Download presentation
Presentation is loading. Please wait.

1
Allergic Rhinitis and Sinusitis for Primary Care Providers
Steve Meixel, MD Waccamaw Community Care

2
Reference www.uptodate.com 2014 UpToDate
Pharmacology of allergic rhinitis Acute sinusitis and rhinosinusitis in adults

3
Why talk about Hay Fever and Sinusitis?
Very common: affects 10-30% of pop. Our environment: Lots of allergens Long allergy seasons People are not getting the treatment they need. Ineffective treatment = MORE problems.

4
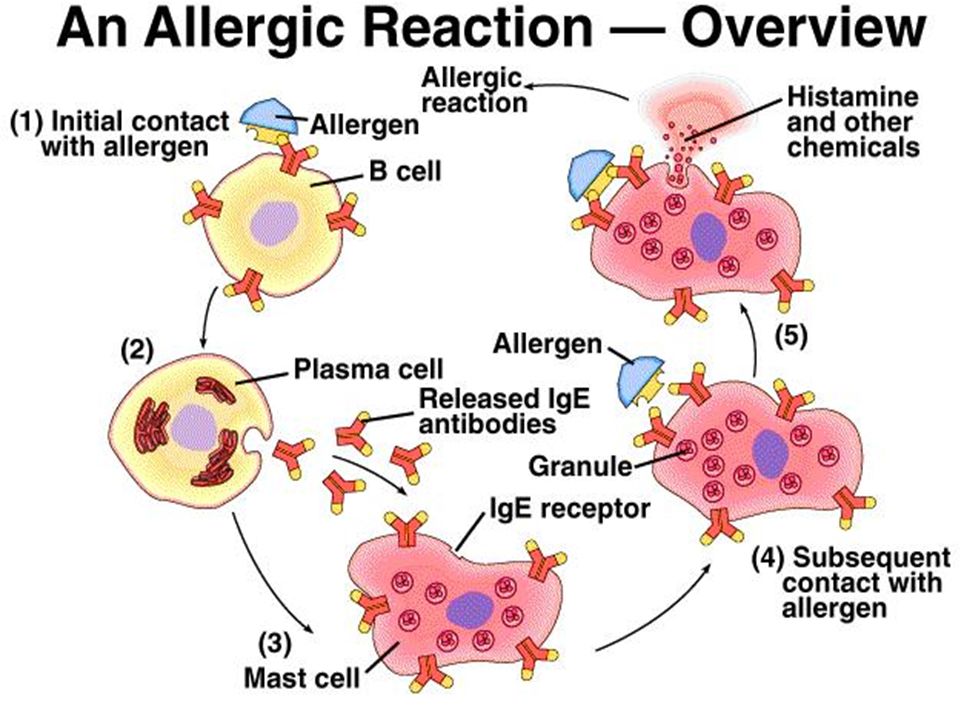
Types and Causes of Allergic Reactions

5
Symptoms of Allergic Rhinitis (Hay Fever):
Runny nose Sneezing Itchy eyes

6
How does pollen cause a problem?

8
Treatments: Allergen avoidance: Keep a symptom diary
Pharmacotherapy (nasal steroids are first line) Allergen immunotherapy (“allergy shots”)
 Allergen immunotherapy ( allergy shots )")
9
Decongestants open the airway
Sudafed (e.g. Claritin D) Phenylephrine (e.g. Dimetapp, lots of others) Afrin Nasal Spray BEWARE: Use only 5 days! (or rhinitis medicamentosa can develop) Caution: can cause problems with urination in MEN (prostatic obstruction)
 Phenylephrine (e.g. Dimetapp, lots of others) Afrin Nasal Spray. BEWARE: Use only 5 days! (or rhinitis medicamentosa can develop) Caution: can cause problems with urination in MEN (prostatic obstruction)")
10
Prostate Gland

11
How to Evaluate a Drug: STEP
The things that the patients care about. Safety Tolerability Efficacy Price

12
Nasal Steroids (Flonase, Nasonex, Rhinocort……)
Most effective single therapy More effective than antihistamines or antihistamine sprays Non-sedating Often also helps with eye itching Can work in 3 – 12 hrs. May take 7-10 days to reach full benefit

13
Nasal Steroids (Flonase, Nasonex, Rhinocort……)
Start at maximal dose and taper lower once controlled More expensive than antihistamines Caution with glaucoma Theme: EFFECTIVE! Start early, may need to use all season, $$

14
Different generations: same effect, but different bioavailability.
1st generation: Higher bioavailabilty Beclomethasone (Beconase AQ $196, Qnasl $159) Flunisolide (Nasarel $69) Budesonide (Rhinocort Aqua $135) 2nd generation: lower risk of systemic effects Fluticasone proprionate (Flonase $106) Fluticasone furoate (Veramyst $137) Mometasone furoate (Nasonex $158)
 Flunisolide (Nasarel $69) Budesonide (Rhinocort Aqua $135) 2nd generation: lower risk of systemic effects. Fluticasone proprionate (Flonase $106) Fluticasone furoate (Veramyst $137) Mometasone furoate (Nasonex $158)")
15
Nasal Steroids: Side Effects
Local irritation (2-10%): drying, burning, smell, taste Nosebleeds (2-12%): Scant blood: stop few days on side of bleed Frank epistaxis: may need to change type (I have had luck with aqueous)…or stop. Direct spray away from septum. Possible concerns: Glaucoma, Cataracts
: drying, burning, smell, taste. Nosebleeds (2-12%): Scant blood: stop few days on side of bleed. Frank epistaxis: may need to change type (I have had luck with aqueous)…or stop. Direct spray away from septum. Possible concerns: Glaucoma, Cataracts.")
16
Aqueous vs Dry Powder Aqueous: Dry Powder (Qnasl $159, Zetonna $227)
Tilt head forward (to avoid drainage to throat) Dry Powder (Qnasl $159, Zetonna $227) For pts who don’t like wet, run-off Tilt head back, hold breath, exhale thru mouth
 Dry Powder (Qnasl $159, Zetonna $227) For pts who don’t like wet, run-off. Tilt head back, hold breath, exhale thru mouth.")
17
Other Nasal Sprays Antihistamine: Combination (antihistamine/steroid):
Azelastine (bitter taste) Astelin ($194) Astepro ($171) Olopatadine Patanase ($194) Combination (antihistamine/steroid): Dymista (azelastine/fluticasone) ($182)
 Astelin ($194) Astepro ($171) Olopatadine. Patanase ($194) Combination (antihistamine/steroid): Dymista (azelastine/fluticasone) ($182)")
18
Oral Antihistamines 1St Generation: (diphenhydramine, chlorpheniramine, hydroxyzine, brompheniramine)– OTC Sedating, cross blood-brain barrier Implicated in fatal MVAs Geriatric problems: confusion, urinary hesitancy Problems in children: Impaired school performance Paradoxical agitation OTC cold Rx– linked to deaths in <2yo

19
Oral Antihistamines 2nd Generation: e.g. Loratadine, cetirizine, fexofenadine Avoid unwanted CNS effects Have anti-inflammatory properties No evidence that tolerance develops No evidence to support H1 & H2 (e.g. ranitidine) As effective as cromolyn
 As effective as cromolyn.")
20
Cromolyn sodium (NasalCrom)
Inhibits mast cell release of antihistamine Safe, even for children >2yo Dosing: 3-4x/day Works if used shortly before exposure E.g. visiting a home with a cat For allergic rhinitis: More effective if used just prior to allergy season. $9-13

22
Montelukast (Singulair)
Approved for allergic rhinitis & asthma Leukotriene receptor antagonist Good if cannot tolerate nasal sprays Rare side effects: depression, suicide $170/month

23
Ipratropium (Atrovent) Nasal
Controls profuse nasal discharge Not as effective as nasal steroids for sneezing, itching, nasal obstruction $130/ bottle

24
Therapies requiring caution
Nasal decongestants: rhinitis medicamentosa OK for <3-5d: At onset of treatment Before air travel Systemic steroids OK at start of treatment if symptoms severe Avoid steroid shots

25
Pregnant Women Allergen avoidance Nasal saline
Intermittent congestion: Nasal decongestant (for <5d) Persistent symptoms: Nasal budesonide (Rhinocort Aqua) Cromolyn Loratidine or cetirizine
 Persistent symptoms: Nasal budesonide (Rhinocort Aqua) Cromolyn. Loratidine or cetirizine.")
26
Important other things:
Avoid the allergens (pollen, mold) Keep windows closed Set car AC on “inside circulation” Cat out of the bedroom Saline (salt water) nose spray (or showers) Wash out the allergens Change air filters Keep diary of symptoms & be a detective
 Keep windows closed. Set car AC on inside circulation Cat out of the bedroom. Saline (salt water) nose spray (or showers) Wash out the allergens. Change air filters. Keep diary of symptoms & be a detective.")
28
Don’ts Don’t use nasal decongestant sprays for longer than 5 days.
Don’t use oral steroids frequently or longer than 2 wks. However, I frequently use a short course of steroids to arrest the allergies in a severely affected patient.

29
If nasal steroids are not effective alone…
Add a 2nd generation antihistamine or an antihistamine/decongestant Add a topical antihistamine nasal spray Antihistamine eye drops (for allergic conjunctivitis) Montelukast (Singulair) – especially if asthma also Atrovent Nasal
 Montelukast (Singulair) – especially if asthma also. Atrovent Nasal.")
30
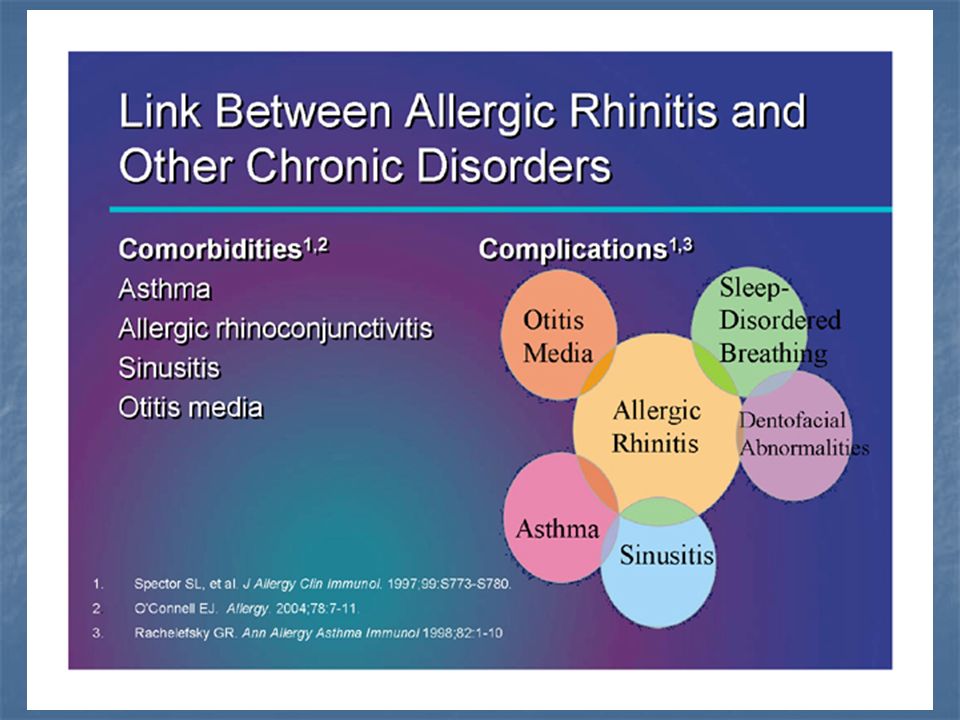
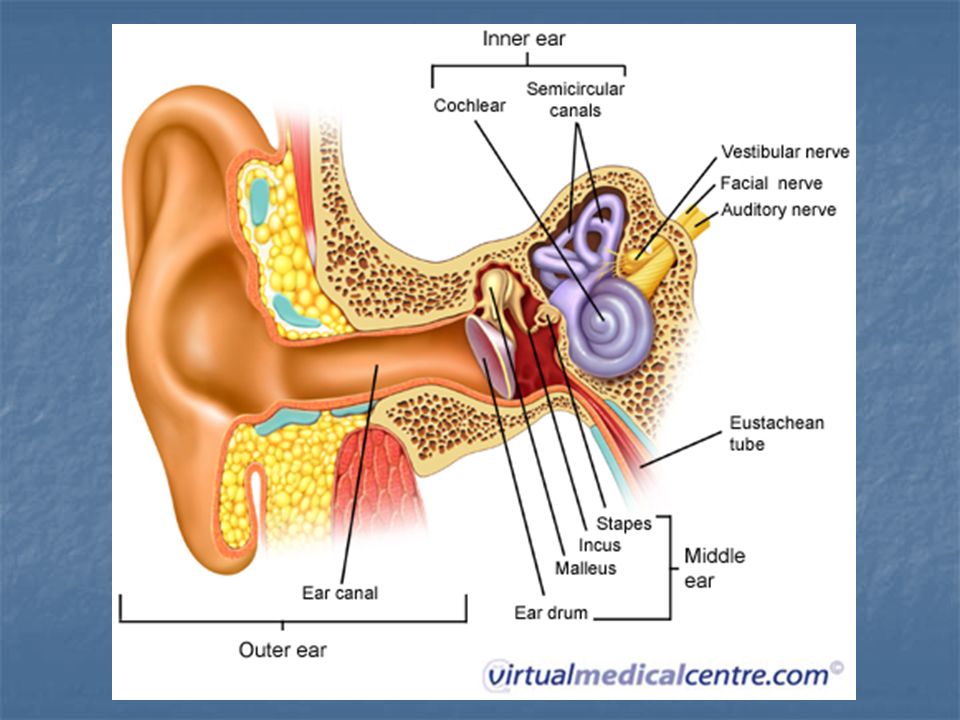
Complications: Asthma gets worse. Sinus infections Ear infections
Principle: Body cavities that get blocked get infected!

34
Referral: Children with persistent symptoms– for consideration of immunotherapy Patients who fail maximal therapy Coexisting asthma or nasal polyps Recurrent complications (e.g. otitis media) Intolerable side effects from treatments Pts. interested in immunotherapy Pts. requiring recurrent systemic steroids
 Intolerable side effects from treatments. Pts. interested in immunotherapy. Pts. requiring recurrent systemic steroids.")
35
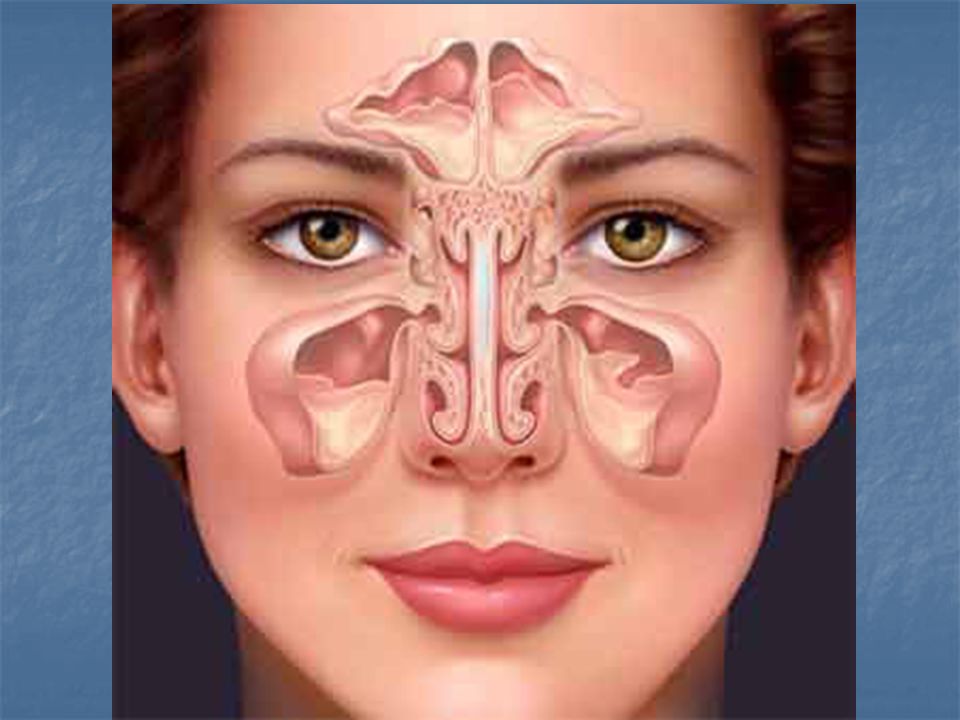
Sinusitis

36
Acute Rhinosinusitis (lasts < 4weeks)
Acute Viral Rhinosinusitis (AVRS): e.g. Cold: usually resolves in 7-10 d Acute Bacterial Rhinosinusitis (ABRS): Complicates AVRS in 0.5-2% 40-69% of ABRS clears spontaneously
: e.g. Cold: usually resolves in 7-10 d. Acute Bacterial Rhinosinusitis (ABRS): Complicates AVRS in 0.5-2% 40-69% of ABRS clears spontaneously.")
37
Clinical Problems: Antibiotics are not needed for AVRS
But 85-98% treat with antibiotics (1990) Problem: Cannot distinguish ABRS vs AVRS in first 10 days. How can we limit antibiotic use?
 Problem: Cannot distinguish ABRS vs AVRS in first 10 days. How can we limit antibiotic use")
38
Suspect ABRS ARS lasts > 10d with no improvement Severe symptoms:
T>102, purulent discharge, facial pain (x3d) Worse symptoms (“double sickening”) Pt was improving. Then worse symptoms after 5-6d.
 Worse symptoms ( double sickening ) Pt was improving. Then worse symptoms after 5-6d.")
39
Treatment of AVRS <10d = Supportive Care
1. Acetaminophen (< 3-4g/d) or NSAID 2. Nasal saline 3. +/- Nasal steroids: (NNT 15 = $$) Best in patients with h/o allergic rhinitis 4. Nasal decongestants <3-5d (or rebound) Not helpful in ABRS (continued)
 or NSAID 2. Nasal saline 3. +/- Nasal steroids: (NNT 15 = $$) Best in patients with h/o allergic rhinitis 4. Nasal decongestants <3-5d (or rebound) Not helpful in ABRS (continued)")
40
Treatment of AVRS 5. Oral decongestants: Not helpful for ABRS 6. Antihistamines: Not recommended. No evidence of benefit, + side effects 7. Mucolytics (e.g. Guaifenesin): No data to show benefit.
: No data to show benefit.")
41
Bacterial Sinusitis (ABRS)
ABRS is more likely if: > 10 days of symptoms Purulent D/C, facial pressure, nasal congestion

43
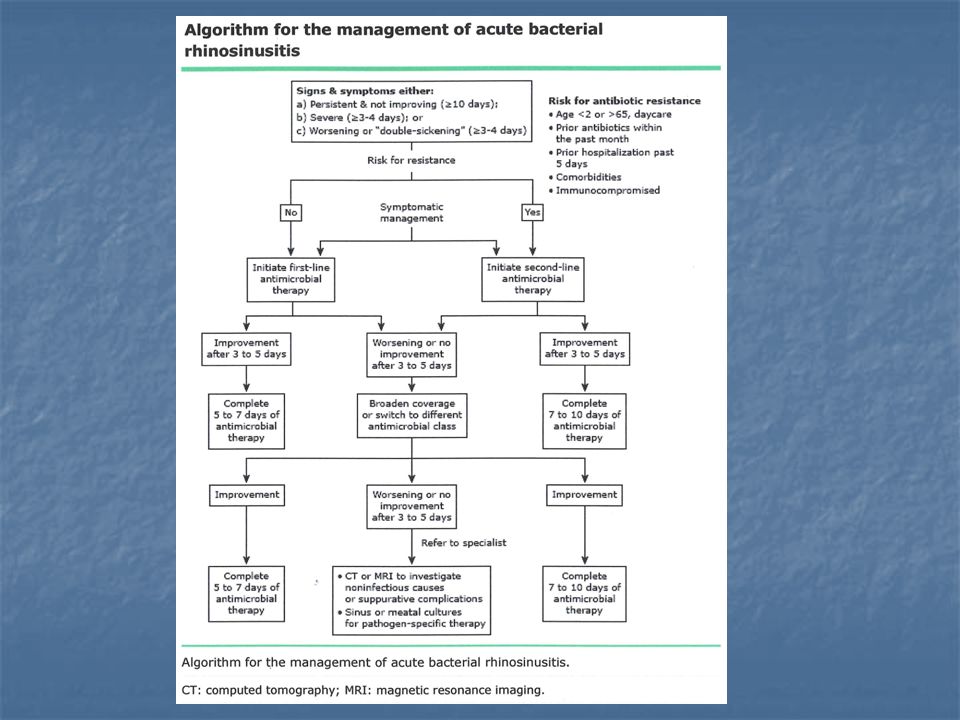
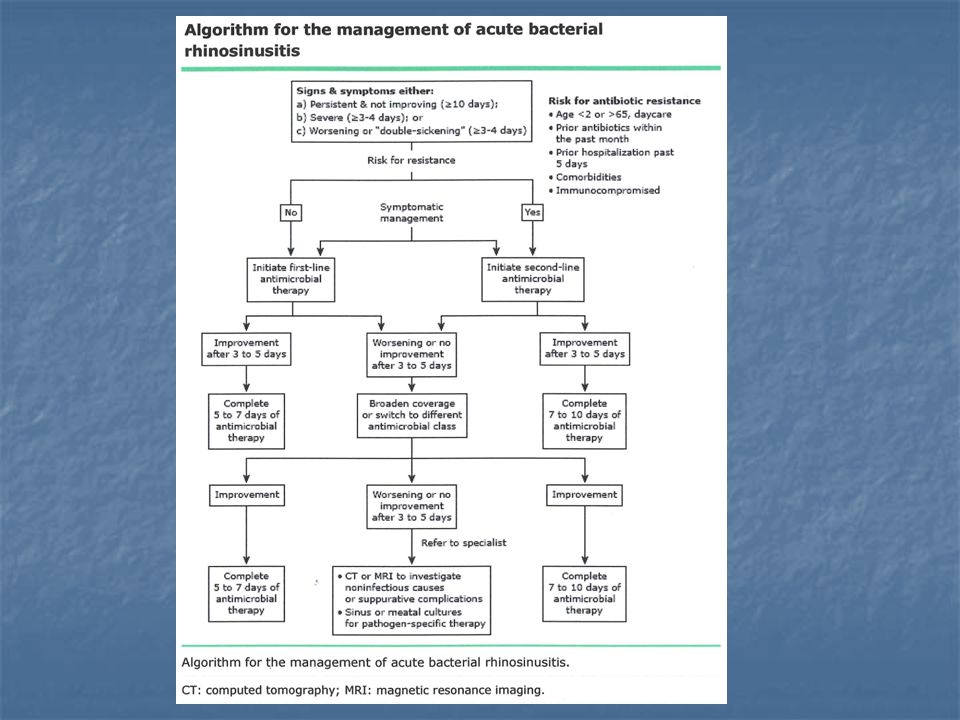
Treatment of ABRS May observe 3-7d if mild symptoms:
T< 101 (38.3) and mild pain Treat if no improvement or if worsens Start antibiotics if: Moderate symptoms with clinical ABRS Severe symptoms T>102, purulent discharge, facial pain x3d
 and mild pain. Treat if no improvement or if worsens. Start antibiotics if: Moderate symptoms with clinical ABRS. Severe symptoms. T>102, purulent discharge, facial pain x3d.")
44
Recommendation for penicillin non-allergic patients
Amoxicillin-clavulanate for 5-7d 500/125mg TID ($46 for 5d) or 875/125mg BID ($33 for 5d) 2000/125mg BID ($76 for 5d) if >65yo recently hospitalized Treated with antibiotic in last month immunocompromised
 or 875/125mg BID ($33 for 5d) 2000/125mg BID ($76 for 5d) if. >65yo. recently hospitalized. Treated with antibiotic in last month. immunocompromised.")
45
Penicillin-allergic patients
Doxycycline: 100mg bid x 5-7 d ($6-13 for 5d) Respiratory fluoroquinolone Levofloxacin: 500mg daily x 5-10 d ($107 for 5d) Moxifloxacin: 400mg daily x 5-10d ($141 for 5d)
 Respiratory fluoroquinolone. Levofloxacin: 500mg daily x 5-10 d. ($107 for 5d) Moxifloxacin: 400mg daily x 5-10d. ($141 for 5d)")
46
Not recommended due to increased bacterial resistance
Azithromycin Clarithromycin Trimethoprim-Sulfa Cephalosporins

47
Pregnant Patients Amoxicillin-clavulanate (class B)
Azithromycin for pen-allergic (class B) Don’t use Doxycycline (class D) Fluoroquinolones (class C)
 Don’t use. Doxycycline (class D) Fluoroquinolones (class C)")
48
Duration of Treatment 5-7 days is recommended
Meta-analysis of 12 trials showed no difference in cure rates between 3-6 days vs 6-10 days of treatment

49
2nd Line Treatment Amoxicillin-clavulanate 2000mg/125mg bid
Levofloxacin 500mg daily Moxifloxacin 400mg daily Recommended course is 7 – 10 days CT scan of sinuses if failure to improve.

50
Referral Early referral: Less urgent referral: High persistent fever
Severe headache Meningeal signs Orbital edema/visual disturbance Less urgent referral: Failure to respond to 1st & 2nd line Rx 3-4 episodes / year Chronic symptoms Pts w/ allergic rhinitis who may need immunotherapy

52
Hay Fever and Sinusitis
Any Questions????

Similar presentations