Download presentation
Presentation is loading. Please wait.

1
Bucharest Workshop ~ OSI Partners 17/18 th October 2008 Teresa Guthrie Centre for Economic Governance and AIDS in Africa

2
CEGAA aims to contribute to improved economic governance, fiscal policy and financial management and accountability, with specific attention to improving the response to HIV and AIDS. Through ~ economic and budget analysis research, training and capacity building, and advocacy activities With ~ civil society orgs, independent research agencies, parliamentarians and Ministries of Health and National AIDS Commissions.

3
Overview of this Presentation Potential scope for budget monitoring and expenditure tracking Different foci & methods in BMET Costing Budget monitoring Expenditure tracking Examples of evidence-based advocacy using BMET data Key decisions in developing the Project TORs

4
Transparency & Accountability ~ Govt Allocation & Expenditure Processes Govt Budget is a powerful economic policy tool to balance the revenue & expenditure, maintain fiscal discipline, and translate policies into services. Undermined by IMF/ WB conditionalities. Budget allocation is powerful indicator of the priority accorded to health (or other issue), more than policy or legislation, and are key to the sustainability of programmes. Participatory, transparent, accountable budget & expenditure systems indicate degree democracy in the country. Budget Allocations do not equate to actual Expenditure Monitoring of allocations & expenditure depends upon strong financial information systems!
, more than policy or legislation, and are key to the sustainability of programmes. Participatory, transparent, accountable budget & expenditure systems indicate degree democracy in the country. Budget Allocations do not equate to actual Expenditure Monitoring of allocations & expenditure depends upon strong financial information systems!.")
5
BMET compliments policy & service analysis & strengthens advocacy Policy Services BUDGET $$ Policy Analysis Prog.Evaluation BMET

6
Definitions Costing – determining required resources, quantities, their costs and calculating total cost for an intervention Budgeting – a plan to manage the available resources, within a specific timeframe (usually 1year) according to the project plan (intended allocations) Expenditure – those resources spent on particular interventions Adequacy – are the inputs sufficient to achieve intended goals – implies knowledge of how much is needed. Efficacy / Effective – achieves its intended outputs or outcomes – implies programme plan.

7
Definitions cont. Efficient – achieves its outputs with the best use of inputs/ resources – most cost-efficient. Allocative efficiency – best choice of type of intervention between different types of intervention (eg. Prevention activities vs treatment activities. Technical efficiency – best choice of intervention from same type of interventions (eg. Within treatment options, best and cheapest ARVs). Operational efficiency – intervention is run/ implemented as efficiently as possible. Programme outputs – immediate tangible products Programme outcomes – results of the outputs Programme impact –longer-term effects (the overall purpose for the intervention)
. Operational efficiency – intervention is run/ implemented as efficiently as possible. Programme outputs – immediate tangible products Programme outcomes – results of the outputs Programme impact –longer-term effects (the overall purpose for the intervention).")
8
8 Fiscal Cycle ~ Different Phases & Methods Assessment of Resource Need – costing analysis Budget Allocations – indication of intended PUBLIC expenditure Actual Expenditure – execution of budget. Can include all sources of funds and by all service providers Public Private Donor Budget Monitoring Process Actual amounts Revenue & tax Sector analysis Expenditure Analysis Process/finance channels Actual amounts Output analysis – interim indicators comparing with objectives of expenditure Outputs Social Auditing Effectiveness Quality Outcome analysis – long-term indicators. Impact assessment Life years saved Quality of life Reduced prevalence rates Causal link Effectiveness (CEA/CBA/CUA) Your use of the data will influence all these aspects National Provincial District
 Your use of the data will influence all these aspects National Provincial District.")
9
How much was spent How much was allocated How much is needed Through government Public Foreign Private Through private orgs/NGOs In strategic programs Targeted IEC Condoms PMTCT STI treatment VTC ARV treatment IO treatment Palliative services Social Impact Mitigation Staff training Research Beneficiaries? Outputs At global level At national level MOH Other ministries NGO, CSO, CBO At province level Tertiary, Secondary Primary level NGO, CSO, CBO At local level In strategic programs Based on need (idealistically?) Currently covered (reality?) Financial / Programmatic gaps Linking Resource Need Estimates to Allocation Analysis to Expenditure Estimates $$ $ $$$
 Currently covered (reality ) Financial / Programmatic gaps Linking Resource Need Estimates to Allocation Analysis to Expenditure Estimates $$ $ $$$.")
10
1. Costing Methods Costing - determining the expenditure required to purchase the resources/ good/ inputs needed to achieve an activity or strategy Budgeting - the allocation of resources to match requirements. Once the cost of an activity is determined, the total number of desired activities will then determine the desired funding (case of treatment).
..")
11
1. Costing cont. In costing we identify and measure all the inputs and all the outputs. Costs are always related to the outcomes they produce. Outcomes can also be called benefits or output. There are intermediate and final outcomes. Some examples: HIV treatment programmes: cost per life year gained HIV prevention programmes: cost per HIV case prevented At a more basic level, we often relate costs to certain activities, such as the cost of an inpatient day or the cost per outpatient visit

12
Costs to be included Direct Direct – all the expenses incurred in delivering the health service, including shared costs Indirect costs Indirect costs – those additional costs, usually from the perspective of the patient, in accessing treatment, eg. Transport, loss of productivity, etc Intangible costs Intangible costs – those difficult to identify and measure eg. The drawbacks due to illness, depression, loss of quality of life Recurrent costs Recurrent costs - Resources that are used up within one year or costs that are incurred on an annual basis Capital costs Capital costs - Resources that last for more than one year (buildings, medical equipment, furniture, training of staff on HIV medicine and ART etc). Shared costs Shared costs - resources will be used jointly by the ART programme and other programmes in the health facility
. Shared costs Shared costs - resources will be used jointly by the ART programme and other programmes in the health facility.")
13
2. Budget Monitoring Approach Using the central and sub-national budget documents Using the available line-items for the intended allocations for a sector (eg. Health), programme (eg. HIV/AIDS and STI), facility (eg. Hospitals/ clinics) Undertake simple analysis with the nominal figures to ascertain: Amount allocated – nominal & real terms (adjusted for inflation) Increases from previous year (or more) ~ trends Projected increases (if uses MTEF) Proportional priorities ~ shares of total exp & GDP Per capita allocation ~ adequacy (requires costing), regional comparison
, programme (eg. HIV/AIDS and STI), facility (eg. Hospitals/ clinics) Undertake simple analysis with the nominal figures to ascertain: Amount allocated – nominal & real terms (adjusted for inflation) Increases from previous year (or more) ~ trends Projected increases (if uses MTEF) Proportional priorities ~ shares of total exp & GDP Per capita allocation ~ adequacy (requires costing), regional comparison.")
14
(Public Health as share of total expenditure) 0% 2% 4% 6% 8% 10% 12% 14% 16% 18% 2000/12001/22002/32003/42004/52005/6 Mozambique South Africa Kenya Abuja target Namibia – Health specific Namibia - Total for MoHSS Source: Guthrie & Hickey, 2004. ABU, Idasa. Prioritisation of Health ~ proportional analysis

15
3. Expenditures Tracking ~ What do we want to know? To describe the financial flows and actual expenditures for HIV and AIDS: Who has promised/ committed/ allocated what? Who pays (sources)? Who manages the funds (financing agents)? Who provides the services (providers)? What was provided (functions/ASC: prevention, treatment, social mitigation, other sector activities)? What are the budget components (Objects of expenditure)? Who benefits from the spending (beneficiaries)? Compare the budgeted/ allocated/ committed / transferred amounts with the actual expenditures
. Who manages the funds (financing agents). Who provides the services (providers). What was provided (functions/ASC: prevention, treatment, social mitigation, other sector activities). What are the budget components (Objects of expenditure). Who benefits from the spending (beneficiaries). Compare the budgeted/ allocated/ committed / transferred amounts with the actual expenditures.")
16
Data Required to Understand Spending Programme/ Activity Programme/ Activity Programme/ Activity Programme/ Activity Programme/ Activity Programme/ Activity Programme/ Activity Programme/ Activity Adjusted from UNAIDS NASA approach.

17
Flow of resources from origin to end users: reconstruction of transactions AC Source Provider Functions B Objects of Expenditure Target Groups Agent

18
4. Output Monitoring Social Auditing Citizen Score Cards Service Satisfaction Surveys Quality assessment of services Counting numbers of beneficiaries, staff members, availability & quantity of drugs These activities are better carried out by the community members / beneficiaries of the services Clinical data – life years saved, QALYs, DALYs

19
Eg. BMET : TB treatment in SA Initially institutionalisation of TB pts Advent of DOTS – needed evidence to prove was more cost-effective than institutionalisation Then rolled out DOTS With advent of HIV/AIDS, co-infection rates increased Needed evidence to prove that ART would be cost- effective in reducing incidence of OIs (incl. TB), and that govt could afford to provide ARVs free to patients Now calling for integrated treatment of HIV/AIDS and TB, and needing evidence to prove that TB prophylaxis for HIV-patients is cost effective MDR-TB & XDR-TB… ?
, and that govt could afford to provide ARVs free to patients Now calling for integrated treatment of HIV/AIDS and TB, and needing evidence to prove that TB prophylaxis for HIV-patients is cost effective MDR-TB & XDR-TB… .")
20
Using Financial Information for Evidence-Based Political Decisions

21
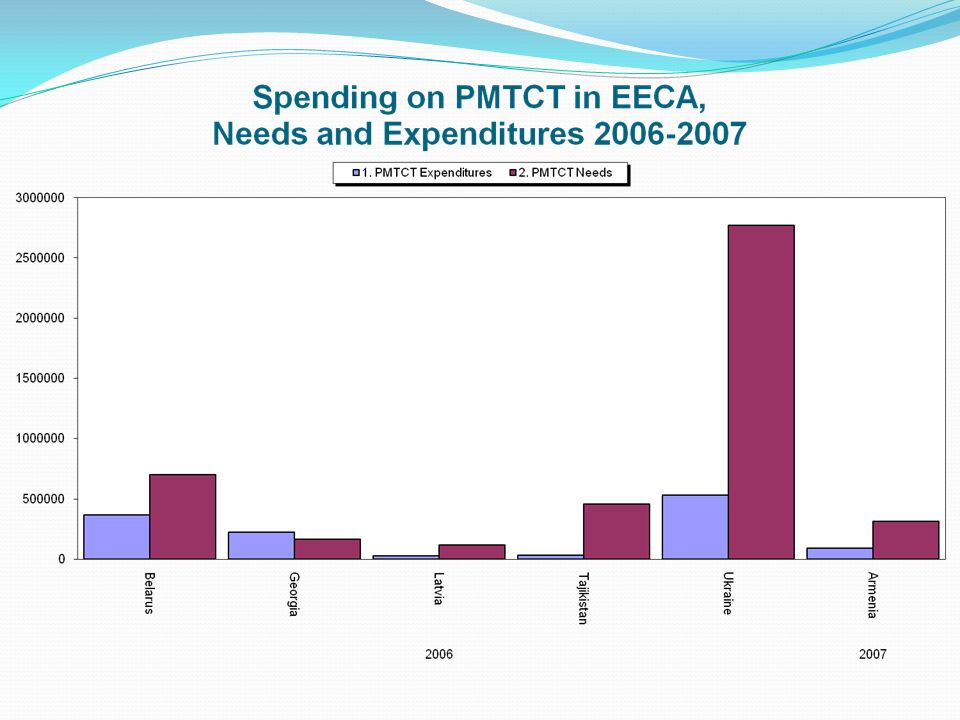
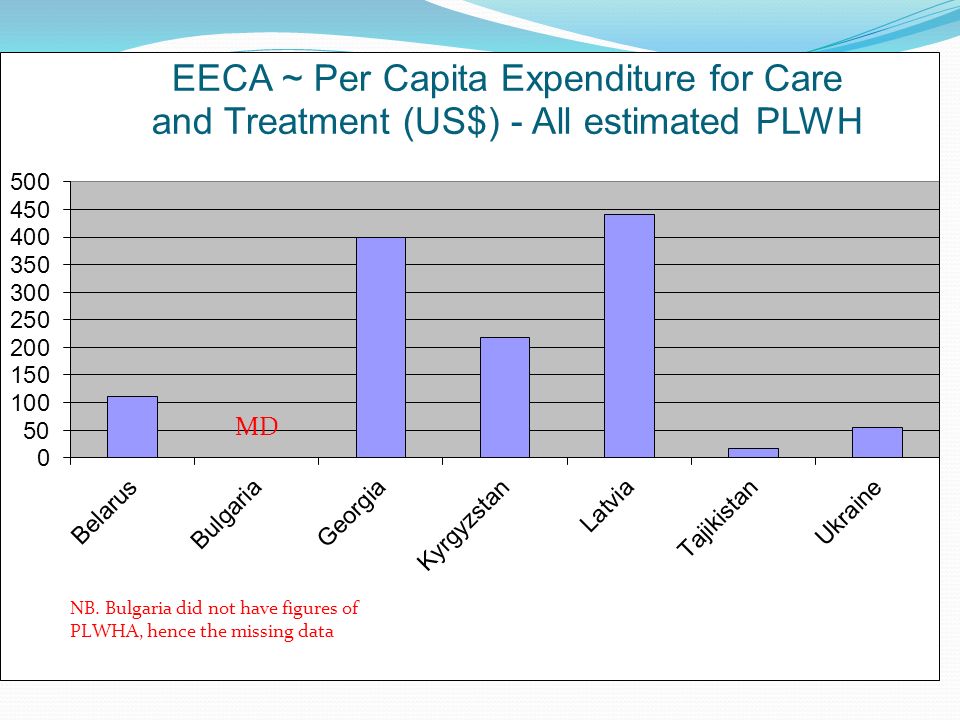
Financial Sources for HIV/AIDS in EECA

23
Composition of HIV international sources – Swaziland (05/06 & 06/07)
")
24
Sources of HIV/AIDS Funds in Swaziland - 50,000,000 100,000,000 150,000,000 200,000,000 250,000,000 300,000,000 350,000,000 400,000,000 Year Emalangenn International funds Public Funds International funds 239,520,821 220,816,750 Public Funds 32,835,809 136,915,968 2005/20062006/2007

25
Spending Priorities in Swaziland

26
Sources of HIV/AIDS Funds in Botswana (Pula)
")
27
AIDS Categories in Botswana

30
NSP Priorities vs Actual Spending - Zambia

31
*Armenia 2007, Bulgaria 2006-2007, Croatia 2006, Georgia 2006, Kazakhstan 2007, Kyrgyzstan 2006, Latvia 2006, Republic of Moldova 2007, Tajikistan 2006

35
Opportunities for evidence-based political decisions ADEQUACY OF FUNDING – PUBLIC & EXTERNAL Public commitments-meeting national/international commitments ~ long-term sustainability Comparison to costed NSP estimates of required resources – funding gap analysis Centralised funding and spending with low funds for the sub-national level Data not disaggregated according to national and sub- national levels Discrepancies between allocations and actual expenditures ~ measurement of absorptive capacity, leakages, transaction costs

36
Opportunities for evidence-based political decisions (2) ALLOCATIVE DECISIONS – PRIORITIES Meeting national priorities (aligned to NSP?) Balance between programmes ~ unsustainability of treatment costs without adequate prevention interventions ~ allocative efficiency Equity in allocations ~ between geographical areas, providers, beneficiaries & according to need EFFICIENCY OF SPENDING Provides varying unit costs for interventions, allows comparison of technical efficiency Identifies poor absorption capacity ~ allows for exploration of factors: bottlenecks, dumping etc.
 ALLOCATIVE DECISIONS – PRIORITIES Meeting national priorities (aligned to NSP ) Balance between programmes ~ unsustainability of treatment costs without adequate prevention interventions ~ allocative efficiency Equity in allocations ~ between geographical areas, providers, beneficiaries & according to need EFFICIENCY OF SPENDING Provides varying unit costs for interventions, allows comparison of technical efficiency Identifies poor absorption capacity ~ allows for exploration of factors: bottlenecks, dumping etc.")
37
Opportunities for evidence-based political decisions (3) C OORDINATION, H ARMONISATION AND A LIGNMENT Alignment of the actual HIV/AIDS spending to NSP – public and external Agent analysis shows who determines use of funds Identifies poor harmonisation – duplicative financing & reporting, high transaction costs I NSTITUTIONALIZATION OF NASA Within the Monitoring and Evaluation (M&E) framework Using standardised financial information/ reporting mechanisms
 C OORDINATION, H ARMONISATION AND A LIGNMENT Alignment of the actual HIV/AIDS spending to NSP – public and external Agent analysis shows who determines use of funds Identifies poor harmonisation – duplicative financing & reporting, high transaction costs I NSTITUTIONALIZATION OF NASA Within the Monitoring and Evaluation (M&E) framework Using standardised financial information/ reporting mechanisms")
38
Opportunities for evidence-based political decisions (4) E NHANCED T RANSPARENCY, A CCOUNTABILITY & E CONOMIC G OVERNANCE Increased pressure (& desire) for mutual accountability by all players Promotes a (legal) framework to ensure all partners report through a national resource tracking system Link framework to the National Resource Mobilisation and Management Strategy Using the framework to harmonise standards of costing among different partners Ensures transparent procurement systems & best pricing within and between countries & regions
 E NHANCED T RANSPARENCY, A CCOUNTABILITY & E CONOMIC G OVERNANCE Increased pressure (& desire) for mutual accountability by all players Promotes a (legal) framework to ensure all partners report through a national resource tracking system Link framework to the National Resource Mobilisation and Management Strategy Using the framework to harmonise standards of costing among different partners Ensures transparent procurement systems & best pricing within and between countries & regions")
39
Opportunities for evidence-based political decisions (5) S TANDARDIZATION & C OMPARABILITY Ensures standard classification of spending & activities within & between countries & regions Provides comprehensive list of possible interventions Resource needs estimates Classification standardised with NASA Package of interventions Future requirements (funding gap) by programmes Comparison of TFRR & TE
 S TANDARDIZATION & C OMPARABILITY Ensures standard classification of spending & activities within & between countries & regions Provides comprehensive list of possible interventions Resource needs estimates Classification standardised with NASA Package of interventions Future requirements (funding gap) by programmes Comparison of TFRR & TE")
40
So how to go about it…. Broad consultation to discuss and decide what are the key issues requiring advocacy to bring about change And how can budgetary and expenditure data strengthen the advocacy campaign Be clear about your purpose

41
Determining the purpose & intended outcomes What are the key issues that you feel require an advocacy response? What is your advocacy goal & intended outcomes? What data is required to provide evidence to support the advocacy strategy? Who will be the key audience of the findings? Who will be the likely supporters and the likely opposition? What will be the focus/ topic of the project – OST, IDUs, HIV/AIDS, TB, health generally, health systems strengthening, ART?

42
Planning the Project – Terms of Reference The scope of the project: Which phase/s of the budget are being considered (need assessment, costing, resource allocation, processes), budgeted allocations analysis, expenditure analysis, output analysis, impact analysis) Which years are to be covered Which sources of funds (public and/or external and/or private, OOPE) Which providers of services – all, only central or only district level, specific facilities, eg hospitals/ schools, etc etc? Will the outputs and outcomes measured? Against what? Efficiency analysis? (CBA, CEA, CUA?) Is analysis of the beneficiary groups required? Is analysis of the objects of expenditure required?
 Is analysis of the beneficiary groups required. Is analysis of the objects of expenditure required .")
43
Resource Tracking Process The broad steps in expenditure analysis: 1. Developing the project ToR ~ agree on purpose (advocacy goals), scope & methods & partners 2. Planning and preparation 3. Training & capacity building 4. Data Collection, Processing & Analysis 5. Preliminary findings validation & identification of advocacy campaigns / strategies 6. Final Report & Dissemination 7. Advocacy campaign implementation 8. On-going BMET by organisations involved
, scope & methods & partners 2. Planning and preparation 3. Training & capacity building 4. Data Collection, Processing & Analysis 5. Preliminary findings validation & identification of advocacy campaigns / strategies 6. Final Report & Dissemination 7. Advocacy campaign implementation 8. On-going BMET by organisations involved.")
44
Possible Country-Level Partnership Arrangements The CORE Team could be made up of: An organisation/s with economic or research skills A Community level organisation &/or a strong advocacy org Association of PLWHAs or PLWD/ Chln & Youth / Gender network (depending on your focus) Members of the CORE team should be able to commit 2 or 3 people, 50% of their time, for at least 2yrs, hopefully 3yrs. The REFERENCE group could include other key stakeholders whose input /assistance is necessary Broader stakeholder group to identify issues, advocacy, etc Select one org to be the country Co-ordinating agent Identify suitable organisations to provide the tech. support

45
Challenges in Monitoring Allocations & Expenditure Budget documents: Do not give detail Not actual expenditure Non-standardised Some donor contributions off- budget Limited CS participation in allocative decisions Allocations not based on need/ equity Not used as a planning tool Expenditure records: Not available/ accessible to CS Not disaggregated (by programme/ facility / district) Donors do not provide actual expenditure by recipients (vs commitmts/ disbursmts) NHA data impt but not detailed sufficiently (esp.public sources) FOI laws in few countries or not used for accessing public expenditure records.
 Donors do not provide actual expenditure by recipients (vs commitmts/ disbursmts) NHA data impt but not detailed sufficiently (esp.public sources) FOI laws in few countries or not used for accessing public expenditure records.")
46
CSO Challenges in BMET Stronger on advocacy side but often lacking technical capacity on ‘number- crunching’ Stronger on the social auditing, citizen score cards, survey satisfaction surveys but lacking skills for assessing efficiency of spending, absorptive capacity BMET requires long-term commitment ito of HR and building capacity and transferring skills Lack human capacity and usually over-stretched Reliant of project-based funding – unreliable, unsustainable, no investment in institutional devmt

47
Thank You For more information contact: Teresa Guthrie Centre for Economic Governance and AIDS in Africa Email: teresa@cegaa.org Teresa.cegaa@gmail.com Tel: +27-82-872-4694 Fax: +27-21-425-2852

Similar presentations











efficiencies and sustainability Simelela, N., Sipho, S., Sozi, C., Damisoni, H.,>")











 HIV modelling for in-country ownership solutions – generation of evidence IAS Conference, Washington DC, 19-20 July.>")