Download presentation
Presentation is loading. Please wait.

1
Amber Leon Jeanine Mills Erin Prasad Nutrition Assessment and Therapy 1 Winter 2012

2
http://www.medmovie.com/mmdatabase/Me diaPlayer.aspx?ClientID=89&TopicID=925 http://www.medmovie.com/mmdatabase/Me diaPlayer.aspx?ClientID=89&TopicID=925 A diagnosis of Metabolic Syndrome means that a person is at increased risk for developing ◦ Cardiovascular Disease (2 times as likely) ◦ Type 2 Diabetes Mellitus (5 times as likely) ◦ Stroke
 ◦ Type 2 Diabetes Mellitus (5 times as likely) ◦ Stroke")
3
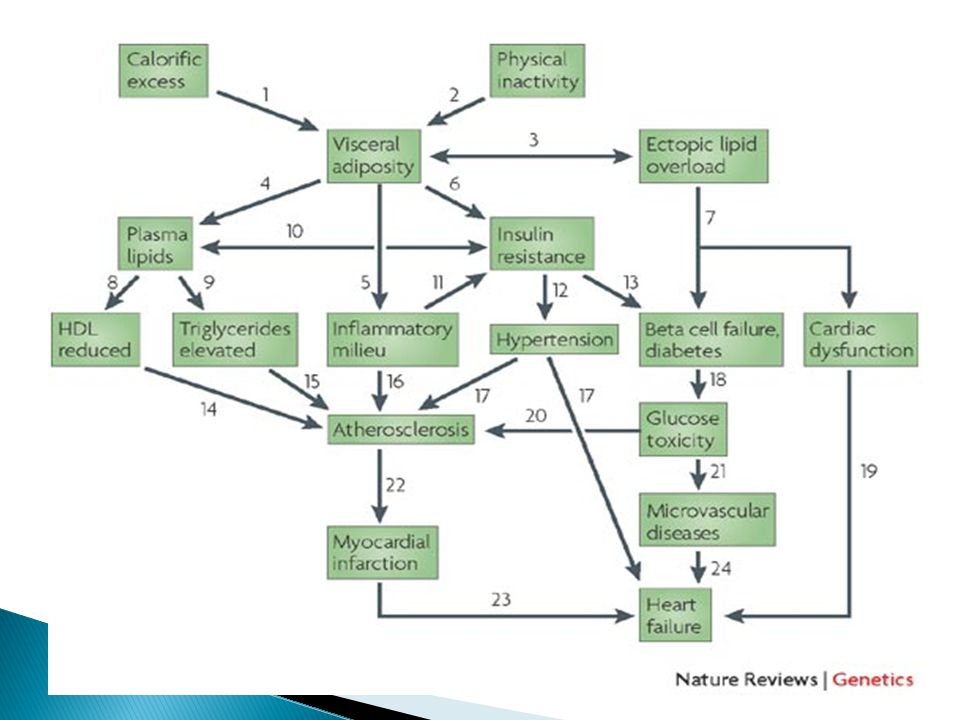
Metabolic syndrome represents the clustering of several risk factors and is not a disease unto itself. In 1988 Gerald M. Reaven proposed insulin resistance as the underlying factor and named the constellation of abnormalities Syndrome X. Insulin resistance may underlie the pathogenesis of metabolic syndrome. Or insulin resistance may result from the increased visceral adipose tissue (VAT)
.")
4
Fat distribution seems to be related to metabolic function with centrally obese people at higher risk of metabolic syndrome and it’s associated diseases than peripherally obese people.

6
VAT products that may activate components of the inflammatory pathway and inhibit insulin signaling. ◦ Free fatty acids and their metabolites ◦ Cytokines (ex: tumor necrosis factor alpha) ◦ Adiponectin (hormone released from adipose tissue) decreases, furthering insulin resistance. VAT is a risk factor for coronary artery disease, dyslipidemia hypertension, stroke, type 2 diabetes and Metabolic Syndrome
 ◦ Adiponectin (hormone released from adipose tissue) decreases, furthering insulin resistance. VAT is a risk factor for coronary artery disease, dyslipidemia hypertension, stroke, type 2 diabetes and Metabolic Syndrome.")
7
3 out of these 5 must be present for diagnosis Central Obesity Impaired Glucose Tolerance Hypertension Dyslipidemia ◦ Elevated Serum Triglicerides ◦ Lowered HDL Level Additional symptoms include Prothrombotic state high fibrinogen or plasminogen activator inhibitor [-1] in the blood Proinflammatory state elevated high-sensitivity C-reactive protein in the blood
![ 3 out of these 5 must be present for diagnosis Central Obesity Impaired Glucose Tolerance Hypertension Dyslipidemia ◦ Elevated Serum Triglicerides ◦ Lowered HDL Level Additional symptoms include Prothrombotic state high fibrinogen or plasminogen activator inhibitor [-1] in the blood Proinflammatory state elevated high-sensitivity C-reactive protein in the blood](http://images.slideplayer.com/23/6673984/slides/slide_7.jpg " 3 out of these 5 must be present for diagnosis Central Obesity Impaired Glucose Tolerance Hypertension Dyslipidemia ◦ Elevated Serum Triglicerides ◦ Lowered HDL Level Additional symptoms include Prothrombotic state high fibrinogen or plasminogen activator inhibitor [-1] in the blood Proinflammatory state elevated high-sensitivity C-reactive protein in the blood")
8
Genetics Smoking Sedentary lifestyle High calorie diet High-fat diet Ethnicity

9
For Diagnosis Patient must have 3 out of 5 defining symptoms Screening/Labs ◦ Waist Circumference > 40 inches in males >35 inches in females ◦ Blood Pressure >140/90 >130/85 if insulin resistance present ◦ Fasting Blood Glucose > 110mg/dl ◦ Serum Triglycerides > 150mg/dl ◦ Serum HDL < 40mg/dl for males < 50mg/dl for females

10
To increase mortality and decrease the co-morbidities associated with Metabolic Syndrome. Weight Reduction ◦ specifically reduction of visceral adipose tissue and decreased waist circumference (waist to hip ratio, Index of Central Obesity) Maintain normal blood glucose levels Improve lipid profile (increase HDL, lower triglycerides) Lower blood pressure Decrease Systemic Inflammation
 Maintain normal blood glucose levels Improve lipid profile (increase HDL, lower triglycerides) Lower blood pressure Decrease Systemic Inflammation.")
11
Dash Diet ◦ Designed to reduce hypertension ◦ Low sugar ◦ Low fat ◦ High fiber Carbohydrate Counting/Exchanges ◦ normalization of blood glucose Fruit and Vegetable intake ◦ May help to lower blood pressure ◦ May help to lose weight ◦ May replace other more refined carbohydrates Omega 3 Fats ◦ Reduction of inflammation Refer for and Encourage physical activity ◦ Improved glucose tolerance ◦ Improved blood pressure ◦ Improved lipid profile ◦ Improved cardiovascular fitness and endurance ◦ Improved depression

12
Calculate calories for weight loss ◦ 7% weight loss has been shown to be enough to reverse a Metabolic Syndrome diagnosis Protein within AMDR ◦ 10-35% of calories Fat within AMDR ◦ 20-35% of calories ◦ Emphasis on omega 3 and unsaturated fatty acids Carbohydrate within AMDR ◦ 45-65% of calories ◦ Emphasis on whole foods sources ◦ Emphasis on maintaining blood sugar levels as close to normal as possible. Fluids ◦ 35ml/kg or 1ml/kcal

13
Blood Glucose ◦ Insulin ◦ Oral medications Sulfonylureas, Meglitinides Biguanides Thiazolidinediones Alpha-glucosidase inhibitors DPP-4 inhibitors Cholesterol ◦ Statins ◦ Bile acid binding resins ◦ Cholesterol absorption inhibitors ◦ Combination cholesterol absorption inhibitor and statin ◦ Fibrates ◦ Niacin ◦ Combination statin and niacin ◦ Omega-3 Fatty Acids Blood Pressure ◦ Diuretics ◦ Beta-blockers ◦ ACE inhibitors ◦ Angiotensin II receptor blockers ◦ Alpha-2 receptor Agonist ◦ Combined alpha and beta- blockers ◦ Central agonists ◦ Peripheral adrenergic inhibitor ◦ Vasodialoator

14
Insulin resistance ◦ Chromium polynicotinate, ◦ Maitake mushrooms ◦ Green tea polyphenols ◦ Antioxidants ◦ Alpha lipoic acid ◦ Cinnamon ◦ Oat beta-glucan ◦ Omega 3 fatty acids ◦ Holy Basil Abnormal blood lipids ◦ Omega-3 fatty acids ◦ Niacin ◦ Oat beta-glucan ◦ Holy Basil Blood Pressure ◦Garlic ◦Omega-3 fatty acids ◦calcium ◦magnesium ◦vitamin C ◦Miatake Mushrooms Anti Inflammatory ◦ B-vitamins B6, B12, Folate ◦ Omega 3 fatty acids ◦ Turmeric ◦ Ginger ◦ Holy Basil

15
In 2006 The IDF (international diabetes foundation) estimated that 20-25% of the World population has Metabolic Syndrome. ◦ Prevalence is increasing in the adult population worldwide ◦ Prevalence is increasing in the US among children and adolescents Secondary associated conditions include ◦ Compromised renal function ◦ Polycystic ovary syndrome ◦ Non-alcoholic fatty-liver disease ◦ Non-alcoholic steatohepatitis ◦ Gestational diabetes mellitus ◦ Inflammation ◦ Depression Metabolic Syndrome is COMPLICATED The causes and symptoms overlap and contribute to one another. Pharmacological interventions improve some symptoms while exacerbating others People with this diagnosis are likely to be overwhelmed and feeling hopeless about their ability to improve their health. Diet and Exercise lifestyle changes can improve patients health dramatically.

Similar presentations








 75% of your cholesterol is.>")



 and Drug Therapy in Different Risk Categories Risk Category LDL Goal (mg/dL)>")





 are obese. 17% (12.5 million) of children 2—19 years are obese. Top leading.>")

