Download presentation
Presentation is loading. Please wait.

1
Biochemistry of tooth tissues and saliva: biological role, physical-chemical properties and biochemical content. Regulation and pathology of saliva formation, significance in the appearance of dental diseases.

2
Teeth The role is to masticate (chew) food
Humans have two sets of teeth Deciduous (baby or milk) teeth 20 teeth are fully formed by age two Permanent teeth Replace deciduous teeth beginning between the ages of 6 to 12 A full set is 32 teeth, but some people do not have wisdom teeth
 teeth. 20 teeth are fully formed by age two. Permanent teeth. Replace deciduous teeth beginning between the ages of 6 to 12. A full set is 32 teeth, but some people do not have wisdom teeth.")
3
Tooth is a complex system of specialized tissues
Teeth contain tooth enamel and dentin Dentin contains collagen and is similar in composition to bone

4
A . TOOTH TISSUES TOOTH ENAMEL, is the hardest part of the tooth Enamel acts as a protective tissue that covers the exposed part of a tooth, the crown. 2. DENTIN , is the tissue that forms the mainl mass of a tooth. It supports the enamel and absorbs the pressure of eating. 3. DENTAL PULP, a soft connective tissue containing nerves and blood vessels, that nourish the tooth. 4. CEMENTUM, covers the dentine outside of the root (under the gum line) and it is attached to the bone of the jaw with little elastic fibers
 and it is attached to the bone of the jaw with little elastic fibers.")
5
Dentin Dentin is a mineralized connective tissue with an organic matrix of collagenous proteins. dentin contain exclusively genetic Type I collagen The chain are high in glycine (Gly), proline (Pro) and hydroxyproline (Hyp) content.
, proline (Pro) and hydroxyproline (Hyp) content.")
6
The HAP of teeth is not compositionally pure
Composed of mineralized calcium phosphate (specifically, the calcium phosphate phase called hydroxyapatite (HAP) Ca10(PO4)6(OH)2) within a matrix of collagen fibrils The HAP of teeth is not compositionally pure it’s composition can actually be better represented as (Ca, Sr, Mg, Na, H2O)10(PO4, HPO4, CO3P2O7)6(OH, F, Cl, H2O)2 HAP is a ‘living mineral’ that is continually grown, dissolved & remodeled in response to signals of internal (e.g., pregnancy) and external (e.g., gravity, exercise) origin
 Ca10(PO4)6(OH)2) within a matrix of collagen fibrils. The HAP of teeth is not compositionally pure. it’s composition can actually be better represented as. (Ca, Sr, Mg, Na, H2O)10(PO4, HPO4, CO3P2O7)6(OH, F, Cl, H2O)2. HAP is a ‘living mineral’ that is continually grown, dissolved & remodeled in response to signals of internal (e.g., pregnancy) and external (e.g., gravity, exercise) origin.")
7
Apatites of tooth tissues
Ca10(PO4)6(OH)2 Ca8H2(PO4)6 · 5H2O Ca10(PO4)6CO3 or Ca10(PO4)5CO3(OH)2 Ca10(PO4)6Cl SrCa9(PO4)6(OH)2 Ca10(PO4)6F2
6(OH)2. Ca8H2(PO4)6 · 5H2O. Ca10(PO4)6CO3 or Ca10(PO4)5CO3(OH)2. Ca10(PO4)6Cl. SrCa9(PO4)6(OH)2. Ca10(PO4)6F2.")
8
Hydroxyappatite

9
Enamel is 95% HAP Enamel gains mechanical strength by interweaving HAP crystals Enamel initially starts with a high protein content, but these are removed and the voids backfilled with HAP as the tooth matures

10
B. PERIODONTAL TISSUES 5. GUMS, the tough pink-colored skin that covers the bone of the jaw and supports the tooth along with the alveolar bone. HEALTHY GINGIVA CONTAINS MANY FIBROBLASTS AND A FEW INFLAMMATORY CELLS SUCH AS MACROPHAGES ,NEUTROPHILS, PLASMA CELLS AND LYMPHOCYTES.

11
6. PERIODONTAL LIGAMENT, the tissue between the cementum and the alveolar bone. It consists of tough little elastic fibers that keep the tooth attached to the jaw. 7. ALVEOLAR BONE, the bone of the jaw that keeps the tooth in its place, it feeds and protects it.

12
Enamel is the hardest and most highly mineralized substance of the body, and with dentin, cementum, and dental pulp is one of the four major tissues which make up the tooth. Ninety-six percent of enamel consists of mineral, with water and organic material composing the rest. The formation of dentin - dentinogenesis. The porous, yellow-hued material is made up of 70% inorganic materials, 20% organic materials, 10% water.

13
Cementum Cementum is a specialized bony substance covering the root of a tooth. 45% inorganic material (mainly hydroxyapatite), 33% organic material (mainly collagen) 22% water. Cementum is excreted by cementoblasts within the root of the tooth and is thickest at the root apex. Pulp The dental pulp is the part in the center of a tooth made up of living soft tissue and cells called odontoblasts. Those include: Fibroblasts, Granulocites, Histiosites etc. It's commonly called 'the nerve', although it contains many other structures which are not nerves.
 22% water. Cementum is excreted by cementoblasts within the root of the tooth and is thickest at the root apex. Pulp. The dental pulp is the part in the center of a tooth made up of living soft tissue and cells called odontoblasts. Those include: Fibroblasts, Granulocites, Histiosites etc. It s commonly called the nerve , although it contains many other structures which are not nerves.")
14
Biochemical composition of teeth tissues
Compounds pulp dentin enamel cementum Water g per 100 g tissue 13 2,5 3,2 Organic compounds 40 20 4 25 Inorganic compounds 69 96 70 Ca g per 100 g of ashes 30 35 36 35,5 Mg 0,8 1,2 0,5 0,9 Na 0,2 1,1 K 0,1 0,3 P 17,0 17,4 17,3 17,1 F 0,02 citrate - 1,0

15
Organic components Soluble proteins: Albumins, globulins Enzymes:
Alkaline phosphatase Acidic phosphatase Glycoproteins No soluble proteins: Collagen Enamelin

16
Carbohydrates Glycogen
Glycosaminoglycans (GAG, mucopolysaccharides) are long-chain compounds made up of hundreds repeating disaccharide units. One of the sugars in each disaccharide unit is a hexosamine (glycosamine). Many proteoglycans contain a core protein which links them to the cellular membrane.
 are long-chain compounds made up of hundreds repeating disaccharide units. One of the sugars in each disaccharide unit is a hexosamine (glycosamine). Many proteoglycans contain a core protein which links them to the cellular membrane.")
17
Proteoglycans Hyaluronic acid is an extremely long and rigid glycosaminoglycan Chondroitin 6 sulphate

18
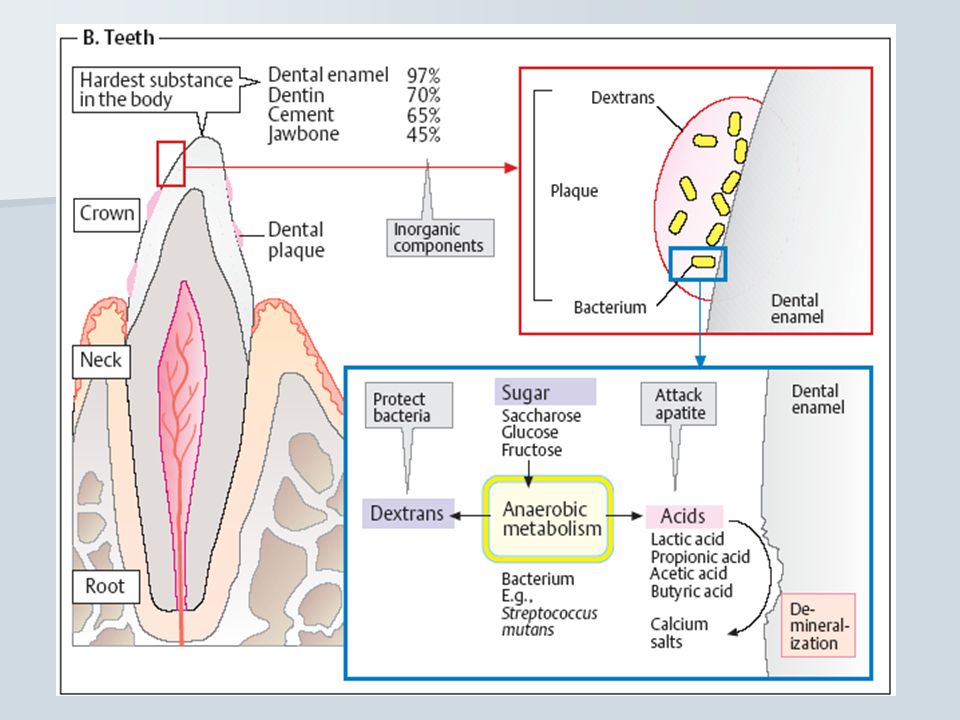
Dental plaque Plaque is a biofilm consisting of large amounts of various bacteria which forms on teeth. If not removed regularly, it can lead to dental cavities (caries) or periodontal problems (such as gingivitis). Given time, plaque can mineralize along the gingiva, forming tartar. The microorganisms that form the biofilm are almost entirely bacteria (mainly streptococcus and anaerobes). Certain bacteria in the mouth in the absence of oxygen produce lactic acid, which dissolves the calcium and phosphorus in the enamel. This process - demineralisation, leads to tooth destruction.
 or periodontal problems (such as gingivitis). Given time, plaque can mineralize along the gingiva, forming tartar. The microorganisms that form the biofilm are almost entirely bacteria (mainly streptococcus and anaerobes). Certain bacteria in the mouth in the absence of oxygen produce lactic acid, which dissolves the calcium and phosphorus in the enamel. This process - demineralisation, leads to tooth destruction.")
19
Scurvy Scurvy - dietary deficiency in vitamin C, leading to abnormal collagen. (hemorrhages, loose of teeth, gums swell and bleed easily)
 .")
20
Dental caries Dental caries, also described as "tooth decay" or "dental cavities", is an infectious disease which damages the structures of teeth. Tooth decay is caused by certain types of acid-producing bacteria which cause the most damage in the presence of fermentable carbohydrates such as sucrose, fructose, and glucose. The resulting acidic levels in the mouth affect teeth because a tooth's special mineral content causes it to be sensitive to low pH

21
Teeth demineralisation:
Са10 (РО4)6(ОН)2 + 2Н+ → Са9Н2 (РО4)6(ОН)2 + Са2+ Conversion of GAP into ftorapatite: Са10 (РО4)6(ОН)2 + 2F- → Са10 (РО4)6F2 + 2(ОН)- Excess of F- couses demineralisation Са10 (РО4)6(ОН)2 + 20F- → 10CаF2 + 6РО (ОН)-
6(ОН)2 + 2Н+ → Са9Н2 (РО4)6(ОН)2 + Са2+ Conversion of GAP into ftorapatite: Са10 (РО4)6(ОН)2 + 2F- → Са10 (РО4)6F2 + 2(ОН)- Excess of F- couses demineralisation. Са10 (РО4)6(ОН)2 + 20F- → 10CаF2 + 6РО (ОН)-")
22
ph 6,4 - 7,8 assists in mineralization
Са2+/ Р for mineralization in saliva is 1,67 Mg2+, Mn2+, Zn2+, Cu2+, Si2+ increase mineralization ph<6,2 leads to the demineralization

24
ORAL ENVIRONMENT CARIES
A progressively destructive, infectious disease resulting in: Demineralization of enamel / cementum Bacterial penetration to pulp Formation of macroscopic activity Caries promotion Caries reduction dietary carbohydrate increased salivary flow reduced salivary flow reduced plaque cariogenic bacteria fluoride Sound enamel plaque acid prod saliva acid neutralization mineral loss mineral gain (fluoride) Lesions Cavity
 Lesions. Cavity.")
25
ORAL ENVIRONMENT SALIVA
A complex fluid secreted by salivary glands containing water, mucin, proteins, salts and enzymes. Functions: aids in digestion lubricates both hard and soft tissues buffers cariogenic acids forms the pellicle provides minerals for repairing enamel / cementum (remineralization) delivers antimicrobial agents (immunoglobulins, enzymes, etc.)
 delivers antimicrobial agents (immunoglobulins, enzymes, etc.)")
26
Saliva neutralises the acids which cause the pH of the tooth surface to rise above the critical pH. This causes 'remineralisation', the return of the dissolved minerals to the enamel. In the presence of plaque, saliva is unable to penetrate through the plaque to neutralize the acid produced by the bacteria.

27
Salivary glands SALIVA Mixture of mucus and serous fluids
Helps to form a food bolus Contains salivary amylase to begin starch digestion Dissolves chemicals so they can be tasted

28
Saliva is secreted to the mouth by three major paired salivary glands (submamandibular, parotid, and sublingual glands) and by numerous minor mucous glands, at a rate of approximately ml.min-1. 65 % from the submandibular, 23 % from the parotid, 8 % from the minor mucous, 4 % from the sublingual.

29
Secretions of Salivary Glands
Parotid glands clear water, serous fluid rich in amylase Sublingual glands primarily mucus most viscous Submandibular glands primarily serous fluid some mucus

30
The most important small salivary glands are:
lingual glands minor sulblingual glands close to the larger major sublingual glands labial glands on the inner surface of the lips palatine glands tonsillar glands buccal glands The labial, sublingual, mlnor lingual and buccal glands are composed predominantly of mucous cells, but some serous cells may be present. The palatine and lateral lingual glands are entirely mucous secreting

31
Digestion The digestive functions of saliva include moistening food, and helping to create a food bolus, so it can be swallowed easily. Saliva contains the enzyme Amylase that breaks some starches down into maltose and dextrin. Salivary glands also secrete enzyme to start fat digestion. This is useful for infants to digest the fat in milk.

32
Pellicle deposits In addition to this, saliva is responsible for depositing salivary pellicle that covers the entirety of the tooth surfaces. This pellicle play a role in plaque formation, it may also act as a protective barrier between acids and the tooth surface

33
Disinfectants Saliva contained in the mouth has natural disinfectants. Human saliva contains such antibacterial agents as secretory IgA, lactoferrin, and lactoperoxidase.

34
Stimulation The production of saliva is stimulated both by the sympathetic nervous system and the parasympathetic. The saliva stimulated by sympathetic innervation is thicker, and saliva stimulated parasympathetically is more watery.

35
Daily salivary output There has been some disagreement regarding the daily salivary output in a healthy individual. Today, it is believed that the average person produces approximately 700mL of saliva per day, which is much less than was once thought.

36
Saliva is characteristically a colorless dilute fluid, with a density ranging from 18 to 35. Its pH is usually around 6.64, and varies depending on the concentration of CO2 in the blood. The total concentration of inorganic and organic constituents is generally low when compared to serum.

37
There are four major components of saliva:
mucus that serves as a lubricant, amylase, an enzyme that initiates the digestion of starch, lingual lipase, an enzyme that begins the digestion of fat, and a slightly alkaline electrolyte solution that moistens food. Human saliva is always hypotonic to plasma. Na+ and Cl- concentrations are less than that of plasma; but K+ and HCO3- concentrations are higher in saliva than in plasma. Amylase and mucus also increase in concentration after stimulation.

38
Saliva Composition Produced in salivary glands, saliva is 98% water, but it contains many important substances, including electrolytes, mucus, antibacterial compounds and various enzymes. Water Electrolytes: 2-21 mmol/L sodium (lower than blood plasma) 10-36 mmol/L potassium (higher than plasma) mmol/L calcium mmol/L magnesium 5-40 mmol/L chloride (lower than plasma) 25 mmol/L bicarbonate (higher than plasma) mmol/L phosphate
 mmol/L potassium (higher than plasma) mmol/L calcium mmol/L magnesium mmol/L chloride (lower than plasma) 25 mmol/L bicarbonate (higher than plasma) mmol/L phosphate.")
39
Mucus. Mucus in saliva mainly consists of mucopolysaccharides and glycoproteins;
Antibacterial compounds (thiocyanate, hydrogen peroxide, and secretory immunoglobulin A) In its secretory form, IgA is the main immunoglobulin found in mucous secretions, including tears, saliva
 In its secretory form, IgA is the main immunoglobulin found in mucous secretions, including tears, saliva.")
40
ENZYMES There are three major enzymes found in saliva.
α-amylase. Amylase starts the digestion of starch and lipase fat before the food is even swallowed. It has a pH optima of 7.4. lysozyme. Lysozyme acts to lyse bacteria. lingual lipase. Lingual lipase has a pH optimum ~4.0 so it is not activated till entering an acidic environment.

41
Enzymes Minor enzymes include salivary acid phosphatases A+B,
N-acetylmuramyl-L-alanine amidase, NAD(P)H dehydrogenase-quinone, salivary lactoperoxidase, superoxide dismutase, glutathione transferase, aldehyde dehydrogenase, glucose-6-phosphate isomerase, tissue kallikrein. Cells: Possibly as much as 8 million human and 500 million bacterial cells per mL. The presence of bacterial products (small organic acids, amines, and mercaptans) causes saliva to sometimes exhibit foul odor.
H dehydrogenase-quinone, salivary lactoperoxidase, superoxide dismutase, glutathione transferase, aldehyde dehydrogenase, glucose-6-phosphate isomerase, tissue kallikrein. Cells: Possibly as much as 8 million human and 500 million bacterial cells per mL. The presence of bacterial products (small organic acids, amines, and mercaptans) causes saliva to sometimes exhibit foul odor.")
42
Biochemical composition of human saliva in relation to other mucosal fluids
Histatins are polypeptides which possess exceptional anti-fungal and anti-bacterial activities, but are nevertheless present only in saliva. Proline-rich proteins (PRPs) are members of a closely related family, of which the acidic PRPs are found solely in saliva. Mucins are a group of glycoproteins that contribute to the visco-elastic character of the mucosal secretions. Mucins have distinct tissue distributions and amino acid sequences. Other salivary proteins are present in one or more mucosal secretions.
 are members of a closely related family, of which the acidic PRPs are found solely in saliva. Mucins are a group of glycoproteins that contribute to the visco-elastic character of the mucosal secretions. Mucins have distinct tissue distributions and amino acid sequences. Other salivary proteins are present in one or more mucosal secretions.")
43
Lysozyme is an example of a component
belonging to an ancient self-defense system, whereas secretory immunoglobulin A (sIgA) is the secreted part of a adaptive immune system. Cystatins are closely related proteins which belong to a multigene family. Alpha-Amylase plays a specific role in digestion, but is nevertheless present in several body fluids. Kallikrein and albumin are components of blood plasma. But whereas albumin diffuses into the different mucosal secretions, kallikrein is secreted specifically by the mucosal glands.
 is the secreted part of a adaptive immune system. Cystatins are closely related proteins which belong to a multigene family. Alpha-Amylase plays a specific role in digestion, but is nevertheless present in several body fluids. Kallikrein and albumin are components of blood plasma. But whereas albumin diffuses into the different mucosal secretions, kallikrein is secreted specifically by the mucosal glands.")
44
the pH changes from being slightly acidic (at rest) to basic (pH 8) at ultimate stimulation. This increase in alkalinity is due to the increase of HCO3- in the saliva

45
Salivary Dysfunction Major types of disorders affect the salivary glands: one that results in salivary gland malfunction, whereby not enough saliva is produced, and one that results in salivary gland swelling. When the flow of saliva is insufficient or almost nonexistent.This condition - dry mouth (xerostomia). Hypothyroid states, diabetes mellitus, and HIV and hepatitis C infection have all been associated with xerostomia. The loss of saliva can have multiple deleterious consequences, including a constant sense of dryness (xerostomia), increased tooth decay, fungal infections and oral burning (Candidiasis), decreased or altered taste, difficulty speaking and swallowing, and recurrent salivary gland infections.
. Hypothyroid states, diabetes mellitus, and HIV and hepatitis C infection have all been associated with xerostomia. The loss of saliva can have multiple deleterious consequences, including a constant sense of dryness (xerostomia), increased tooth decay, fungal infections and oral burning (Candidiasis), decreased or altered taste, difficulty speaking and swallowing, and recurrent salivary gland infections.")
46
Too much or too little saliva can affect oral health and quality of life.
Hyposalivation leads to dental decay, oral yeast infections, taste problems, bad breath, difficulty speaking and swallowing, and recurrent salivary glands infections. The loss of saliva is not associated with the development of periodontal disease Hypersalivation can cause social problems and may be a sign of an underlying medical problem (stomatitis, pulpitis, parodontitis etc).
.")
47
ORAL ENVIRONMENT PLAQUE
Soft sticky, invisible film constantly forming in your mouth. Covers teeth and gums. Oral mucosa cells Saliva Bacteria Can be removed by brushing and flossing. Gram + cocci Gram + rods Gram – anaerobes (healthy mouth) (gingivitis) Formation / progression influenced by: Diet Host immune system Oral environment
 (gingivitis) Formation / progression influenced by: Diet. Host immune system. Oral environment.")
48
Taste Disorders Loss of taste Persistent unusual or unexpected tastes
Perversions of taste (for example, when something sweet tastes salty) Evaluation includes medical history review, head, neck and oral examination, diagnostic imaging, salivary function assessment, and testing of ability to taste and smell.
 Evaluation includes medical history review, head, neck and oral examination, diagnostic imaging, salivary function assessment, and testing of ability to taste and smell.")
49
Salivary Gland Swelling: Salivary gland swelling can occur when one of the ducts that carry saliva from the salivary gland to the mouth is blocked. Pain may occur, especially during eating. The most common cause of blockage is a stone. Salivary gland stones are most common in adults; 25% of those with stones have more than one. A stone can form from salts contained in the saliva. Blockage makes saliva back up inside the duct, causing the salivary gland to swell. A blocked duct and gland filled with stagnant saliva may become infected with bacteria.

50
Candidiasis

51
Mumps Mumps is an infection caused by a virus and can cause: Fever
Headache Swelling and tenderness of glands in one or both sides of the neck (called parotitis) Running nose and eyes, sore throat and ears particularly in young children. Occasionally serious complications of mumps infection can occur. These less common, but more serious symptoms include: A meningitis Ear infections which can lead to hearing impairment. Swelling and tenderness of the testicles in adult men (orchitis), and inflammation of the ovaries (oophoritis) in women, though it is very rare for these to cause serious complications such as infertility. Pancreatitis inflammation of the pancreas.
 Running nose and eyes, sore throat and ears particularly in young children. Occasionally serious complications of mumps infection can occur. These less common, but more serious symptoms include: A meningitis. Ear infections which can lead to hearing impairment. Swelling and tenderness of the testicles in adult men (orchitis), and inflammation of the ovaries (oophoritis) in women, though it is very rare for these to cause serious complications such as infertility. Pancreatitis inflammation of the pancreas.")
52
Mumps, certain bacterial infections, and other diseases (such as AIDS, Sjögren's syndrome, diabetes mellitus, and sarcoidosis) may be accompanied by swelling of the major salivary glands. Swelling also can result from cancerous or noncancerous tumors in the salivary glands. An injury to the lower lip may harm any of the minor salivary glands found there and block the flow of saliva.

Similar presentations







 BY. Dr. Shahzadi Tayyaba Hashmi DNT 353.>")




 Click here to launch video Click here to download print activity.>")






