Download presentation
Presentation is loading. Please wait.

1
WHY MIGHT THE WORLD FACE AN OVERPOPULATION PROBLEM? Chapter 2 Key Issue 4

2
MALTHUS ’ THEORY OF POPULATION GROWTH In 1798 Thomas Malthus published his views on the effect of population on food supply. His theory has two basic principles: Population grows at a geometric rate i.e. 1, 2, 4, 16, 32, etc. Food production increases at an arithmetic rate i.e. 1, 2, 3, 4, etc.

3
MALTHUS (CONT.) The consequence of these two principles is that eventually, population will exceed the capacity of agriculture to support the new population numbers. Population would rise until a limit to growth was reached. Further growth would be limited when: preventive checks - postponement of marriage (lowering of fertility rate), increased cost of food etc. positive checks - famine, war, disease, would increase the death rate.
, increased cost of food etc. positive checks - famine, war, disease, would increase the death rate..")
4
MALTHUS (CONT.) Population grows geometrically…. Population exceeds carrying capacity… Population is kept in “ check ” – preventative and/or positive checks

5
© Dr. Jean-Paul Rodrigue 2. The Malthusian Crisis ■The “ Malthusian crisis ” Available agricultural spaces are limited. Technical progresses (machinery, irrigation, fertilizers, and new types of crops) are slow to occur. Increasing incapability to support the population. If this persists, the population will eventually surpass the available resources. The outcomes are “ Malthusian crises ” : Food shortages. Famines. War and epidemics. “ Fix ” the population in accordance with available resources. Necessity of a “ moral restraint ” on reproduction.
 are slow to occur. Increasing incapability to support the population. If this persists, the population will eventually surpass the available resources. The outcomes are Malthusian crises : Food shortages. Famines. War and epidemics. Fix the population in accordance with available resources. Necessity of a moral restraint on reproduction..")
6
© Dr. Jean-Paul Rodrigue Overexploitation 2. The Malthusian Crisis Population Resources Technological Innovation Time Quantity t2 t3 t1

7
© Dr. Jean-Paul Rodrigue 2. The Malthusian Crisis ■The Malthusian Crisis has not occurred Malthus has been criticized on several accounts during the last 200 years. Religious view (Protestantism), racist and elitist. Did not foresee the demographic transition: Changes in the economy that changed the role of children in the industrializing societies. Failed to account for improvements in technology: Enabled food production to increase at rates greater than arithmetic, often at rates exceeding those of population growth. Enabled to access larger amounts of resources. Enabled forms of contraception.
, racist and elitist. Did not foresee the demographic transition: Changes in the economy that changed the role of children in the industrializing societies. Failed to account for improvements in technology: Enabled food production to increase at rates greater than arithmetic, often at rates exceeding those of population growth. Enabled to access larger amounts of resources. Enabled forms of contraception..")
8
© Dr. Jean-Paul Rodrigue Global Growth in Population and Grain (Wheat and Rice) Production, 1961-2005
 Production,")
9
ESTHER BOSERUP ’ S THEORY OF POPULATION GROWTH In contrast to Malthus, instead of too many mouths to feed, Boserup emphasized the positive aspects of a large population; In simple terms, Boserup suggested that the more people there are, the more hands there are to work; She argued that as population increases, more pressure is placed on the existing agricultural system, which stimulates invention; The changes in technology allow for improved crop strains and increased yields.

10
ANTI-POPULATIONISTS VS. PRONATALISTS Malthus– anti-populationist Echoed in recent debates by Paul Ehrlich, author of The Population Bomb; Ehrlich believed that the earth ’ s carrying capacity would quickly be exceeded, resulting in widespread famine and population reductions; Boserup– pronatalist (cornucopian) Echoed in recent debates by Julian Simon, who opposed Ehrlich by using economic theories; ie. Resources needed to support populations are becoming more abundant, not scarcer;
 Echoed in recent debates by Julian Simon, who opposed Ehrlich by using economic theories; ie. Resources needed to support populations are becoming more abundant, not scarcer;.")
12
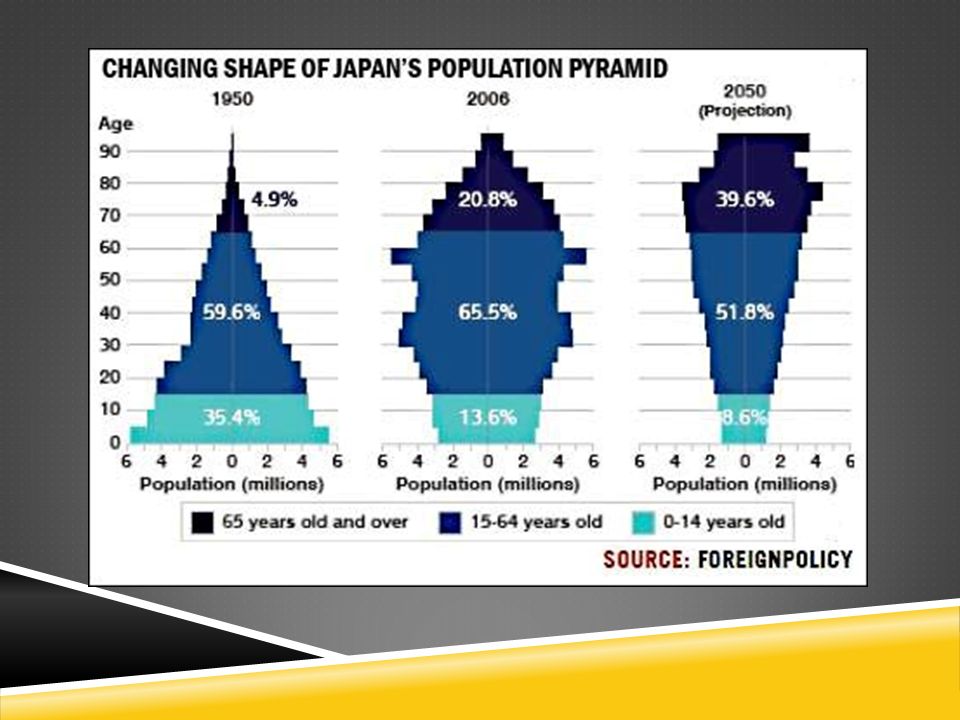
POSSIBLE STAGE 5: DECLINE Low CBR Increasing CDR Negative NIR Large Elderly Population Less Young Women having Children High Dependency Ratio---pensions, elder care

16
THE EPIDEMIOLOGIC CHARACTER OF POPULATION PHENOMENA epi, upon; demos, people; logos, study Epidemiology is the study of what “comes upon” groups of people. Epidemiology is concerned with the distribution of disease and death, and with their determinants and consequences in population groups.

17
1. EPIDEMIOLOGICAL TRANSITION Concept Focuses on changes over time in the causes of mortality affecting certain populations: Health conditions. Disease patterns. Result in a decline in death rates and an increase of life expectancy. The society goes through a transition from communicative diseases to degenerative diseases.

18
1. EPIDEMIOLOGICAL TRANSITION Time Share of mortality Communicative diseases Degenerative diseases Age of communicative diseases Age of receding pandemics Age of degenerative and man-made diseases High Fertility High Mortality High Fertility Decreasing Mortality Low Fertility Low Mortality LI=70 years LI=50 years LI=30 years

19
THE EPIDEMIOLOGIC TRANSITION

20
THE EPIDEMIOLOGIC TRANSITION STAGE 1: PESTILENCE AND FAMINE Infectious and parasitic diseases Epidemics Example Black Plague High CDR

21
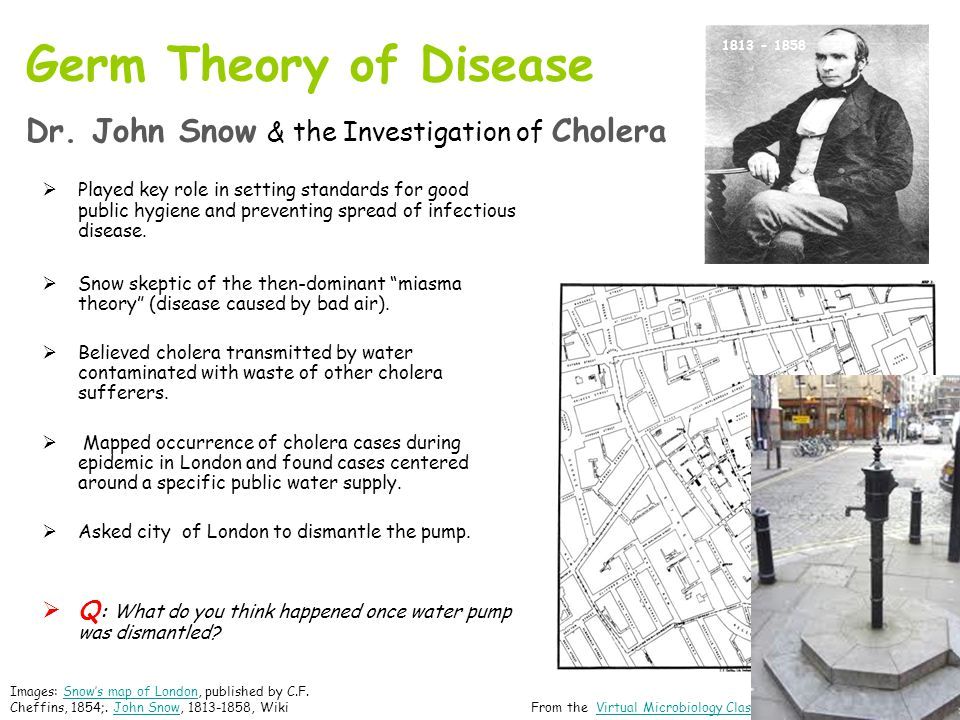
THE EPIDEMIOLOGIC TRANSITION STAGE 2: RECEDING PANDEMICS Improved sanitation, nutrition, & medicine during Industrial Revolution Rapidly Declining CDR

23
Fig. 2-23: By mapping the distribution of cholera cases and water pumps in Soho, London, Dr. John Snow identified the source of the water-borne epidemic. CHOLERA IN LONDON, 1854

24
THE EPIDEMIOLOGICAL TRANSITION STAGE 3 – DEGENERATIVE & HUMAN- CREATED DISEASES Chronic Disorders associated with aging Cardiovascular diseases (hear attacks) & cancer Moderately Declining CDR
 & cancer Moderately Declining CDR")
25
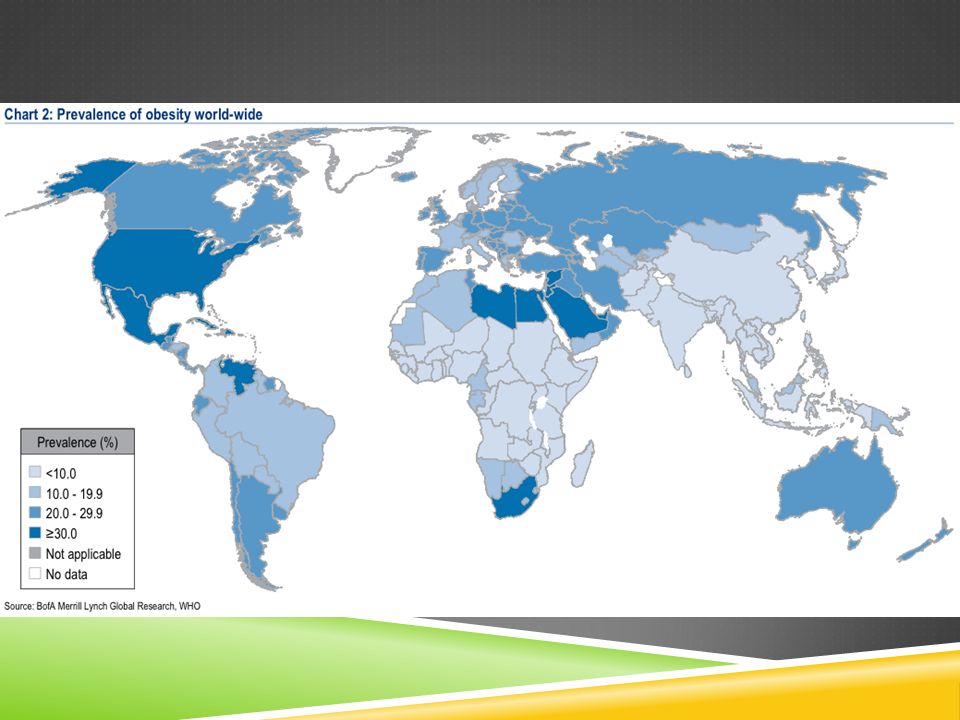
THE EPIDEMOLOGICAL TRANSITION STAGE 4: DELAYED DEGENERATIVE DISEASES Cardiovascular diseases and cancers BUT life expectancy of older people extended through medical advances Cancer growth retarded or removed Bypass to repair cardiovascular system High Obesity rates Non-nutritious food/sedentary lifestyle Low but increasing CDR

27
SPRAWL & OBESITY

28
SPRAWL AND HEALTH CONCERNS Because this study is ecologic and cross-sectional in nature, it is premature to imply that sprawl causes obesity, hypertension, or any other health condition. Our study simply indicates that sprawl is associated with certain outcomes. Future research using quasi-experimental designs is needed to tackle the more difficult job of testing for causality. “Relationship Between Urban Sprawl and Physical Activity, Obesity, and Morbidity” by Reid Ewing, Tom Schmid, Richard Killingsworth, Amy Zlot, Stephen Raudenbush in the American Journal of Health Promotion, Inc., September/October 2003, Vol. 18, No. 1

29
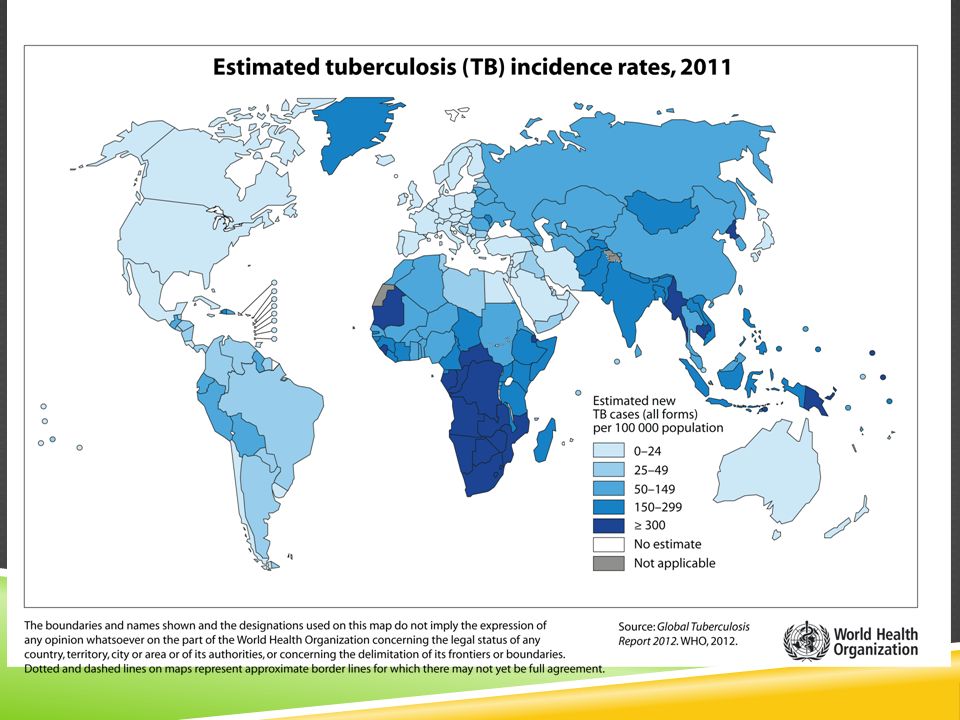
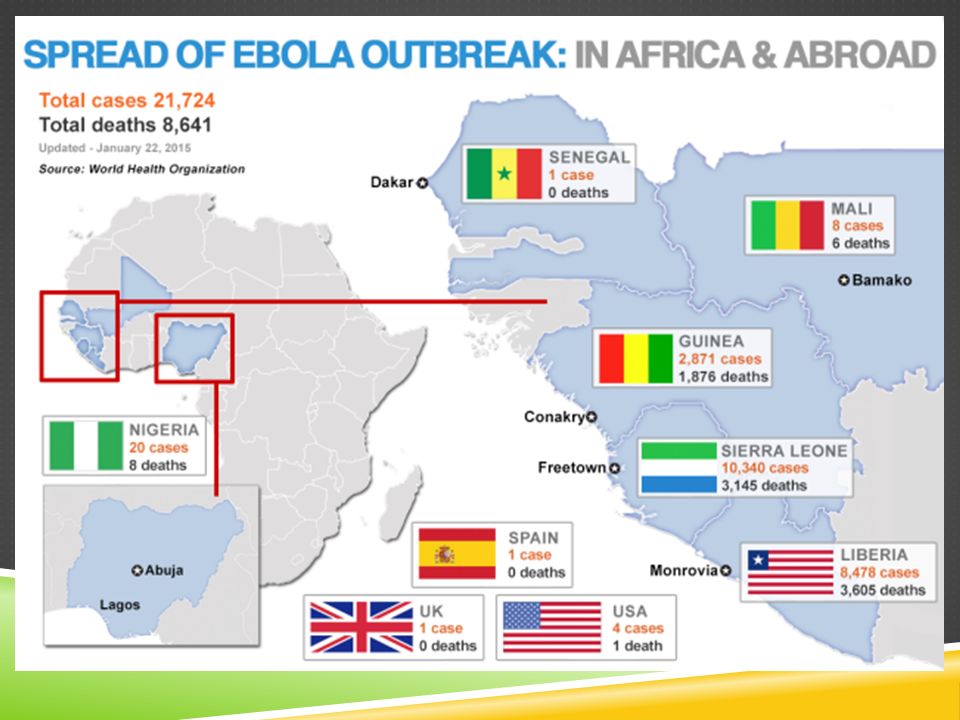
THE EPIDEMIOLOGICAL TRANSITION STAGE 5 – REEMERGENCE OF INFECTIOUS & PARASITIC DISEASES Evolution Antibiotics and genetic engineering Emergence of new strains of viruses and bacteria Poverty Unsanitary conditions in developing countries Increased Connections Spreads from Developing to developed countries

33
HIV/AIDS PREVALENCE RATES, 2005 Fig. The highest HIV infection rates are in sub-Saharan Africa. India and China have large numbers of cases, but lower infection rates at present.

34
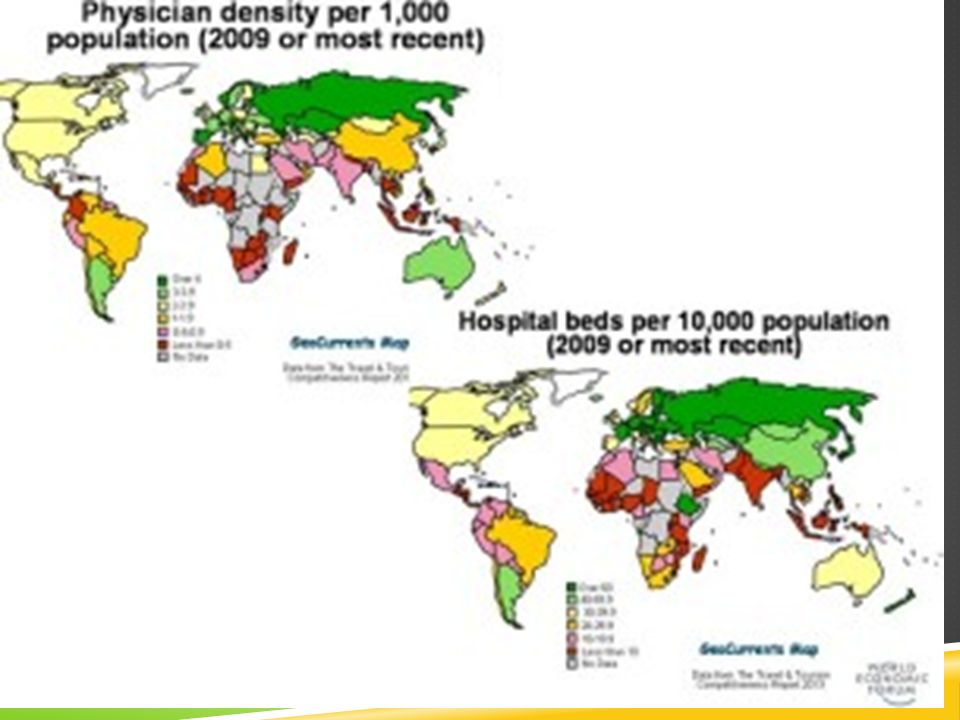
HEALTH CARE Indicators of Health Infant Mortality rate Life Expectancy Provision of Health Care Health Care expenditures Available Medical Services

35
Fig. 2-10: The infant mortality rate is the number of infant deaths per 1000 live births per year. The highest infant mortality rates are found in some of the poorest countries of Africa and Asia. INFANT MORTALITY RATES

36
Fig. 2-11: Life expectancy at birth is the average number of years a newborn infant can expect to live. The highest life expectancies are generally in the wealthiest countries, and the lowest in the poorest countries. LIFE EXPECTANCY AT BIRTH

37
HEALTH CARE PER CAPITA

38
GOVERNMENT EXPENDITURES ON HEALTH CARE

Similar presentations





















 Thomas Malthus, Population Bomb?>")