Download presentation
Presentation is loading. Please wait.

1
PneumoconiosisPneumoconiosis

2
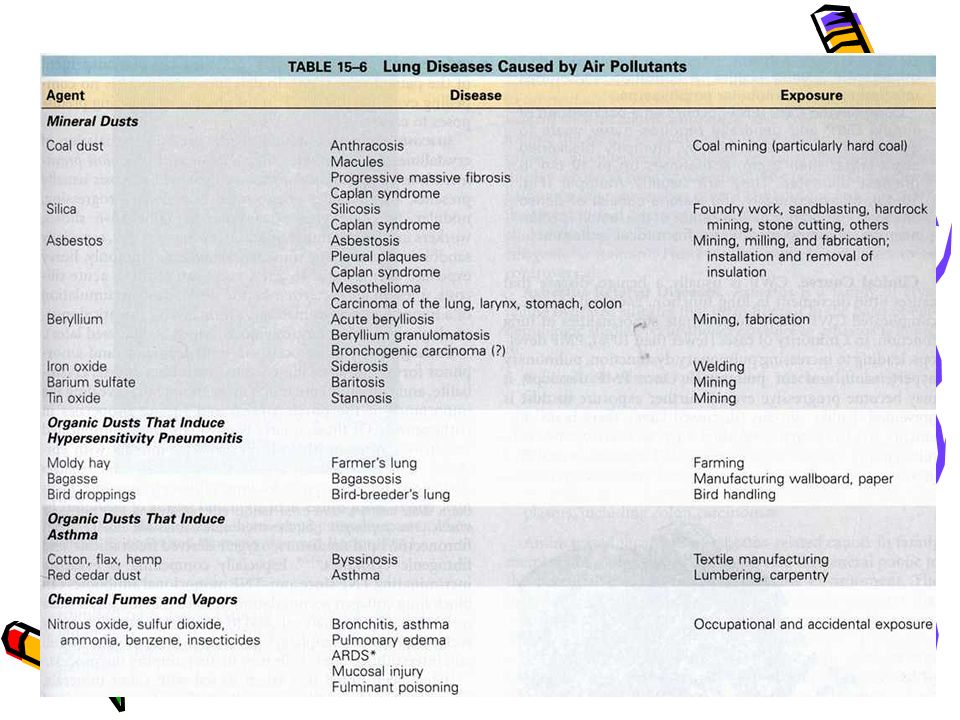
Definition Non neoplastic lung reaction to inhalation of mineral dusts encountered in the workplace. Also includes diseases induced by organic, inorganic particulates and chemical fumes and vapors. Important to diagnose as they are “occupational lung diseases.”e.g. silica, coal, asbestos Some dusts e.g. tin, iron are innocuous

3
Nomenclature According to the causative agent – silicosis Occupation eg knife grinders lung=silicosis

5
Normal protective mechanisms Mucociliary apparatus >10 μm diameter, deposit in bronchi & bronchioles and removed in the mucociliary escalator. Intra-alveolar macrophages- phagocytosis of particles & expectorated. Some go through interstitium into lymphatics. Very Small particles behave like gas & exhaled

6
Normal protective mechanisms Nose & trachea traps all particles >10 μm & 50% of 3μm Mucociliary blanket 2-10 μm removed in the mucociliary escalator. Alveolar macrophages <2 μm removed Very small particles are not phagocytosed,but exhaled.

7
Factors affecting fibrogenic potential Amount of dust retained in the lung (concentration, duration, clearence mechanisms) Size, shape and bouyancy of particles(aerodynamic diameter) (1-5μ size dangerous sized particles reach the periphery : bronchioles & alveoli) Additional effects of other irritants (smoking) Solubility & physiochemical reactivity
 Size, shape and bouyancy of particles(aerodynamic diameter) (1-5μ size dangerous sized particles reach the periphery : bronchioles & alveoli) Additional effects of other irritants (smoking) Solubility & physiochemical reactivity")
8
Factors affecting (cont…) Solubility & cytotoxicity of particles Small particles dissolve in pulmonary fluids → acute toxicity Larger,non soluble persist in lung parenchyma Some dusts directly penetrate the epithelial cells into the interstitium. Physiochemical reactivity Direct injury to tissue (free radicals )e.g. Quartz Fibrosing pneumoconiosis (eg silicosis)
e.g. Quartz Fibrosing pneumoconiosis (eg silicosis).")
9
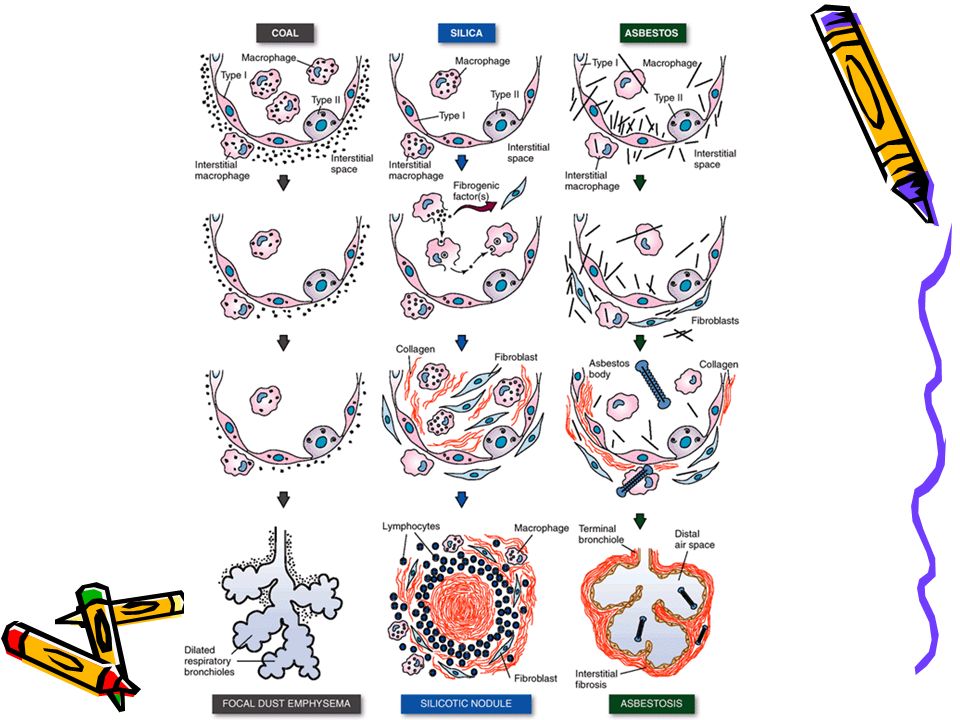
Pathogenesis of fibrosis Ingested dusts trigger macrophages to release chemical mediators that trigger fibrosis (TNF, IL 1,PDGF). Persistent release of factors causes fibrosis Migrating macrophages to lymphatics trigger immune reaction Fibrosis (nodular-silica, interstitial – asbestos ??)
.")
10
Pathogenesis Inhalation Escape removal by defence apparatus Particles penetrate epithelium → direct injury Fibrosis Engulfment by alveolar & interstitial macrophages → lymphatics → lymph node (modify immune response )
")
11
Coal workers pneumoconiosis (CWP) Associated with coal mining industry Carbon + silica (anthracosilicosis) Classification Asymptomatic anthracosis (anthracite –coal) Simple CWP- no dysfunction Complicated CWP- (progressive massive fibrosis PMF)
 Associated with coal mining industry Carbon + silica (anthracosilicosis) Classification Asymptomatic anthracosis (anthracite –coal) Simple CWP- no dysfunction Complicated CWP- (progressive massive fibrosis PMF)")
12
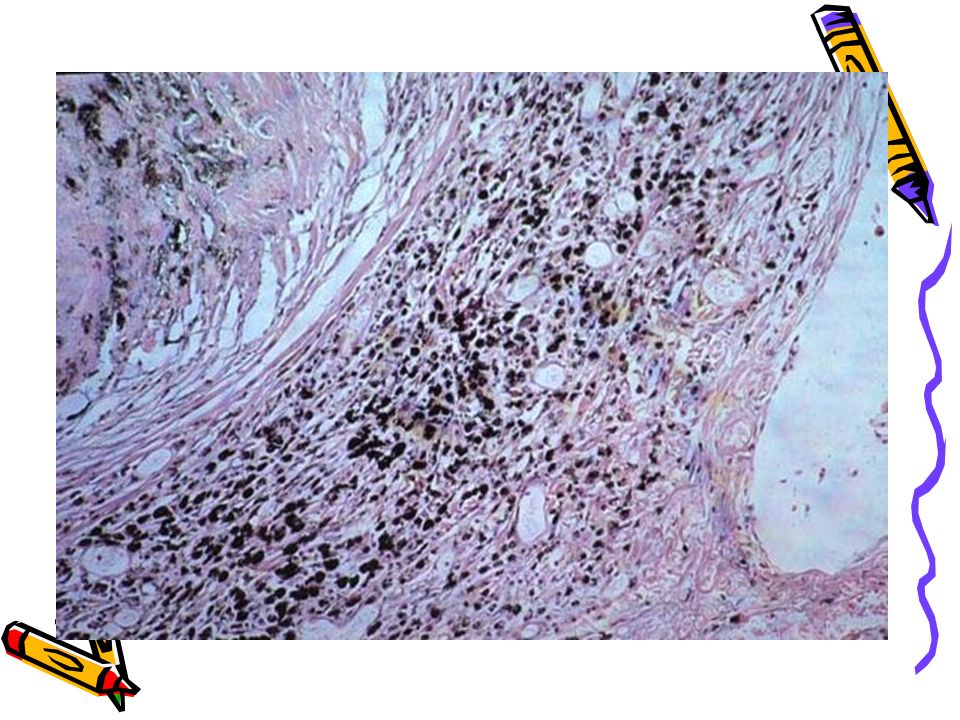
Anthracosis (urban dwellers) morphology Gross Streaks of anthracotic pigment in lymphatics and draining hilar lymph nodes Microscopy Carbon pigment in alveolar and interstitial macrophages,in connective tissue and lymphatics and lung hilus.
 morphology Gross Streaks of anthracotic pigment in lymphatics and draining hilar lymph nodes Microscopy Carbon pigment in alveolar and interstitial macrophages,in connective tissue and lymphatics and lung hilus.")
13
Simple CWP Gross :Coal macules (1-2mm) & Coal nodules >upper lobes and upper zones of lower lobes Microscopy: Carbon laden macrophages & delicate collagen fibres. Adjacent to respiratory bronchioles initially (where dust settles), later interstium & alveoli. Dilatation of respiratory bronchioles –focal dust emphysema
, later interstium & alveoli. Dilatation of respiratory bronchioles –focal dust emphysema.")
14
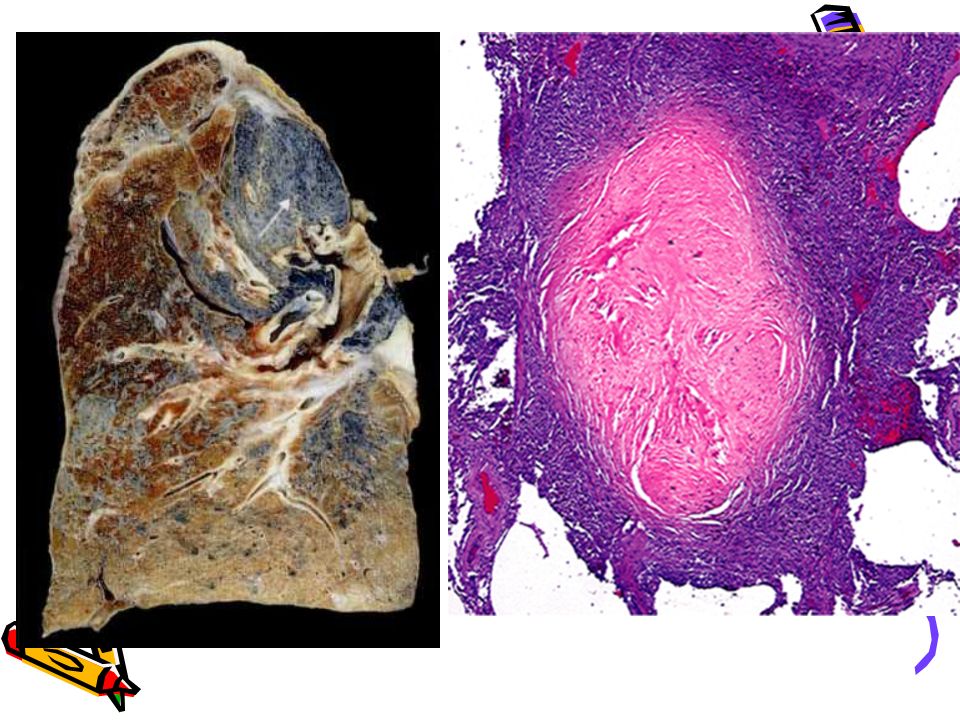
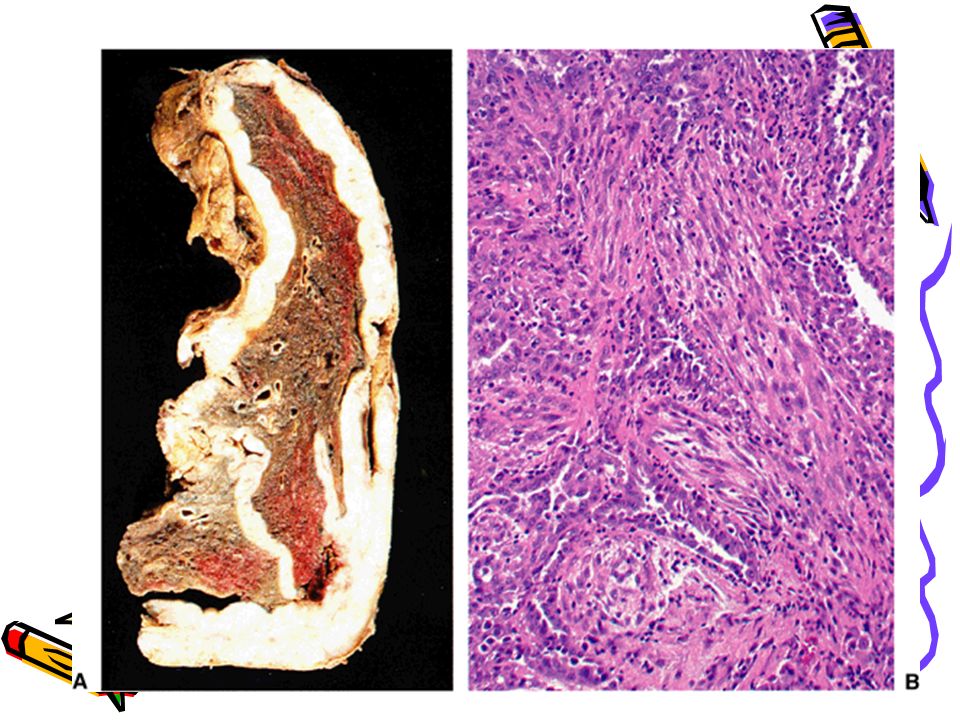
Complicated CWP Gross Multiple.,>2 cm,v dark scars Microscopy: Dense collagen and carbon pigment. Central necrosis (+/-)
.")
15
Clinical course Usually asymptomatic with little decrease of lung function PMF pulmonary dysfunction (restrictive) Pulmonary hypertension, cor pulmonale Progressive even if further exposure to dust is prevented ↑ chronic bronchitis and emphysema No association with TB or carcinoma
 Pulmonary hypertension, cor pulmonale Progressive even if further exposure to dust is prevented ↑ chronic bronchitis and emphysema No association with TB or carcinoma")
20
Caplans syndrome 1 st described in coal workers, may be seen in other pneumoconiosis ?? Immunopathologic mechanism Rheumatoid arthritis (RA) + Rheumatoid nodules (Caplan nodules) in the lung Rheumatoid arthritis + pneumoconioses Caplans nodule = necrosis surrounded by fibroblasts,monocytes and collagen s/s RA > lung symptoms
 + Rheumatoid nodules (Caplan nodules) in the lung Rheumatoid arthritis + pneumoconioses Caplans nodule = necrosis surrounded by fibroblasts,monocytes and collagen s/s RA > lung symptoms.")
21
Silicosis Silicosis-nodular fibrosing disease after 20-40 yrs exposure to silica Sand blasters,mine workers,stone cutting,polishing of metals,ceramic manufacturing etc. (Acute silicosis following massive exposure –alveolar lipoproteinosis like. Rapidly progressive disease. )
.")
22
Pathogenesis Fibrogenic activity depends on physical form, association with other minerals. Crystalline silica (quartz) more toxic. (Amorphous forms talc, mica less toxic) Size 0.2-2μm more dangerous Silica particles ingested by alveolar macrophages, kill them and release fibrogenic factors. Released silica ingested again. Recruitment of lymphocytes and macrophages Fibrotic silicotic nodule
 more toxic. (Amorphous forms talc, mica less toxic) Size 0.2-2μm more dangerous Silica particles ingested by alveolar macrophages, kill them and release fibrogenic factors. Released silica ingested again. Recruitment of lymphocytes and macrophages Fibrotic silicotic nodule.")
23
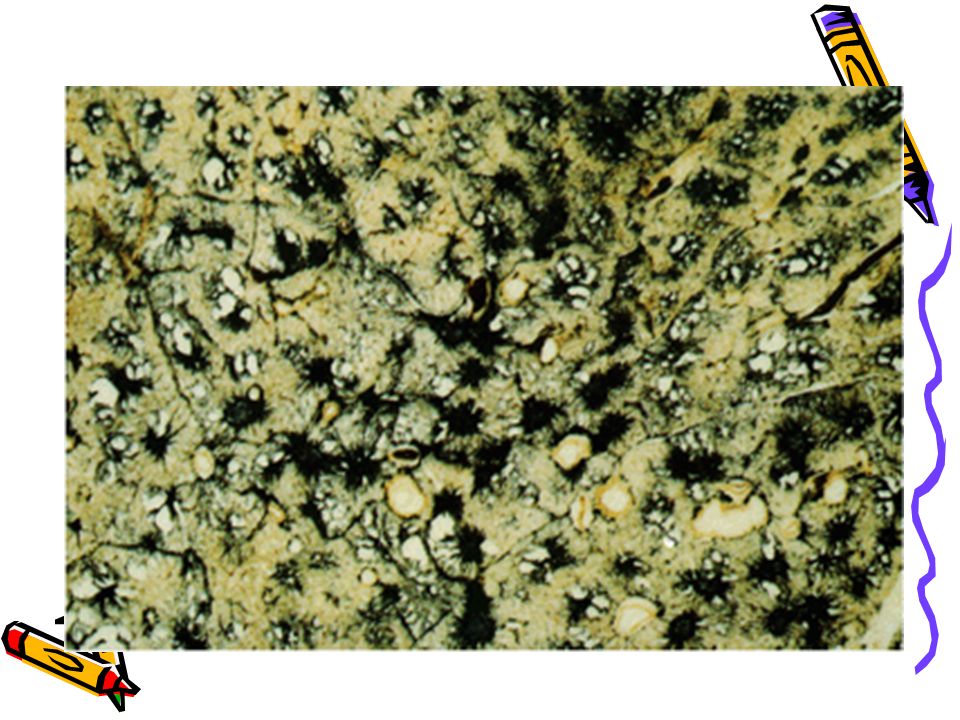
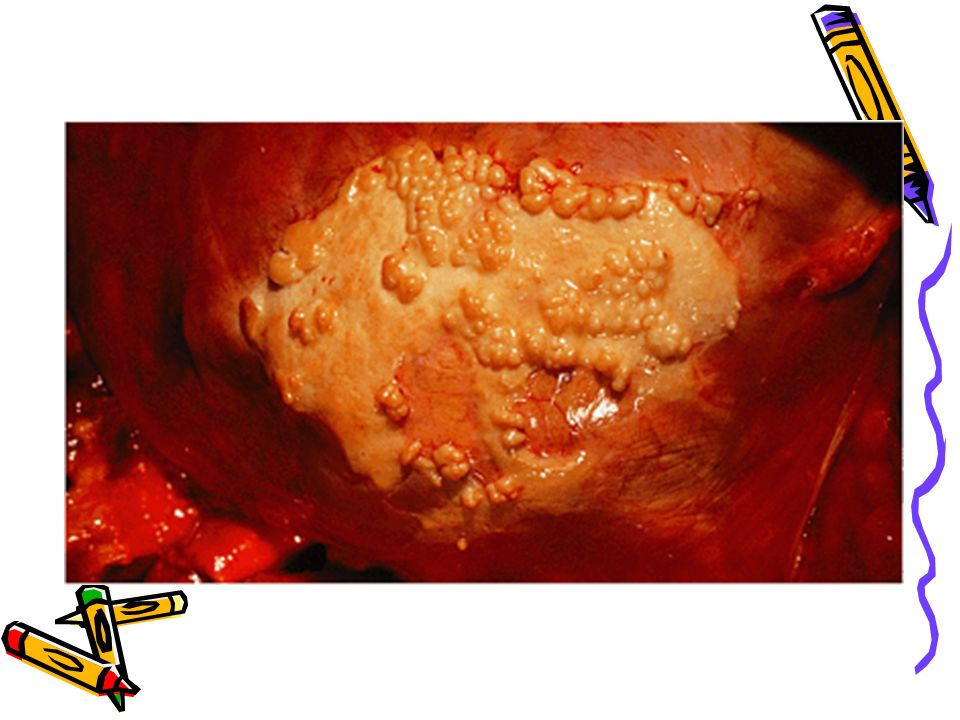
Gross Morphology Discrete pale to black nodules <1cm dia. Upper zone of lungs Hard collagenous scars-central softening Fibrosis in hilar lymph nodes and pleura Enlarged fibrotic LN with peripheral (eggshell) calcification PMF nodules >2 cm dia+ silicosis
 calcification PMF nodules >2 cm dia+ silicosis.")
24
Microscopy Concentric hyalinized collagen surrounded by condensed collagen,fibroblasts & lymphocytes. Birefringent silica particles (polarized light) Nodules incorporate normal lung tissue into themselves.
 Nodules incorporate normal lung tissue into themselves..")
26
Clinical features Early :X Ray fine nodularity in upper zones of lungs. Eggshell calcification in hilar LN PFT normal/moderately affected initially PMF: Progressive disease even after exposure stopped. X ray nodules >2 cm dia. PFT markedly ↓ Associated tuberculosis (↓CMI) Carcinogenic ??
 Carcinogenic .")
27
Prevention Air handling equipment in work place Use of face masks.

28
Asbestos related diseases Fibrous plaques-focal/diffuse Pleural effusion Parenchymal interstitial fibrosis (asbestosis-diffuse interstitial process) Lung carcinoma Malignant Mesothelioma Extrapulmonary malignancies- larynx,?colon
 Lung carcinoma Malignant Mesothelioma Extrapulmonary malignancies- larynx, colon")
29
Asbestos related disease Asbestos = unquenchable Asbsetos is resistant to physical and chemical destruction and is therefore used for fire proofing, insulation, brake lining etc. Construction material Ship demolition industry

30
Forms of asbestos Serpentine Curly,more used in industry e.g.chrysotile. less pathogenic Breaks into fragments Fibrogenic Impacts in upper airways & removed by mucociliary apparatus & more soluble-leached out Not associated with mesothelioma Amphibole straight & stiff e.g. crocidolite more pathogenic Resists breaking into fragments Fibrogenic Align in airstream & go deep,penetrate epithelium,enter interstitium 8 μm long more fibrogenic Associated with mesothelioma

31
Pathogenesis Fibrogenic potential like other inorganic dusts Tumour initiator and promoter Asbestos fibers localized in distal airways (close to mesothelium) release reactive free radicals. Absorption of carcinogens on asbestos fibres e.g. smoking

32
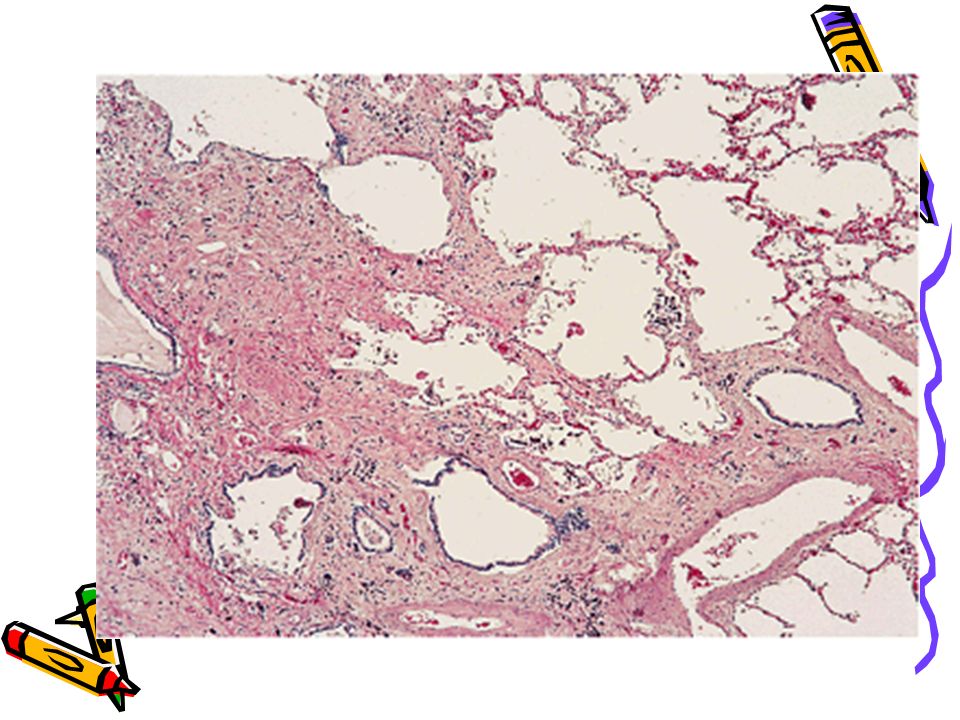
Morphology Diffuse pulmonary interstitial fibrosis Begins in the lower lobes & subpleurally (silica &CWP >upper) Honeycomb lung Pleural plaques
 Honeycomb lung Pleural plaques")
33
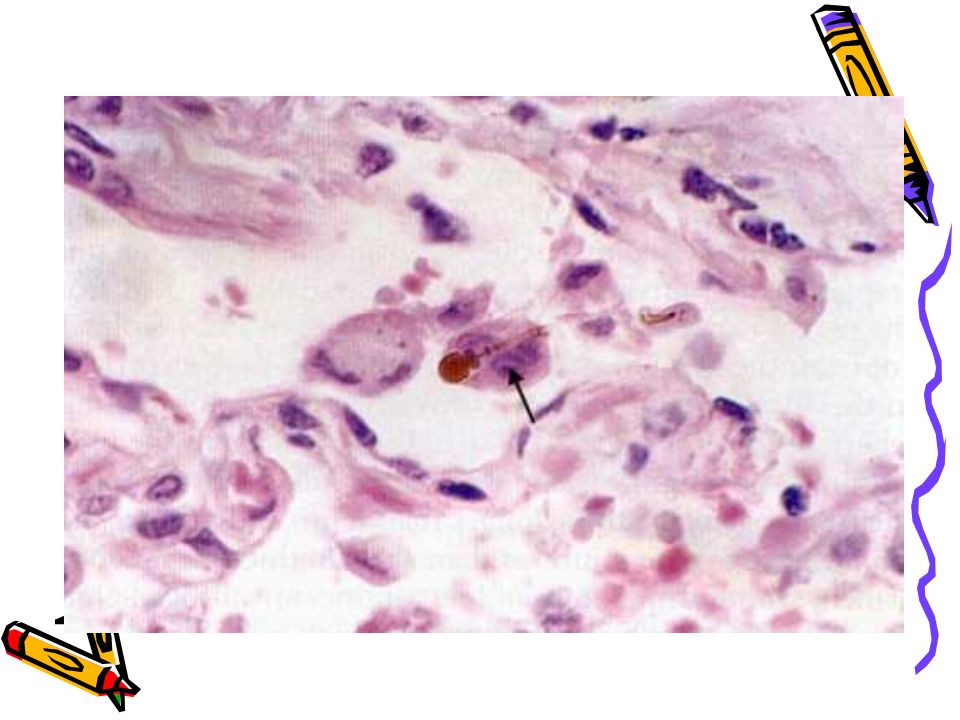
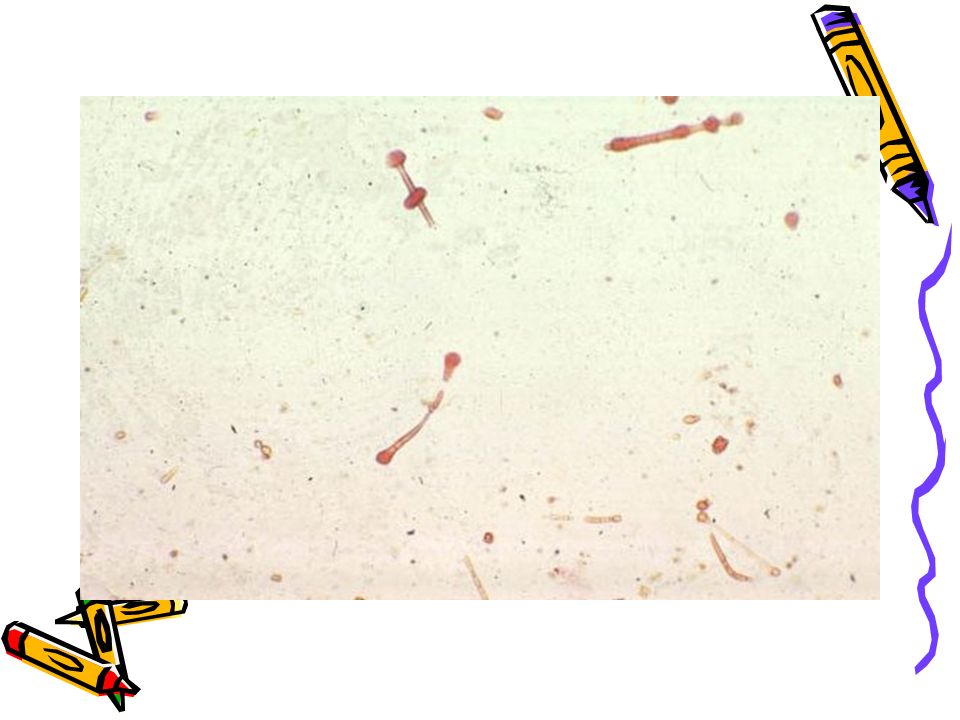
Microscopy Interstitial fibrosis around respiratory bronchioles and alveolar ducts, involves adjacent alveoli Asbestos bodies –golden brown fusiform or beaded rods with a tranluscent centre (asbestos fibre coated by iron containing proteinaceous material) Trapping & narrowing of pulmonary arteries
 Trapping & narrowing of pulmonary arteries")
38
Clinical course Dypsnoea Cough with sputum May progress to respiratory failure, cor pulmonale Cancer

42
Idiopathic pulmonary fibrosis This is characterised by diffuse interstitial inflammation and fibrosis resulting in severe hypoxemia and cyanosis in the late stage Synonyms:-- Chronic interstitial pneumonitis Hamman-Rich Syndrome Cryptogenic fibrosing alveolitis

43
Pathogenesis Sequence of events:-- Injury to alveolar wall Interstitial oedema Accumulation of inflammatory cells(alveolitis) Type 1 pneumocytes injured Hyperplasia of type2 pneumocyte Proliferation of fibroblasts
 Type 1 pneumocytes injured Hyperplasia of type2 pneumocyte Proliferation of fibroblasts")
44
Pathogenesis(contd.) Fibrosis of alveolar walls and alveolar exudate Loss of architecture of lung Cause:-?immune mechanism
 Fibrosis of alveolar walls and alveolar exudate Loss of architecture of lung Cause:- immune mechanism")
46
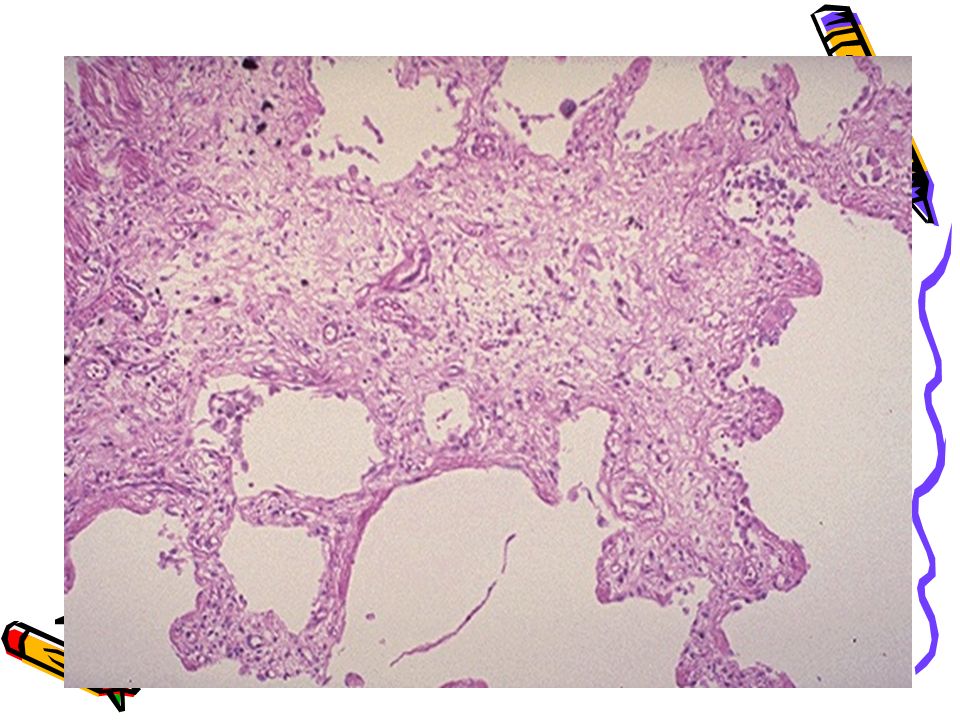
Morphology(contd..) END-STAGE:- Spaces lined by cuboidal /columnar epithelium separated by inflammatory fibrous tissue(Honey- comb lung) (end stage lung same in all conditions)
 END-STAGE:- Spaces lined by cuboidal /columnar epithelium separated by inflammatory fibrous tissue(Honey- comb lung) (end stage lung same in all conditions)")
Similar presentations




>")














 r Thin elastin-rich connective component containing.>")


