Download presentation
Presentation is loading. Please wait.

1
APPROACH TO TOXICOLOGY Dr Sattam Alenezi

2
TOXIC overdose can present with a great variety of clinical symptoms from minor presentations such as nausea and vomiting, to the calamitous, including altered mental status, seizures, cardiac dysrhythmias, hypotension, and respiratory depression.

3
Attempts to identify the poison should, of course, never delay life-saving supportive care.

4
Stabilize ABC and abnormal vital signs. Search to indentify toxidromes. Perform a focused diagnosed workup. Decontamination and antidote as indicated.

5
History The type of toxin or toxins, Time of exposure (acute vs chronic), Amount taken, and Route of administration (e.g., ingestion, intravenous, inhalation).
, Amount taken, and Route of administration (e.g., ingestion, intravenous, inhalation).")
6
Why the exposure occurred (accidental, suicide attempt, a search for euphoria, therapeutic misadventure….. Prior suicide attempts or psychiatric history.

7
Question the patient about all drugs taken, including : Prescription drugs, Over-the-counter medications Vitamins, Herbal preparations.

8
Information solicited from paramedics, police, family, and friends may prove helpful PATIENTS ?

9
In cases of occupational exposure, obtain a description of the work environment and contact people at the site for relevant data

10
PHYSICAL EXAMINATION After stabilization. Systematic approach : Vital signs The eyes Neuro exam Odors Physical stigmata of injection drug use

11
Bradycardia (PACED) Propranolol or other betablockers, Anticholinesterase drugs Clonidine, calcium-channel blockers Ethanol or other alcohols Digoxin
 Propranolol or other betablockers, Anticholinesterase drugs Clonidine, calcium-channel blockers Ethanol or other alcohols Digoxin")
12
Tachycardia (FAST) Free base or other forms of cocaine Anticholinergics, antihistamines, amphetamines Sympathomimetics (cocaine, amphetamines), solvent abuse Theophylline
 Free base or other forms of cocaine Anticholinergics, antihistamines, amphetamines Sympathomimetics (cocaine, amphetamines), solvent abuse Theophylline")
13
Hypothermia (COOLS) Carbon monoxide Opiates Oral hypoglycemics, insulin Liquor Sedative-hypnotics
 Carbon monoxide Opiates Oral hypoglycemics, insulin Liquor Sedative-hypnotics")
14
Hyperthermia (NASA) Neuroleptic malignant syndrome, nicotine Antihistamines Salicylates, sympathomimetics Anticholinergics, antidepressants
 Neuroleptic malignant syndrome, nicotine Antihistamines Salicylates, sympathomimetics Anticholinergics, antidepressants")
15
Hypotension (CRASH) Clonidine, calcium-channel blockers Reserpine or other antihypertensive agents Antidepressants, aminophylline Sedative-hypnotics Heroin or other opiates
 Clonidine, calcium-channel blockers Reserpine or other antihypertensive agents Antidepressants, aminophylline Sedative-hypnotics Heroin or other opiates")
16
Hypertension (CT SCAN) Cocaine Thyroid supplements Sympathomimetics Caffeine Anticholinergics, amphetamines Nicotine
 Cocaine Thyroid supplements Sympathomimetics Caffeine Anticholinergics, amphetamines Nicotine")
17
Rapid respiration (PANT) PCP, paraquat, pneumonitis (chemical) ASA and other salicylates Non-cardiogenic pulmonary edema Toxin-induced metabolic acidosis
 PCP, paraquat, pneumonitis (chemical) ASA and other salicylates Non-cardiogenic pulmonary edema Toxin-induced metabolic acidosis")
18
Slow respiration (SLOW) Sedative-hypnotics (including GHB) Liquor Opiates, sedativehypnotics Weed (marijuana)
 Sedative-hypnotics (including GHB) Liquor Opiates, sedativehypnotics Weed (marijuana)")
19
Miosis (COPS) Cholinergics, clonidine Opiates, organophosphates Phenothiazines, pilocarpine Sedative-hypnotics
 Cholinergics, clonidine Opiates, organophosphates Phenothiazines, pilocarpine Sedative-hypnotics")
20
Mydriasis (AAAS) Antihistamines Antidepressants Atropine and other anticholinergics Sympathomimetics
 Antihistamines Antidepressants Atropine and other anticholinergics Sympathomimetics")
21
Optic neuritis and vision loss may indicate advanced methanol poisoning.

22
Vertical or rotary nystagmus is a finding peculiar to phencyclidine (PCP). Horizontal nystagmus occurs with lithium, barbiturates, sedative-hypnotics, and antiepileptic poisoning(most notably phenytoin [Dilantin] and carbamazepine[Tegretol])
.")
23
Neurologic Examination A systematic neurological evaluation. Seizures are common. Muscle fasciculations (organophosphate poisoning), Rigidity (tetanus and strychnine), Tremors (lithium and methylxanthines) Dystonic posturing (neuroleptic agents)
, Rigidity (tetanus and strychnine), Tremors (lithium and methylxanthines) Dystonic posturing (neuroleptic agents).")
24
Agents That Cause Seizures. OTIS CAMPBELL* Organophosphates Tricyclic antidepressants Isoniazid, insulin Sympathomimetics Camphor, cocaine Amphetamines, anticholinergics Methylxanthines (theophylline, caffeine) Phencyclidine (PCP) Benzodiazepine withdrawal, botanicals (water hemlock), GHB Ethanol withdrawal Lithium, lidocaine Lead, lindane
 Phencyclidine (PCP) Benzodiazepine withdrawal, botanicals (water hemlock), GHB Ethanol withdrawal Lithium, lidocaine Lead, lindane.")
25
Skin Examination Remove the patient’s clothing. Color and temperature of the skin, as well as whether it is dry or diaphoretic. Needle tracks suggest parenteral opiate or cocaine abuse.

26
Diaphoretic skin (SOAP) Sympathomimetics Organophosphates Acetylsalicylic acid or other salicylates Phencyclidine
 Sympathomimetics Organophosphates Acetylsalicylic acid or other salicylates Phencyclidine")
27
Dry skin Antihistamines. Anticholinergics.

28
ODOR POSSIBLE INTOXICANT Bitter almonds Cyanide Fruity Ethanol, acetone, isopropyl alcohol, chlorinated hydrocarbons Garlic Arsenic, dimethyl sulfoxide (DMSO), organophosphates. Glue Toluene, other solvents Pears Chloral hydrate, paraldehyde Rotten eggs Disulfiram, hydrogen sulfide, N-acetylcysteine, dimercaptosuccinic acid (DMSA) Shoe polish Nitrobenzene Wintergreen Methyl salicylate
 Shoe polish Nitrobenzene Wintergreen Methyl salicylate.")
29
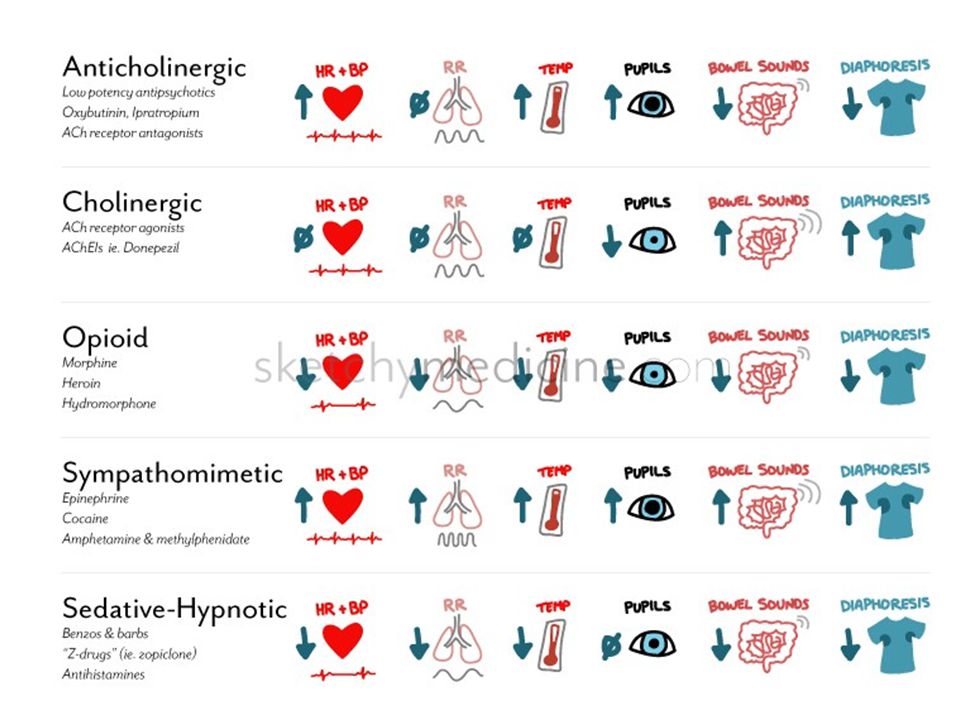
Toxidromes A collection of symptoms associated with certain classes of poisons is known as a toxic syndrome, or toxidrome

30
Cholinergic (organophosphates) ( BAD SLUDGE) o Bradycardia/ Bronchorrhea. o Anxiety. o Delirium. o Salivation o Lacrimation o Urination o Defecation. o Bradycardia. o Gastrointestinal upset. o Emesis

31
Anticholinergic (antihistamines, TCAs) Hyperthermia :HOT as a hare. RED as a beet : flushed skin. Dry as a bone. BLIND as a bat: Dilated pupils MAD as a hatter : altered mental status.

33
Sympathomimetic (cocaine, amphetamines) Diaphoresis Mydriasis. Tachycardia Hypertension Hyperthermia Seizures

34
Narcotic (heroin,methadone) Miosis Hypoventilation Coma Bradycardia Hypotension
 Miosis Hypoventilation Coma Bradycardia Hypotension")
35
Sedative-Hypnotic As benzodiazepins and barbiturates. CNS depression. Respiratory depression. Treatment : supportive flumazinile rarely used.

37
Diagnosis Coma cocktail. ABG. Electrolytes : Anion Gap = Na- (Cl+Hco3). Drug level. Radiography.

38
Agents Causing An Elevated Anion Gap. METALACID GAP Methanol, metformin Ethylene glycol Toluene Alcoholic ketoacidosis Lactic acidosis Aminoglycosides, other uremic agents Cyanide, carbon monoxide Isoniazid, iron Diabetic ketoacidosis Generalized seizure-producing toxins ASA or other salicylates Paraldehyde, phenformin

39
RADIOPAQUE SUBSTANCE CHIPS Chlorinated substance ( pesticides). heavy metals as Iron, and other such as lead, arsenic, mercury Phenothiazines. Sustained-release or enteric coated agents as ASA.

40
DECONTAMINATION Ipecac not used any more. Gastric lavage : Orogastric not nasogastric: Rarely used, has complications. Used in dangerous overdos within 1 hr. Toxin delayed gastric empty. Risk of aspiration and perforation to esophagus, and arrthymia.

41
Activated charcoal : Direct bind to toxin in gut. Some toxins not bind to AC: Pesticide Hydrocarbones Iron Acid /Alkalies/Alcohols Lithium. Solvents.

42
Cathartics Has limited role. Work with AC to avoid constipation. Fluid and electrolytes shifts Not used in : PT with impaired gag reflex. Intestinal obstruction. Caustics.

43
Whole bowel irrigation Use a polyethylene glycol solution is sometimes recommended by poison centers for overdose of metals such as iron and lead, in patients with ingestion of sustained-release formulations, or for the evacuation of drug packets from body packers or body stuffers.

44
Urinary Alkalinization Use in toxins as ASA, phenobarbital, and chloropropamide. Increased urine PH, more toxin will be eliminated by ion trapping mechanism.

45
Dialysis Isopropyl ASA. Theophylline (hemoperfusion by using charcoal). Uremia. Barbiturate. Lithium. Ethylene glycol / ethanol.

Similar presentations













 needed to regulate blood glucose levels is ineffective; Glucose levels can get too high or too low Type I - patients.>")







