmonary edema. Use of this device in these circumstances can worsen the patient’s condition.
 Penetrating thoracic injury. Pulmonary edema. Do not use PASG in cases of penetrating thoracic injury or pulmonary edema. Use of this device in these circumstances can worsen the patient’s condition.")
29
Management of Hypoperfusion
MAST/PASG Contraindications (relative) Pregnancy Penetrating object Evisceration The abdominal section is not inflated for the pregnant patient or the patient with an evisceration.
 Pregnancy. Penetrating object. Evisceration. The abdominal section is not inflated for the pregnant patient or the patient with an evisceration.")
30
Management of Hypoperfusion
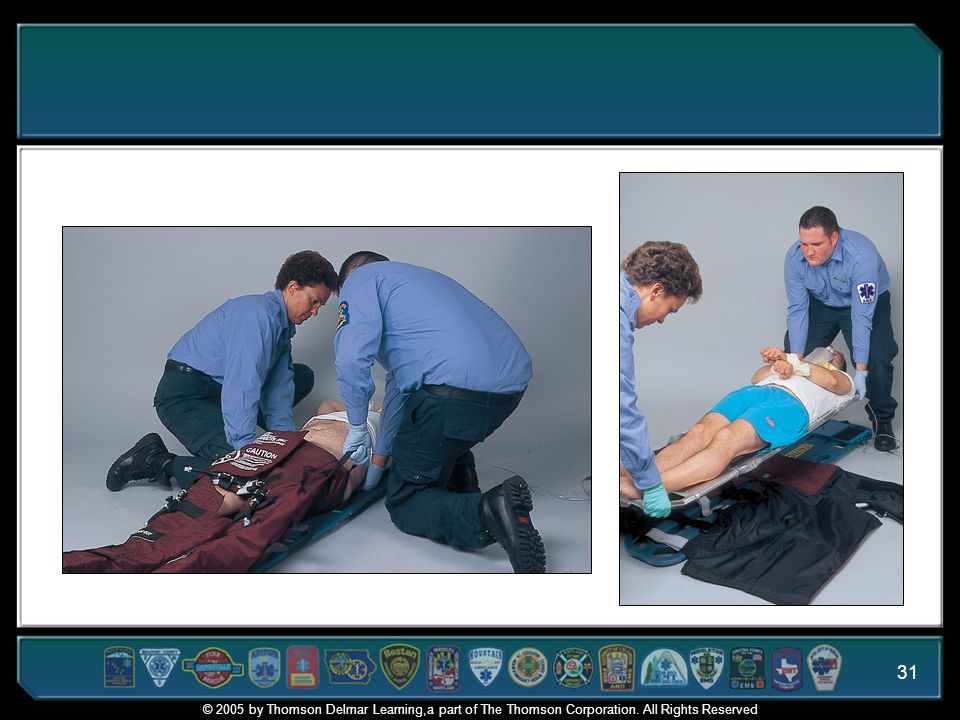
MAST/PASG Application Trouser method Wrapper method After completing the necessary evaluation of the patient, the actual technique of applying the MAST/PASG (such as the trouser method or wrapper method) is an individual choice. The goal is to apply the device quickly with minimal movement of the patient. Review Skill 9-2: Application of MAST/PASG in the textbook.
 is an individual choice. The goal is to apply the device quickly with minimal movement of the patient. Review Skill 9-2: Application of MAST/PASG in the textbook.")
32
MAST/PASG Watch this video clip demonstrating the use of MAST/PASG

33
Management of Hypoperfusion
MAST/PASG Removal Should never be deflated by the EMT Physicians should be familiar with the procedure of slow deflation Gradual process Removal should not be attempted outside of the hospital unless specifically ordered by the physician.

34
Management of Hypoperfusion
Reduce heat loss Prevent excessive heat loss during the evaluation and treatment of the critically ill or injured patient Cover the patient with blankets once the assessment has been completed Additional heat loss of the hypoperfused patient complicates treatment. Keep the patient wrapped in a blanket to prevent heat loss from occurring.

35
Management of Hypoperfusion
Transport Consider ground or air transport Reassess patient frequently and monitor vital signs every five minutes Consider ALS intercept Consult local protocols The patient should be transported to the nearest hospital capable of managing shock in a timely manner. Patients in shock may deteriorate rapidly so vital signs should be reassessed frequently. ALS can provide more advanced treatments to prevent decompensation.

36
Stop and Review What can the EMT do to manage the patient presenting with shock? What are the absolute contraindications for using PASG/MAST? 1. The EMT should concentrate on the ABC’s and provide 100% high concentration oxygen while transporting the patient to a trauma center. If the patient is bleeding; bleeding should be controlled. An ALS intercept can be of benefit to the patient and should be considered. 2. Pulmonary edema and penetrating thoracic trauma.

Similar presentations



















 leading to inadequate oxygen delivery to tissues.>")