Download presentation
Presentation is loading. Please wait.

1
EXCRETORY SYSTEM

2
Function Disposes of wastes & excess ions
Regulates volume & chemical makeup of blood by maintaining proper balance between water & salts, acids & bases UREA

3
Produces renin to regulate blood pressure & kidney function
Produces erythropoietin to stimulate RBC production in bone marrow Metabolizes vitamin D to its active form

4
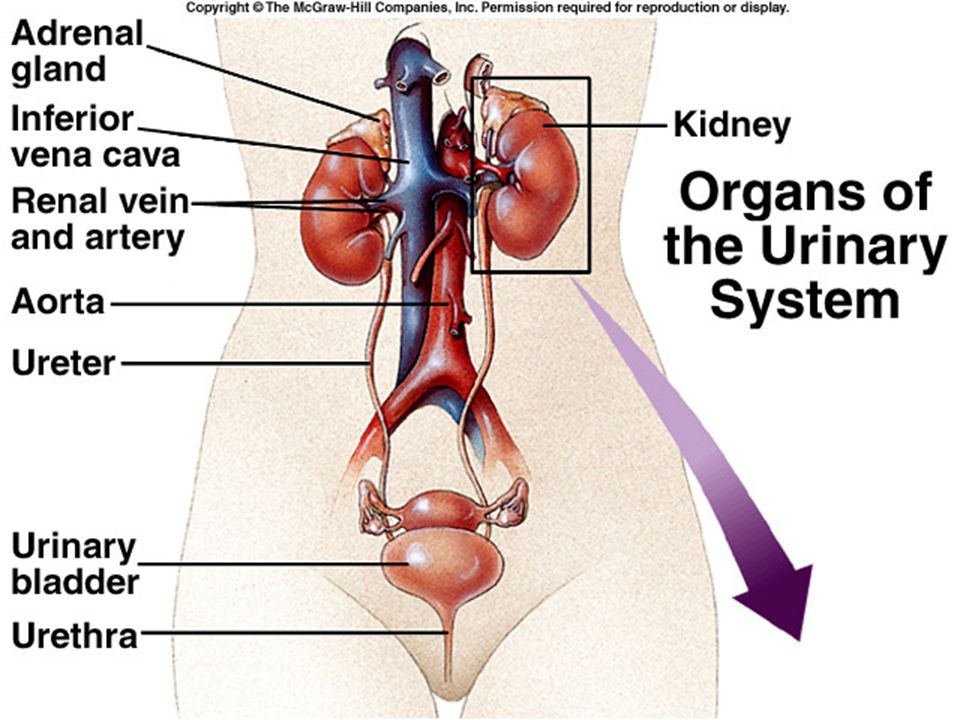
Organs Kidneys Ureters Urinary Bladder Urethra

6
Anatomy of Kidney Bean-shaped
Located between 12th thoracic vertebra and 3rd lumbar vertebra (partial protection) Rt. kidney lies lower than left Concave cleft on medial surface called- hilus which leads to the renal sinus
 Rt. kidney lies lower than left. Concave cleft on medial surface called- hilus which leads to the renal sinus.")
7
Adrenal Glands lie on top of each kidney

8
External anatomy surrounded by renal capsule (protects from surrounding infection and trauma), adipose capsule (holds kidneys in place and protects from trauma), renal fascia (anchors).
, renal fascia (anchors).")
9
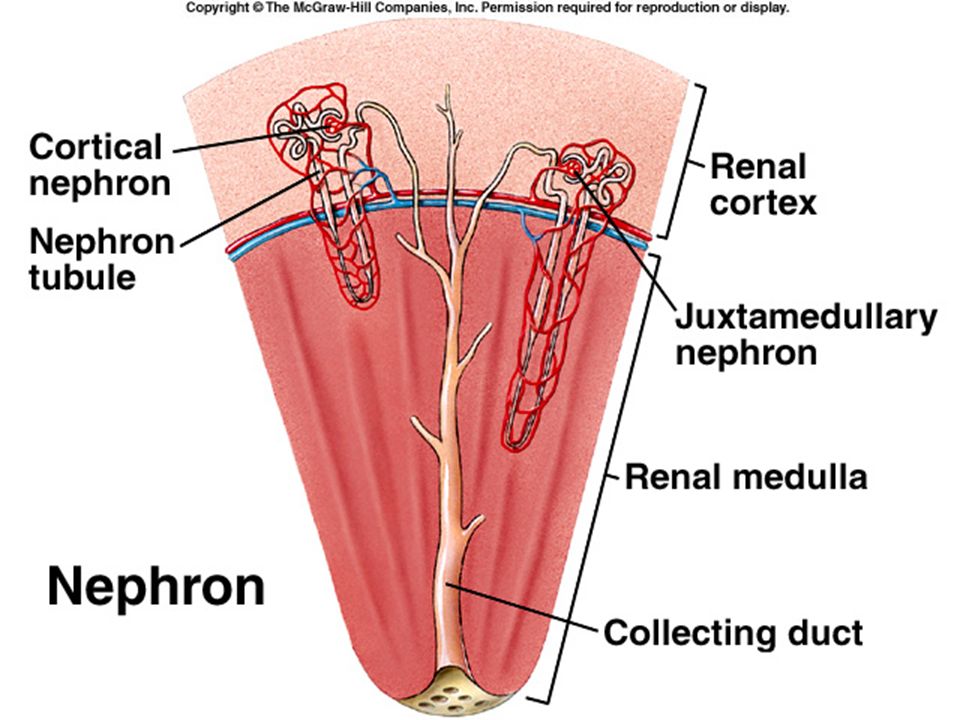
Internal anatomy renal cortex - outer region renal medulla - inner region with cone shaped renal pyramids renal columns separate pyramids renal pelvis - continuous with the ureter leaving the hilus major and minor calyces

10
Renal column Renal pyramid Renal calyx

11
Blood and Nerve Supply renal arteries - deliver 1/4 total cardiac output to kidneys per minute lobar arteries interlobar arteries arcuate arteries Interlobular arteries

12
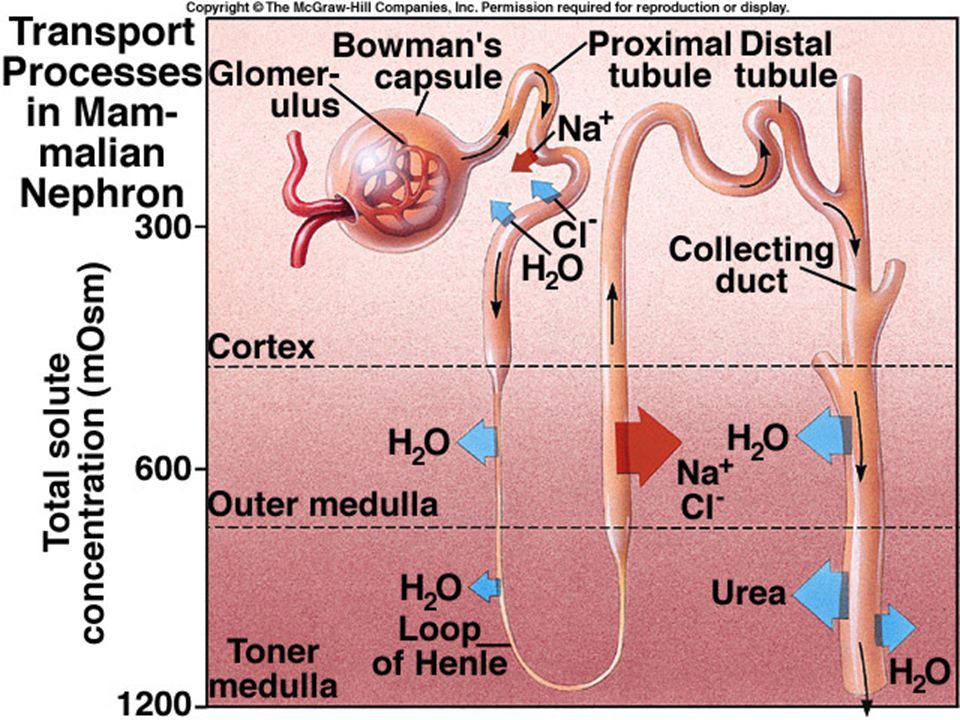
Nephron (this is where the action is!)
Interlobar, Interlobular, Arcuate, Lobar, Renal veins Renal Plexus – sympathetic nerve fibers

13
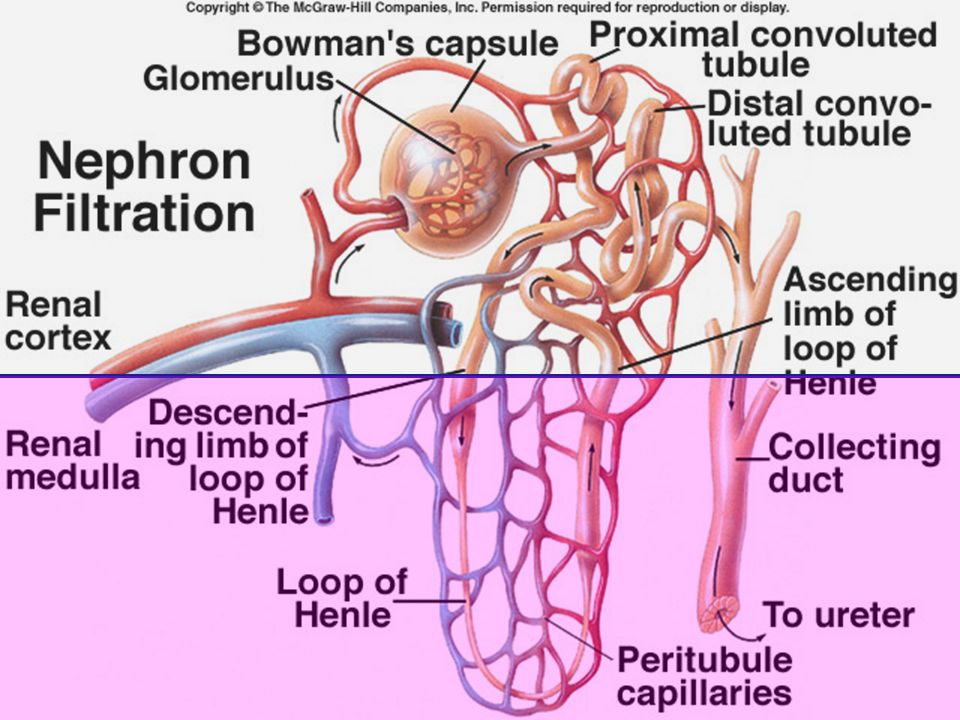
Nephron over 1 million/ kidney; filtering unit of kidney; results in production of urine

14
renal corpuscle - consisting of glomerulus,
Bowman's capsule proximal convoluted tubule (PCT) loop of Henle
 loop of Henle.")
15
distal convoluted tubule (DCT)
collecting tubule (urine collecting duct) papillary ducts (collection of all collecting tubules)
 papillary ducts (collection of all collecting tubules)")
16
Nephron

17
Bowman’s Capsule PCT DCT Loop of Henle Collecting Tubule Renal artery

18
7. Renal vein 8. Interlobular artery 9. Afferent artery 10. Glomerulus 11. Efferent artery 12. Peritubule capillaries

21
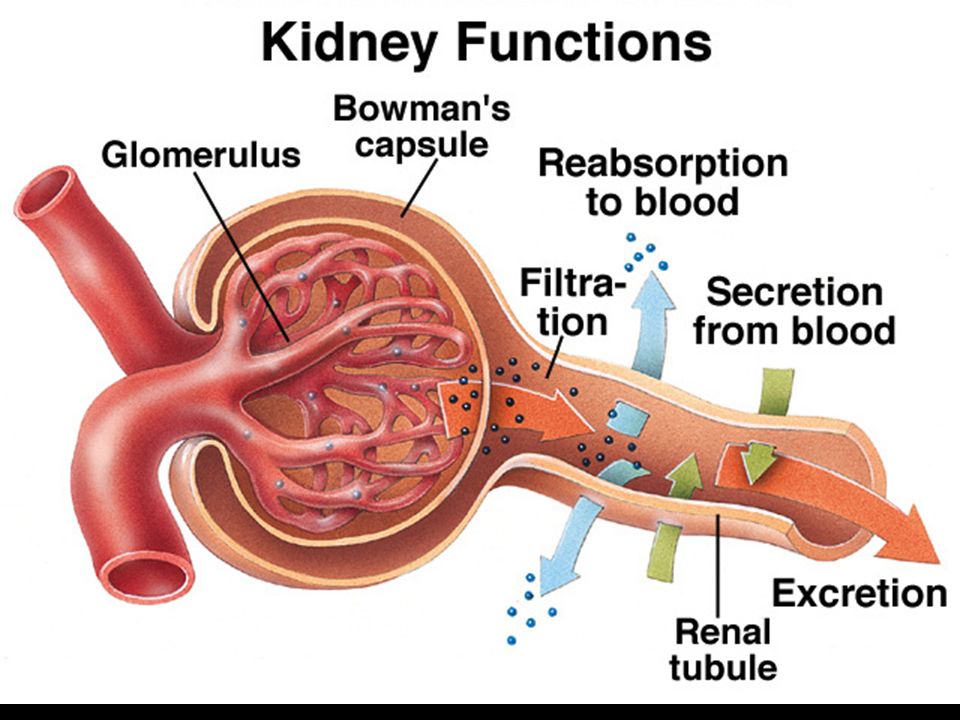
Kidney Physiology 3 Steps involved in kidney filtration
Glomerular Filtration Passive Mechanical

22
based on hydrostatic pressure
enhanced by permeability of filtration membrane filtration membrane consists of 3 layers

24
porous endothelium - prevents passage of cells & large proteins
thin basement membrane – charged to repel charged proteins

25
visceral membrane with slit-like openings; prevents passage of large plasma proteins
Net Filtration Pressure – Glomerular hydrostatic pressure + Bowman's hydrostatic pressure (opposing forces)
")
26
Filtration Rate: rate at which fluid
is forced from blood into Bowman's capsule; dependent upon: - surface area - filtration membrane permeability - Net filtration pressure

27
Glomerular filtration rate
is proportional to Net filtration pressure anything changing pressure at the membrane also changes the GFR, therefore higher blood pressure = higher GFR; dehydration = lower GFR

28
Tubular Reabsorption - reclamation of tubule contents
difference b/t filtrate & urine filtrate - everything in blood plasma except proteins & cells urine - wastes & unneeded substances

29
reclamation begins in PCT (both active/passive transport)
active - glucose; a.a., vit, Na, Ca, Cl, K, P,; most require a carrier molecule. When all carrier molecules are bound, excess are excreted into urine

30
passive - (diffusion, osmosis)
usually tied to active transport of Na other anions move with Na to balance charges in the blood. The anions that move depend on the blood pH H2O moves passively (osmosis) due to its linkage to Na+
 due to its linkage to Na+")
31
solvent drag occurs when filtrate becomes concentrated & solvent follows the concentration gradient back into the body Explains why some drugs & toxins are not excreted easily

32
Nonreabsorbed substances Urea (40% reabsorbed) Creatine uric acid
Tubule absorption capabilities PCT most reabsorption occurs here Uric Acid

33
DCT permeable to Na but not H2O urine concentration determined here
dependent on blood pressure or volume dependent on hormone release:

34
aldosterone - increases Na reabsorption & therefore H2O
ANF - opposes this sex hormones glucocorticoids

35
Tubular Secretion – Reabsorption in reverse
ammonia (secreted into the collecting tubule from the blood) Active process Some drugs (penicillin)
 Active process. Some drugs (penicillin)")
38
Pathology Suppression - holding back Pyuria - tract infection
Ptosis (hydronephrosis) - kinked ureter Pyelonephritis – kidney inflammation
 - kinked ureter. Pyelonephritis – kidney inflammation.")
39
Pyelitis - inflammation of pelvis
Anuria - no output due to low pressure Urethritis - inflammation of urethra Cystitis- inflammation of bladder

40
Dysuria- painful urination
Incontinence - sphincter control Retention - involuntary suppression Diabetes insipidus – lack of ADH Addison's Disease – not enough aldosterone Excess Cl – indicate stone formation

41
Excess phosphates - alkaline urine
Cushing's Disease - hyperaldosteronism Dehydration – low GFR Hypotonic hydration – “water intoxication”; Hyponatremia, too much ADH Renal calculi – kidney stones

Similar presentations













 System>")





