Download presentation
Presentation is loading. Please wait.

1
Poisoning Ali Alhaboob Assisstant Professor of Pediatrics PICU consultant n Overview of pediatric poisoning, diagnosis and treatment n Summary of the most encountered poisoning

2
Epidemiology n Most of the toxic exposures have only minor or no effect on the child n 85% - 90% of pediatric poisoning occurs in < 5 yrs of age (accidental) usually single agent n 10% - 15% in older age, mainly adolescents (intensional) usually several agents n 3-4% of PICU admission are because of toxic exposures
 usually single agent n 10% - 15% in older age, mainly adolescents (intensional) usually several agents n 3-4% of PICU admission are because of toxic exposures")
3
ED referral recommendations n Serious exposures n Younger than 6 months n History of previous toxic ingestion n Questionable or unreliable history

4
Routes of exposures in children n Ingestion n Inhalation n Skin exposure

5
Common agents Less common but serious n Cosmetics and personal care product n Cleaning substances n Plants n Analgesics n Fe supplements n Antidepressants n Pesticides n Hydrocarbon

6
History n Identification of the toxic agent n The time elapsed n The route of exposure n Underlying medical problems n The clinical effect (with few exceptions rapidity of symptoms progression correlates with severity of poisoning.e.g., acetaminophen) n ? Trauma in addition to ingestion (change in LOC).
..")
7
Physical Exam n Weight (determine ? mg/kg ingested) n Vital signs n Check odors from the breath, skin, hair, clothing n Thorough exam for any abnormal finding
 n Vital signs n Check odors from the breath, skin, hair, clothing n Thorough exam for any abnormal finding.")
8
General presentations suggestive of poisoning n Severe vomiting, diarrhea n Acutely disturbed consciousness n Abnormal behavior n Seizure n unusual odor n Shock n Arrhythmias n Metabolic acidosis n Cyanosis n Respiratory distress

9
Clinical clues to the diagnosis of unknown poisoning n Odor n Skin n Mucous membranes n Temperature n Blood pressure n Pulse rate n Respiration n Pulmonary edema n CNS n GI system

10
Odor Signs or symptomPoison n Bitter almond n Acetone n Oil of wintergreen n Garlic n Alcohol n Petroleum n Cyanide n Isopropyl alcohol, methanol, acetylsalicylic acid n Methyl salicylate n Arsenic, phosphorous, thallium, organophosphates n Ethanol, methanol n Petroleum distillates

11
Skin Sign or symptomPoison n Cyanosis n Red flush n Sweating n Dry n Methemoglobinemia secondary to nitrates, nitrites, phenacetin, benzocaine n Carbon monoxide, cyanide, boric acid, anticholenergics n Amphetamines, LSD, organophosphates, cocaine, barbiturates n Anticholenergics

12
Mucous membranes Signs or symptomsPoison n Dry n Salvation n Oral lesions n Lacrimation n Anticholenergics n Organophosphates, carbamates n Corrosives, paraquat n Caustics, organophosphates, irritant gases

13
Temperature Signs or symptomsPoison n Hypothermia n Hyperthermia n Sedatives hypnotics, ethanol, carbon monoxide, clonidine, phenothiazines, TCAs n Anticholenergics, salicylates, phenothiazines, cocaine, TCAs, amphetamines, theophylline

14
Blood Pressure Signs or symptomsPoison n Hypertension n Hypotension n Sympathomimitics (especially phenylpropanolamine in over- the-counter cold remedies), organophosphates, amphetamine, phencyclidine, cocaine n Antihypertensives, barbiturates, benzodiazepines, beta blockers, Ca++ channel blockers, clonidine, TCAs
, organophosphates, amphetamine, phencyclidine, cocaine n Antihypertensives, barbiturates, benzodiazepines, beta blockers, Ca++ channel blockers, clonidine, TCAs")
15
Pulse rate Signs or symptomsPoison n Bradycardia n Tachycardia n Arrhythmias n Digitalis, sedatives hypnotics, beta blockers, ethchlorvynol, opioids n Antichlonergics, sympathomimetics, amphetamines, alcohol, aspirin, theophylline, cocaine, TCAs n Anticholenergics, TCAs, organophosphates, digoxin, phenothiazines, betablockers, carbon monoxide, cyanide

16
Respirations Signs or symptomsPoisoning n Depressed n Tachypnea n Kussmaul’s sign n Wheezing n Pneumonia n Pulmonary edema n Alcohol, opioids, barbiturates, sedatives/hypnotics, TCAs, paralytic shelfish poisoning n Salicylates, amphetamines, carbon monoxide n Methanol, ethylene glycol, salicylates n Organophosphates n Hydrocarbons n Aspiration, salicylates, opioids, sympathomimetics

17
CNS Sings or symptomsPoison n Seizures n Fasciculation n Hypertonus n Myoclonus, rigidity n Camphor, carbon monoxide, cocaine, amphetamines, sympathomimetics, anticholenergic, aspirin, pesticides, organophosphates, lead, PCP, phenothiazines, INH, lithium, theophylline, TCAs n Organophosphates n Anticholenergics, phenothiazines n Anticholenergics, phenothiazines, haloperidol

18
CNS Sings or symptomsPoison n Delirium/psychos is n Coma n Weakness, paralysis n Anticholenergics, phenothiazines, sympathomimetics, alcohol, PCP, LSD, marijuana, cocaine, heroin, heavy metals n Alcohol, anticholenergics, sedative hypnotics, opioids, carbon monoxide, TCAs, salicylates, organophosphates n Organophosphates, carbamates, heavy metals

19
EYE Signs or symptomsPoison n Miosis n Mydriasis n Blindness n Nystagmus n Opioids, phenothiazines, organophosphates, benzodiazepines, barbiturates, mushrooms, PCP n Antichlenergics, sympathomimitics (cocaine, amphetamines, LSD, PCP), TCA, methanol, glutethimide n Methanol n Diphenylydantoin, barbiturates, carbamazepine, PCP,carbon monoxide, glutethimide, ethanol
, TCA, methanol, glutethimide n Methanol n Diphenylydantoin, barbiturates, carbamazepine, PCP,carbon monoxide, glutethimide, ethanol")
20
GI Sings or symptomsPoison n Vomiting, diarrhea n Iron, phosphorous, heavy metals, lithium, mushroom, fluoride, organophosphates

21
Toxidromes of Common Pediatric Poisonings ToxinSigns or symptoms n Anticholenergi cs (atropine, scopolamine, TCAs, antihistamines, mushrooms) n Cholenergics (organophosph ates and carbamate insecticides) n Fever, flushed, warm, dry skin, dry mouth, mydriasis, tachycardia, arrhythmias, agitation, hallucinations, coma n Salivation, lacrimation, sweating, bronchorrhea, emesis, diarrhea, miosis, bradycardia, bronchospasm with wheezing, confusion, weakness, fasciculations, coma
 n Cholenergics (organophosph ates and carbamate insecticides) n Fever, flushed, warm, dry skin, dry mouth, mydriasis, tachycardia, arrhythmias, agitation, hallucinations, coma n Salivation, lacrimation, sweating, bronchorrhea, emesis, diarrhea, miosis, bradycardia, bronchospasm with wheezing, confusion, weakness, fasciculations, coma")
22
Toxidromes of Common Pediatric Poisonings ToxinSigns or symptoms n Opiates n Narcotic withdrawal n Hypothermia, hypoventilation, hypotension, bradycardia, miosis, coma n Nausea, vomiting, diarrhea, abdominal pain, lacrimation, diaphoresis, mydriasis, tremor, irritability, delirium, seizure

23
Toxidromes of Common Pediatric Poisonings ToxinSigns or symptoms n Sedative/ hypnotics n TCAs n Phenothiazines n Hypothermia, hypoventilation, hypotension, tachycardia, coma n Coma, convulsions, arrhythmias, anticholenergic manifestations n Hypotension, tachycardia, dystonia syndrome, oculogyric crisis, trismus, ataxia, coma, anticholenergic manifestations

24
Toxidromes of Common Pediatric Poisonings ToxinSigns or symptoms n Salicylates n Iron n Sympathomimetics (amphetamines, phenylpropanolamie, ephedrine, caffeine, cocaine, aminophylline) n Fever, hyperpnea, vomiting, tinnitus, acidosis, seizure, lethargy, coma n Hyperglycemia, shock, hemorrhagic diarrhea n Tachycardia, arrhythmias, psychosis, hallucinations, nausea, vomiting, abdominal pain
 n Fever, hyperpnea, vomiting, tinnitus, acidosis, seizure, lethargy, coma n Hyperglycemia, shock, hemorrhagic diarrhea n Tachycardia, arrhythmias, psychosis, hallucinations, nausea, vomiting, abdominal pain")
25
Laboratory tests n Qualitative toxicology screening is rarely as helpful as Hx and PE in determining the cause n Best done on urine and gastric aspirate samples n Quantitative serum level of known drug is indicated when it can enable prediction of toxicity or determination of treatment n ABGs with respiratory symptoms and to assess acid-base balance n Blood glucose from 1st sample n Liver and kidney function (metabolism&excretion) n Serum electrolytes (anion gap, renal function) n Serum osmolar gap n CBC (anemia, hemolysis) n DIC panel when suspected
 n Serum electrolytes (anion gap, renal function) n Serum osmolar gap n CBC (anemia, hemolysis) n DIC panel when suspected")
26
Routine Laboratory Tests That Can Suggest Poisoning

27
Drugs with clinically useful serum level quantitation n Acetaminophen n Anticonvulsants n Carbon monoxide n Cholinesterase n Digoxin n Ethanol n Ethylene glycol n Heavy metals n Iron n Isopropanol n Lead n Lithium n Methanol n Methemoglobin n Salicylate n Theophylline

28
Radiography indications n If head trauma cannot be excluded (skull and cervical spine film, head CT if physical findings are suggestive) n If child abuse is suspected (skeletal survey) n If patient is having respiratory distress (CXRay) n If radiopaque substance is suspected
 n If child abuse is suspected (skeletal survey) n If patient is having respiratory distress (CXRay) n If radiopaque substance is suspected")
29
Common substances that are radiopaque (CHIPES) n Chloral hydrate n Heavy metals n Iodine n Phenothiazine n Enteric coated and extended release medication n Salt tablets (in Fe ingestion, serial films indicate movement and elemination)
 n Chloral hydrate n Heavy metals n Iodine n Phenothiazine n Enteric coated and extended release medication n Salt tablets (in Fe ingestion, serial films indicate movement and elemination)")
30
Treatment n Airway: patency and protective mechanisms (if absent, use nonspecific antidote of D10W 2cc/kg and Naloxone 0.1mg/kg; if no response intubate. n Breathing: clear secretions, give O2, continuous O2 saturation, ABGs, CXRay, treat wheezing and stridor, early controlled intubation prefered n Circulation: frequent VS, continuous CR monitor, fluids for low BP, do baseline ECG, watch for arrythmias, PALS guidelines n Neurologic status: frequent assessments, the most common cause to admit intoxication to PICU, use nonspecific antidotes, watch for seizures, rule out metabolic causes of seizure

31
GI decontamination Emesis-Syrup of Ipecac TherapyContraindications n Dosage in < 1 yr10 ml n Young children15 ml n Adolescents, adults30 ml may repeat once n Petroleum distillates n Caustic agents n Impaired consciousness, seizures n Rapid coma-inducing agents (e.g., propoxyphene, TCAs)
")
32
GI decontamination Lavage TherapyContraindications n Large bore orogastric hose (28 Fr for young children, 36-40 Fr for adolescents) n Left recumbent Trendelenburg’s position to reduce the risk of aspiration n Lavage with saline or 1/2 NS until return is clear n Most successful for toxins that delay gastric emptying (aspirin, iron, anticholinergics) and for those forming concretions (iron, salicylates, meprobamate) n Corrosive caustic agents n Controversial in petroleum distillates ingestion n Stupor or coma unless airway is protected
 n Left recumbent Trendelenburg’s position to reduce the risk of aspiration n Lavage with saline or 1/2 NS until return is clear n Most successful for toxins that delay gastric emptying (aspirin, iron, anticholinergics) and for those forming concretions (iron, salicylates, meprobamate) n Corrosive caustic agents n Controversial in petroleum distillates ingestion n Stupor or coma unless airway is protected")
33
GI decontamination Activated Charcoal TherapyContraindications n Administer in all cases after emesis n Dosage: - Children 1 g/kg - Adults 50-100 g n Corrosive agents: charcoal interfers with GI endoscopy

34
GI decontamination Cathartics TherapyContraindications n MgSO4 250 mg/kg/dose P.O.(max dose 30 g) in 10%-20% solution n Sorbitol magnesium citrate Repeat above doses every 2-4 hrs until passage of charcoal stained stools n Avoid MgSO4 in renal failure
 in 10%-20% solution n Sorbitol magnesium citrate Repeat above doses every 2-4 hrs until passage of charcoal stained stools n Avoid MgSO4 in renal failure")
35
Enhanced elimination n Forced diuresis by administering 2-3 times the maintenance fluid to achieve U.O = 2-5 cc/kg/hr (contraindicated in pulmonary or cerebral edema and renal failure) n Urinary alkalinization to eleiminate weak acids(salicylates, barbiturates and methotrexate), can be achieved by adding NaHCO3 to the IV fluids, the goal is urine pH of 7-8 n Serum alkalinization in TCAs toxicity n Hemodialysis in low molecular weight substances with low volume of distribution and low binding to plasma proteins n Hemoperfusion, protein binding is not a limitation
 n Urinary alkalinization to eleiminate weak acids(salicylates, barbiturates and methotrexate), can be achieved by adding NaHCO3 to the IV fluids, the goal is urine pH of 7-8 n Serum alkalinization in TCAs toxicity n Hemodialysis in low molecular weight substances with low volume of distribution and low binding to plasma proteins n Hemoperfusion, protein binding is not a limitation")
36
Antidotal Therapy n Only a small proportion of poisoned patients are amenable to antidotal therapy n Only a few poisoning is antidotal therapy urgent (e.g., CO, cyanide, organophosphate and opioid intoxication)
")
37
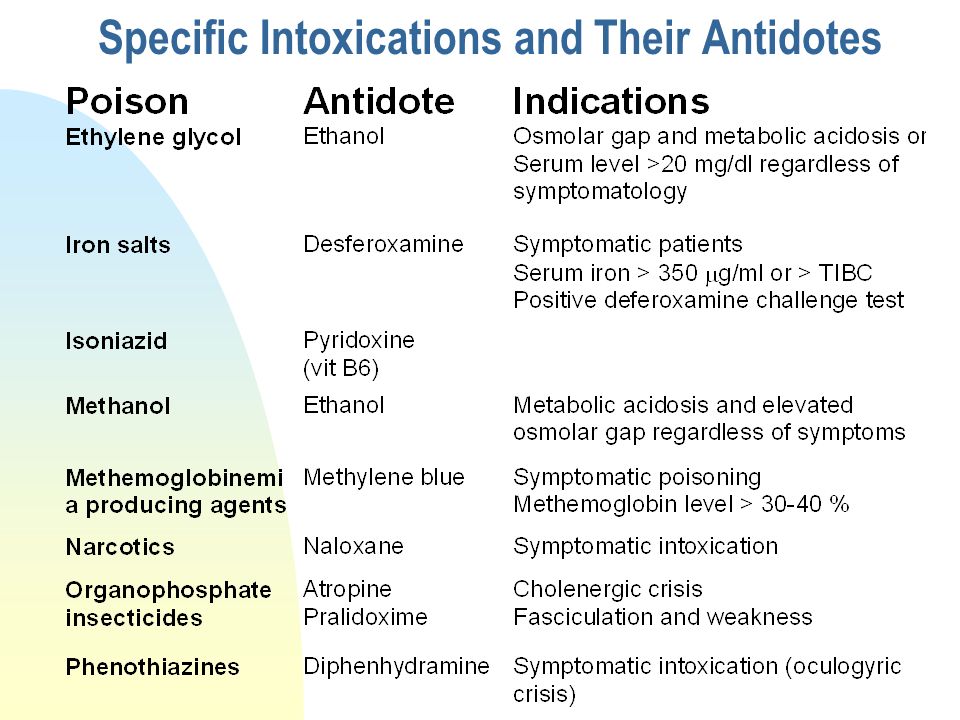
Specific Intoxications and Their Antidotes

39
Acetaminophen (paracetamol) poisoning n Nausea, vomiting and malaise for 24 hrs n Improvement for 24-48 hrs n Hepatic dysfunction after 72 hrs (AST is the earliest and most sensitive) n Death may occur from fulminant hepatic failue n Toxicity likely with ingestion of > 150 mg/kg n Rumack-Matthew nomogram defines the risk of hepatic damage in acute intoxication (level at 4 hrs post ingestion)
 poisoning n Nausea, vomiting and malaise for 24 hrs n Improvement for hrs n Hepatic dysfunction after 72 hrs (AST is the earliest and most sensitive) n Death may occur from fulminant hepatic failue n Toxicity likely with ingestion of > 150 mg/kg n Rumack-Matthew nomogram defines the risk of hepatic damage in acute intoxication (level at 4 hrs post ingestion)")
40
Acetaminophen (paracetamol) poisoning management n GI decontamination n Activated charcoal within 4 hrs of ingestion n Antidote N-acetylcysteine is most effective if given within 8 hrs of ingestion, total of 17 doses, P.O or IV (However, NAC should be given even with > 24hrs presentation) n NAC should be given if serum acetaminophen level is either in the “possible” or “probable” hepatotoxic range
 poisoning management n GI decontamination n Activated charcoal within 4 hrs of ingestion n Antidote N-acetylcysteine is most effective if given within 8 hrs of ingestion, total of 17 doses, P.O or IV (However, NAC should be given even with > 24hrs presentation) n NAC should be given if serum acetaminophen level is either in the possible or probable hepatotoxic range")
41
Salicylate toxicity Clinical manifestations CommonUncommon n Fever n Sweating n Nausea n Vomiting n Dehydration n Hyperpnea n Tinnitus n Seizures n Coma n Coagulopathy n Respiratory depression n Pulmonary edema n SIADH n Hemolysis n Renal failure n Hepatotoxicity n Cerebral edema

42
Laboratory findings in salicylate toxicity n Metabolic acidosis n Respiratory alkalosis n Mixed (resp alkalosis &metabolic acidosis) n Hyperglycemia, Hypoglycemia n Hypernatremia, hyponatremia n Hypokalemia n Hypocalcemia n Prolonged PT n Ketouria
 n Hyperglycemia, Hypoglycemia n Hypernatremia, hyponatremia n Hypokalemia n Hypocalcemia n Prolonged PT n Ketouria")
43
Prediction of acute salicylate toxicity n Ingested dose can predict the severity n < 150 mg/kg toxicity not expected (asymptomatic) n 150-300 mg/kgtoxicity mild to moderate (mild to moderate hyperpnea, lethargy or excitability) n 300-500 mg/kgsevere toxicity (severe hyperpnea, coma or semicoma, sometimes with convulsions)
 n mg/kgtoxicity mild to moderate (mild to moderate hyperpnea, lethargy or excitability) n mg/kgsevere toxicity (severe hyperpnea, coma or semicoma, sometimes with convulsions)")
44
Management of salicylate toxicity n GI decontamination n Correct dehydration and force diuresis n Urine alkalinization and acidosis correction with IV NaHCO3 n Monitor electrolytes, glucose, calcium n Vit K for hemorrhagic diathesis n Decrease fever with external cooling n Hemodialysis for severe intoxication (Dome nomogram), severe acidosis unresponsive to NaHCO3, renal failure, pulmonary edema and severe CNS manifestation
, severe acidosis unresponsive to NaHCO3, renal failure, pulmonary edema and severe CNS manifestation")
Similar presentations







 needed to regulate blood glucose levels is ineffective; Glucose levels can get too high or too low Type I - patients.>")



 enquiries.>")





>")

