Download presentation
Presentation is loading. Please wait.

1
Endocrine System Chapter 16

2
Overview Overall goal of endocrine system: maintain a stable internal environment (homeostasis) Endocrine glands are “ductless glands” Endocrine glands secrete hormones which travel through the blood to a target cell Receptor must be present on target cell

3
Endocrine vs Nervous System
Both systems function to maintain homeostasis Main differences: Feature Endocrine System Nervous System Effector cells Target cells throughout the body Postsynaptic cells in muscle and glandular tissue only Chemical messenger Hormone-chemical Neurotransmitter Distance traveled by messenger Long – in blood Short – across synaptic cleft Regulatory effects Slow to appear; long-lasting Appear rapidly; short

4
Endocrine vs Nervous System

5
Major Endocrine Glands

6
Classification of Hormones
Classified by Function Tropic hormones: target other endocrine glands and stimulate their growth & secretion Sex hormones: target reproductive tissues Anabolic hormones: stimulate anabolism in their target cell

7
Chemical Classifications of Hormones

8
How Hormones Work Hormones bind to receptors on target cells
Lock & key Hormone-receptor interactions produce regulatory changes within the target cell Ex: initiating protein synthesis; activation/inactivation of enzymes; opening/closing of ion channels

9
How Hormones Work Synergism: combinations of hormones have a greater effect on the target cell compared to a single hormone acting alone Permissiveness: a small amount of one hormone allows a second hormone to exhibit its full effect on the target cell Antagonism: two hormones produce opposite effects

10
Regulation of Hormone Secretion
Hormone secretion is controlled by a negative feedback loop Ex: parathyroid hormone (PTH) and blood calcium levels (fig 16-10) Ex: insulin and blood glucose levels
 and blood calcium levels (fig 16-10) Ex: insulin and blood glucose levels.")
11
Endocrine Feedback Loop

12
Hyper vs Hyposecretion
Tumors or abnormalities of the endocrine glands cause secretion of too much or too little hormone Hypersecretion: production of too much hormone Hyposecretion: production of too little hormone Results in lack of target cell response Also caused by target cell insensitivity

13
Pituitary Gland Also called hypophysis
Located on ventral surface of brain, inferior to the hypothalamus “Master gland” because functions are crucial to life Composed of two parts: Anterior Pituitary and Posterior Pituitary

14
Anterior Pituitary Hormones secreted from Anterior Pituitary:
Growth Hormone Prolactin Trophic hormones Thyroid-stimulating hormone (TSH) Adrenocorticotropic hormone (ACTH) Gonadotropic hormones Follicle-stimulating hormone (FSH) Luteinizing hormone (LH)
 Adrenocorticotropic hormone (ACTH) Gonadotropic hormones. Follicle-stimulating hormone (FSH) Luteinizing hormone (LH)")
15
Growth Hormone Growth Hormone (GH) – promotes growth by stimulating protein anabolism Increased protein anabolism allows increased growth rate Target cells: Promotes growth of bone and muscle GH has a hyperglycemic effect; antagonist of insulin Hyperglycemic effect because GH stimulates fat metabolism Interaction vital to maintaining homeostasis of blood glucose levels GH stimulates fat metabolism Shift cells away from glucose catabolism towards lipid catabolism for an energy source Less glucose is used by cells; causes hyperglycemia

16
Growth Hormone Abnormalities
Hypersecretion Prior to ossification of the epiphyseal plates hypersections of GH results in rapid skeletal growth Gigantism After closure of epiphyseal plates hypersecretion causes cartilage to continue to form new bone Acromegaly Distorted appearance; enlarged hands, feet, face, jaw; thickened skin

18
Growth Hormone Abnormalities
Hyposecretion Results in stunted body growth pituitary dwarfism Treated with genetically engineered growth hormone

19
Prolactin (PRL) Also called lactogenic hormone
Initiates milk secretion (lactation) Target cells: Mammary glands During pregnancy PRL promotes development of breasts At birth PRL stimulates milk production
 Target cells: Mammary glands. During pregnancy PRL promotes development of breasts. At birth PRL stimulates milk production.")
20
Prolactin Abnormalities
Hypersecretion: Lactation in non-nursing women Disruption of menstrual cycle Impotence in men Hyposecretion: Insignificant unless mother wishes to breastfeed

21
Trophic Hormones Review: a trophic hormone stimulate effects of other endocrine glands Trophic hormones released from anterior pituitary gland: Thyroid-stimulating hormone (TSH) Adrenocorticotropic hormone (ACTH) Gonadotrophic hormones Follicle-stimulating hormone (FSH) Luteinizing hormone (LH)
 Adrenocorticotropic hormone (ACTH) Gonadotrophic hormones. Follicle-stimulating hormone (FSH) Luteinizing hormone (LH)")
22
Thyroid-stimulating hormone (TSH)
Promotes and maintains growth and development of thyroid gland Required for thyroid gland to secrete its hormones

23
Adrenocorticotropic hormone (ACTH)
Promotes and maintains normal growth and development of the cortex (outer portion) of the adrenal gland Required for adrenal cortex to secrete its hormone
 of the adrenal gland. Required for adrenal cortex to secrete its hormone.")
24
Gonadotrophic hormones
Target cells: gonads (testes & ovaries) Follicle-stimulating hormone (FSH) Females: Stimulates growth & development of an ovum that is released each month during ovulation Stimulate estrogen release from the ovaries Males Stimulates development of seminiferous tubules and maintains sperm production in the testes
 Follicle-stimulating hormone (FSH) Females: Stimulates growth & development of an ovum that is released each month during ovulation. Stimulate estrogen release from the ovaries. Males. Stimulates development of seminiferous tubules and maintains sperm production in the testes.")
25
Gonadotrophic hormones
Luteinizing hormone (LH) Females: Triggers ovulation Promotes development of corpus luteum which secretes progesterone and estrogen; these hormones help maintain pregnancy Males: Stimulates cells of the testes to synthesize and secrete testosterone
 Females: Triggers ovulation. Promotes development of corpus luteum which secretes progesterone and estrogen; these hormones help maintain pregnancy. Males: Stimulates cells of the testes to synthesize and secrete testosterone.")
26
Control of Anterior Pituitary Secretion
The hypothalamus releases chemical called releasing hormones which influence hormone secretion from the anterior pituitary gland This regulatory mechanism is a negative feedback loop

27
Posterior Pituitary Hormones secreted from Posterior Pituitary:
Antidiuretic Hormone (ADH) Oxytocin (OH)
 Oxytocin (OH)")
28
Antidiuretic Hormone (ADH)
Target cells: kidney Prevents formation of large volumes of dilute urine Antidiuresis Helps conserve water balance Example: Blood is hypertonic change detected by osmoreceptors ADH is released water reabsorbed in kidneys and returned to blood

29
ADH Abnormalities Hyposecretion Hypersecretion Diabetes insipidus
Increased urine output of dilute urine “high and dry” Na+ levels are increased; ICF dehydrated Hypersecretion Syndrome of inappropriate antidiuretic hormone (SIADH) Decreased urine output Fluid overload; low Na+ levels
 Decreased urine output. Fluid overload; low Na+ levels.")
30
Oxytocin (OT) Target cells: mammary glands & uterine smooth muscle
Operates on a positive feedback loop Stimulates uterine smooth muscle contractions During childbirth stretching of receptors causes continued release of oxytocin until after delivery of the placenta Ejection of milk into ducts of the breast of lactating women When breastfeeding the suckling action of the baby causes secretion of additional oxytocin increasing milk production Breastfeeding also helps the uterus continue to contract back to normal size during the postpartum period

31
Pineal Body Regulates the body’s biological clock Secretes melatonin
Patterns of eating Sleeping Female reproductive cycle Behavior Secretes melatonin Induces sleep Secretion is inhibited by sunlight Target cell in humans is unknown

32
Melatonin & Seasonal Affective Disorder
Also know as “winter depression” During shorter days, melatonin secretion increases causes a depressed feeling in affected patients Treatment Exposure to high-intensity lights to inhibit melatonin secretion

33
Thyroid Gland The thyroid gland is composed of two lateral lobes connected by an isthmus Located on the anterior and lateral surfaces of the trachea, below the larynx

34
Thyroid Hormones Tetraiodothyronine or thyroxine (T4)
Most abundant thyroid hormone Contains 4 iodine atoms May have effect on target cells, but mostly serve as precursor to T3 Triodothyronine (T3) “principal thyroid hormone” Contains 3 iodine atoms
 principal thyroid hormone Contains 3 iodine atoms.")
35
Thyroid Hormones Both hormone bind to plasma proteins once secreted into the bloodstream Function: Regulate metabolic rate of all cells Regulate cell growth Regulate tissue differentiation Target cells: “general” because thyroid hormones can potentially interact with all cells of the body

36
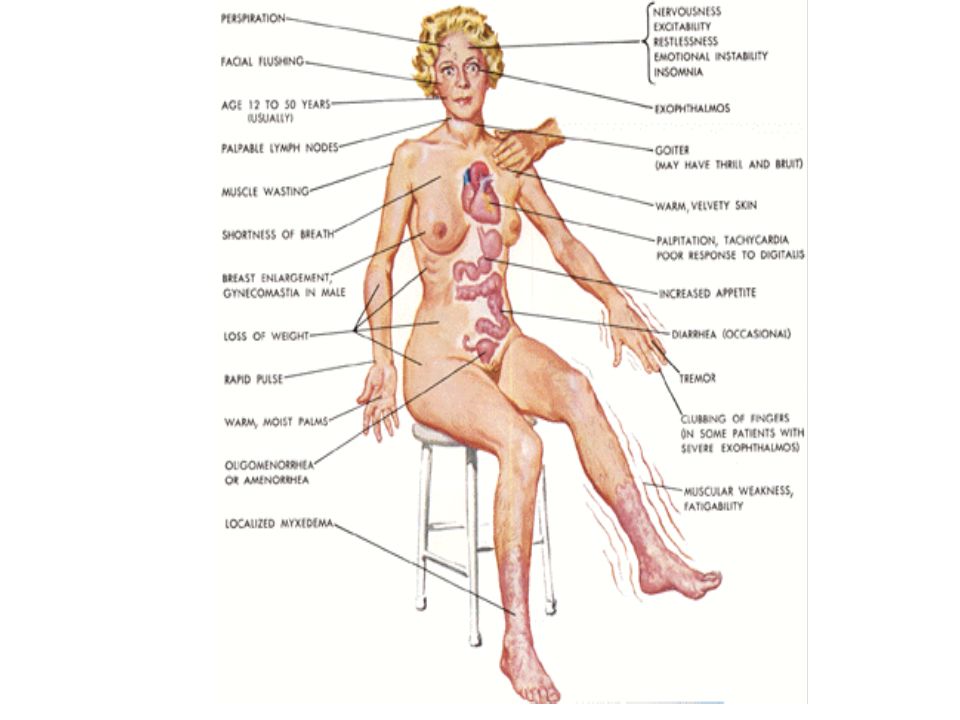
Hypersection Graves Disease
Autoimmune condition (thyroid stimulating antibodies causes abnormal secretion) Weight loss Increases basal metabolic rate Increased heart and respiratory rate exophthalmos
 Weight loss. Increases basal metabolic rate. Increased heart and respiratory rate. exophthalmos.")
38
Exophthalmos

39
Hyposecretion of Thyroid Hormone
Cretinism – develops during the growth years due to hypothyroidism Low metabolic rate Retarded growth and sexual development Mental retardation (possibly) Hypothyroidism later in life Decreased metabolic rate Loss of mental & physical vigor Weight gain Loss of hair Yellow discoloration of the skin myxedema
 Hypothyroidism later in life. Decreased metabolic rate. Loss of mental & physical vigor. Weight gain. Loss of hair. Yellow discoloration of the skin. myxedema.")
41
Goiter Caused by lack of iodine in the diet
Iodine is needed to synthesize thyroid hormone Lack of iodine causes drop in thyroid hormone production/secretion Negative feedback loop informs hypothalamus and anterior pituitary to release releasing hormones and TSH Lack of iodine causes enlargement of thyroid gland

43
Calcitonin The 3rd hormone secreted from the thyroid gland
Target cells – bone Function – regulates calcium levels in the blood by decreasing blood calcium levels Increases action of osteoblasts (build bone) and inhibits action of osteoclasts (breakdown bone) Antagonist to parathyroid hormone
 and inhibits action of osteoclasts (breakdown bone) Antagonist to parathyroid hormone.")
44
Parathyroid Glands Parathyroid glands are embedded in the posterior aspect of the thyroid glands Usually 4 or 5 parathyroid glands

45
Parathyroid Hormone Secreted from Parathyroid glands
Target cells: bone and kidney Action: maintains calcium homeostasis Increases osteoclast activity; decrease osteoblast activity Calcium absorbed in kidneys and returned to the bloodstream Activates vitamin D in the kidneys which increases intestinal absorption of calcium Parathyroid hormone is an antagonist to calcitonin

47
Adrenal Glands Located on top of both of the kidneys
Composed of two parts: Outer portion adrenal cortex Inner portion adrenal medulla Both parts of the adrenal glands are structurally and functionally different; often treated as two different glands

48
Adrenal Cortex Composed of three distinct layers or zones
Outer zone secrete mineralocorticoids Middle zone secrete glucocorticoids Inner zone secrete glucocorticoids and gonadocorticoids

50
Pancreas Located in the LUQ
Contains both endocrine and exocrine tissue Endocrine portion is made up of tiny islands of cells called pancreatic islets (also islets of Langerhans) Alpha cells secrete glucagon Beta cells secrete insulin
 Alpha cells secrete glucagon. Beta cells secrete insulin.")
52
Pancreatic Hormones Glucagon Insulin
Increases blood glucose levels Converts glycogen to glucose in liver cells Stimulates gluconeogenesis Target cells liver Insulin Decreases blood glucose levels Promotes movement of glucose, amino acids, fatty acids into cells Promotes metabolism of these molecules once by cells Target cells general (all cells) Glucagon and Insulin produce antagonistic effects (fig 16-27, page 512)
 Glucagon and Insulin produce antagonistic effects (fig 16-27, page 512)")
54
Diabetes Results from either
1) inadequate or absence of insulin production 2) Insulin resistance – decreased insulin receptors results in decreased effectiveness of glucose uptake
 inadequate or absence of insulin production. 2) Insulin resistance – decreased insulin receptors results in decreased effectiveness of glucose uptake.")
55
Diabetes – Signs & Symptoms
Hyperglycemia – elevated amounts of glucose in the blood Results glucose not entering the cells properly Glycosuria – glucose present in the urine Elevated glucose levels in the blood exceeds kidney’s abilities to reabsorb glucose; glucose “spills over” into the urine Polyuria – increased urine production Water follows glucose lost in urine

56
Diabetes – Signs & Symptoms
Polydipsia – excessive thirst Polyuria causes dehydration Polyphagia – excessive and continuous hunger Although blood sugar is high cells are “starving” because cells cannot uptake glucose **3 P’s = polyuria, polydipsia, polyphagia**

57
Type 1 Diabetes Absolute deficiency of insulin production
Cause of beta cell destruction is unknown Requires insulin injections or an insulin pump

58
Type 2 Diabetes Previously called non-insulin-dependent diabetes (NIDDM) or adult onset diabetes Beta cell produce reduced amounts of insulin Loss of insulin receptors on target cells leads to insulin resistance Treated with insulin injections, oral diabetic medication and lifestyle modifications

59
Complications of Diabetes
Untreated or poorly controlled diabetes can lead to many complications that affect almost every system in the body: Atherosclerosis – build up of fatty materials in the blood vessls Lead to heart attack, stroke, reduced circulation Diabetic retinopathy – can lead to blindless

60
Complications of Diabetes
Neuropathy – nerve damage Amputations Kidney disease May require dialysis

61
Gonads – Testes & Ovaries
Composed mainly of coils of seminiferous tubules & interstitial cells Interstitial cells secrete testosterone Target cells – general Function: Growth & maintenance of male sexual characteristics Sperm production Testosterone secretion is regulated by the gonadotropin leutinizing hormone (LH)
")
62
Gonads – Testes & Ovaries
Estrogen Secreted by cells of the ovarian follicles Target cells: general Functions: Promote development & maintenance of female sexual characteristics Breast development Regulation of menstrual cycle

63
Gonads – Testes & Ovaries
Progesterone (“pregnancy-promoting hormone”) Secreted by corpus luteum Target cells: general Functions (with estrogen): Maintains the lining of the uterus to maintain a pregnancy Remember Estrogen & Progresterone secretion is regulated by FSH and LH (gonadotropic hormones)
 Secreted by corpus luteum. Target cells: general. Functions (with estrogen): Maintains the lining of the uterus to maintain a pregnancy. Remember Estrogen & Progresterone secretion is regulated by FSH and LH (gonadotropic hormones)")
64
Placenta Tissue that forms along the lining of the uterus
Serves as the connection between the circulatory systems of the mother and developing fetus Secretes human chorionic gonadotropin (hCG) Target cells: ovaries
 Target cells: ovaries.")
65
Placenta Function: hCG is high during the 1st trimester
Stimulates hormone (estrogen & progesterone) secretion from the ovaries High levels of estrogen & progesterone help maintain uterine lining for pregnancy hCG is high during the 1st trimester A high hCG level is used to confirm a pregnancy
 secretion from the ovaries. High levels of estrogen & progesterone help maintain uterine lining for pregnancy. hCG is high during the 1st trimester. A high hCG level is used to confirm a pregnancy.")
Similar presentations














>")








 Tropic hormones.>")


