Download presentation
Presentation is loading. Please wait.

1
Acid- Base Pathophysiology
Randall L Tackett, PhD University of Georgia College of Pharmacy

2
General Concepts Acid – High concentration of hydrogen ions (donates H+) Base – High concentration of hydroxide ions (accepts H+) pH Describes the acidity or alkalinity of a substance pH scale represents the hydrogen ion concentration

3
Blood pH =

4
pH Small changes in pH produce major disturbances
Most biological processes function within a narrow pH range Affects electrolyte and hormone functions Body produces more acids than bases Metabolic processes produce CO2

5
pH and Cell Membrane Selectively permeable
Permeability of cell membrane influenced by pH Affects the degree of ionization and the concentration of ionized substances Changes in ionization results in loss of substances from the cell

7
pH Kidneys most effective regulator of pH
Can excrete large amounts of acid Conserves and also can excrete bases Rates of correction Buffers - immediately Respiratory system - minutes to hrs Renal mechanisms - several hrs to days

8
Acid-Base Balance Intake of normal diet produces 50 to 100 mEq of hydrogen per day Hydrogen is normally excreted in urine and combined with phosphate and ammonia

11
Carbonic Acid- Bicarbonate System
Primary extracellular fluid buffer system Maintains a ration of bicarbonate to carbonic acid of 20:1

12
Respiratory System Adjusts rate and depth of respiration
Increased rate and depth - CO2 excreted Decreased rate and depth - CO2 conserved Limited gain - cannot completely compensate for changes in pH (only 50-75%) Responds rapidly and helps buffer pH until the renal mechanism kicks in
 Responds rapidly and helps buffer pH until the renal mechanism kicks in.")
13
Renal System Regulates amount of bicarbonate absorbed or excreted
Also regulates ammonia and electrolytes Slower onset but more prolonged action Infinite gain - can completely correct abnormalities in pH

14
Acid-Base Balance Metabolic acidosis begins to occur when GFR decreases by 30% to 40% due to: Decreased ammonia synthesis Decreased bicarbonate reabsorption Phosphate buffers remain effective until late stages of renal failure Bicarbonate levels stabilize at end-stage renal failure because hydrogen is buffered by anions from bone

15
Assessment of Acid-Base
Blood and urine pH Arterial blood gases (ABG) Anion gap Representative of the unmeasured anions in the plasma Aids in the differentiation of cause of metabolic acidosis
 Anion gap. Representative of the unmeasured anions in the plasma. Aids in the differentiation of cause of metabolic acidosis.")
16
Acid-Base Imbalances pH< 7.35 acidosis pH > 7.45 alkalosis
Response to acid-base imbalance is called compensation complete if brought back within normal limits partial compensation if range is still outside norms.

17
Compensation If underlying problem is metabolic, hyperventilation or hypoventilation helps: respiratory compensation. If problem is respiratory, renal mechanisms can result in metabolic compensation.

18
Acidosis Principal effect of acidosis is depression of the CNS through ↓ in synaptic transmission. Generalized weakness Deranged CNS function the greatest threat Severe acidosis causes Disorientation coma death

19
Alkalosis Alkalosis causes over excitability of the central and peripheral nervous systems. Numbness Lightheadedness It can cause : Nervousness Muscle spasms or tetany Convulsions Loss of consciousness Death

21
Respiratory Acidosis Carbonic acid excess
Hypercapnia – high levels of CO2 in blood Chronic conditions: Depression of respiratory center in brain that controls breathing rate – drugs or head trauma Paralysis of respiratory or chest muscles Emphysema

22
Respiratory Acidosis Acute conditions:
Adult Respiratory Distress Syndrome Pulmonary edema Pneumothorax

23
Compensation for Respiratory Acidosis
Kidneys eliminate hydrogen ion and retain bicarbonate ion

24
Signs and Symptoms of Respiratory Acidosis
Breathlessness Restlessness Lethargy and disorientation Tremors, convulsions, coma Respiratory rate rapid, then gradually depressed Skin warm and flushed due to vasodilation caused by excess CO2

26
Respiratory Alkalosis
Carbonic acid deficit pCO2 less than 35 mm Hg (hypocapnea) Most common acid-base imbalance Primary cause is hyperventilation
 Most common acid-base imbalance. Primary cause is hyperventilation.")
27
Respiratory Alkalosis
Conditions that stimulate respiratory center: Oxygen deficiency at high altitudes Pulmonary disease and Congestive heart failure – caused by hypoxia Acute anxiety Fever, anemia Early salicylate intoxication Cirrhosis Gram-negative sepsis

28
Compensation of Respiratory Alkalosis
Kidneys conserve hydrogen ion Excrete bicarbonate ion

30
Metabolic Acidosis Bicarbonate deficit - blood concentrations of bicarb drop below 22 mEq/L Causes: Loss of bicarbonate through diarrhea or renal dysfunction Accumulation of acids (lactic acid or ketones) Failure of kidneys to excrete H+
 Failure of kidneys to excrete H+")
31
Symptoms of Metabolic Acidosis
Headache, lethargy Nausea, vomiting, diarrhea Coma Death

32
Compensation for Metabolic Acidosis
Increased ventilation Renal excretion of hydrogen ions if possible K+ exchanges with excess H+ in ECF ( H+ into cells, K+ out of cells)
")
34
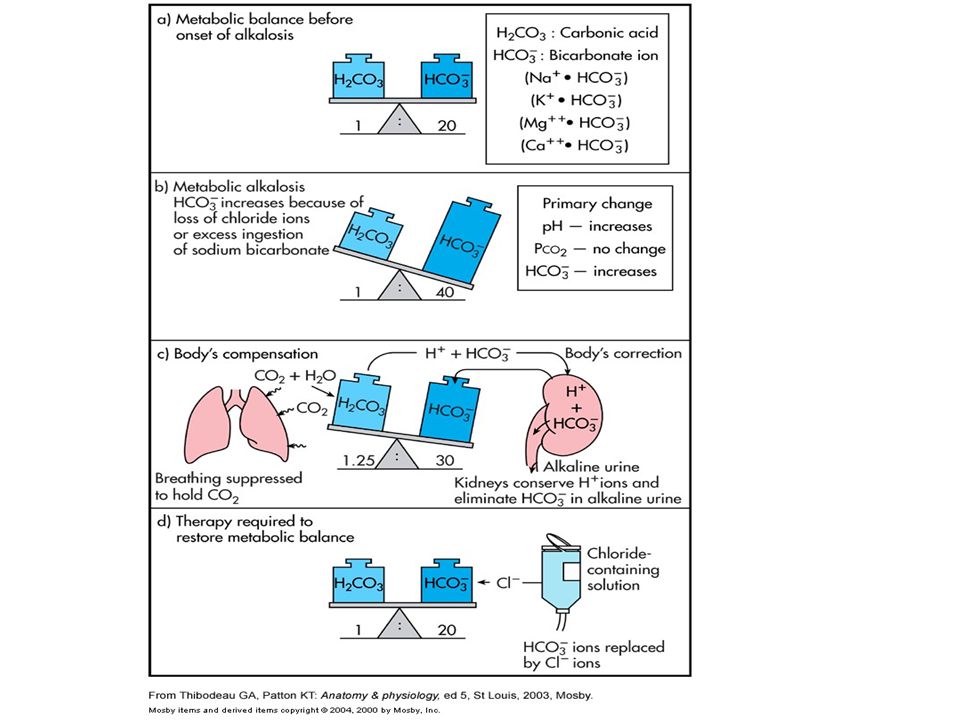
Metabolic Alkalosis Bicarbonate excess - concentration in blood is greater than 26 mEq/L Causes: Excess vomiting = loss of stomach acid Excessive use of alkaline drugs Certain diuretics Endocrine disorders Heavy ingestion of antacids Severe dehydration

35
Compensation for Metabolic Alkalosis
Alkalosis most commonly occurs with renal dysfunction Respiratory compensation difficult – hypoventilation limited by hypoxia

36
Symptoms of Metabolic Alkalosis
Respiration slow and shallow Hyperactive reflexes ; tetany Often related to depletion of electrolytes Atrial tachycardia

38
Phosphate and Calcium Balance
Changes in acid-base balance affect phosphate and calcium In early renal failure, phosphate excretion decreases and plasma phosphate levels increase due to decreased GFR Elevated plasma phosphate binds calcium producing hypocalcemia

39
Phosphate and Calcium Balance
Decreased calcium stimulates the release of parathyroid hormone which releases calcium from bone and enhances urinary phosphate secretion Phosphate and calcium levels return to normal Incremental losses of GFR decreases effectiveness of parathyroid hormone

40
Phosphate and Calcium Balance
When GFR declines to 25% of normal, parathyroid hormone is no longer effective in maintaining serum phosphate Persistent reduction of GFR and hyperparathyroidism results in: Hyperphosphatemia Hypocalcemia Dissolution of bone

41
Phosphate and Calcium Balance
Hypocalcemia and bone disease are accelerated by: Impaired synthesis of 1,25 vitamin D3 Lack of vitamin D reduces intestinal absorption of calcium and impairs resorption of phosphate and calcium from bone

Similar presentations









![1 Acid and Base Balance and Imbalance. 2 pH Review pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic;](/14/4450368/big_thumb.jpg "1 Acid and Base Balance and Imbalance. 2 pH Review pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic;>")




 Assistant Prof. in Pathology Al Maarefa College.>")
![1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.](/15/4651316/big_thumb.jpg "1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.>")





 H + concentration in the body.>")

![Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.](/20/5962628/big_thumb.jpg "Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.>")
 donors in biochemical equations/solutes.>")
 concentration. More H + = more acidic = lower.>")
