Download presentation
Presentation is loading. Please wait.

1
SHOCK Dr.Mohammed Sharique Ahmed Quadri Assistant Prof.Physiology
Almaarefa College

2
Inadequate Tissue Perfusion
WHAT IS SHOCK? Shock is the term used to describe acute circulatory failure with inadequate or inappropriately distributed tissue perfusion resulting in generalized cellular hypoxia and/or an inability of the cells to utilize oxygen. Inadequate Tissue Perfusion SHOCK IS A SYNDROME THAT CAN OCCUR IN THE COURSE OF MANY LIFE THREATENING TRAUMATIC CONDITIONS OR DISEASE STATES

3
Or it can be define simply as
A clinical state in which tissues do not receive adequate blood flow and O2 to meet their metabolic needs. Firstly, we are going to recap some basic physiological principles and apply them to a patient with shock. SBP, SVR and CO are intrinsically linked to blood flow.

4
Physiological Principles
Tissue perfusion is driven by blood pressure BP = CO X PVR CO – Cardiac Output PVR – Peripheral Vascular resistance

5
CO = SV X HR This means that BP= SV X HR X PVR
Cardiac Output CO = SV X HR This means that BP= SV X HR X PVR Blood Pressure = Stroke Volume X Heart Rate X Peripheral Vascular Resistance

6
What affects Stroke volume?
Volume of Blood pumped by the heart during 1 cycle What affects Stroke volume? Rhythm Problems Blood Volume Stroke Volume Heart Muscle Damage MechanicalObstruction Mechanical Obstruction

7
What makes up blood volume
Plasma RBCs WBCs Platelets

8
What Alters Blood Volume?
Haemorrhage Plasma Loss Loss /Redistribution of Extracellular Volume

9
Heart rate too fast to allow adequate refilling of heart between beats
Heart rate increases as a compensatory response to Shock Heart rate too fast to allow adequate refilling of heart between beats

10
Peripheral Vascular Resistance
PVR regulated by ARTERIOLAR tone. Dilatation opens Arteriovenous beds & increases volume of circulatory system

11
What Alters PVR? Circulating cytokines & Inflammatory mediators (e.g. Histamine) Endotoxins Drugs (e.g. Nitrates)
 Endotoxins. Drugs (e.g. Nitrates) .")
12
Mechanical Obstruction
Blood Volume Mechanical Obstruction Heart Damage / Rhythm Stroke Volume Heart Rate PVR Blood Pressure

13
TYPES OF SHOCK HYPOVOLEMIC CARDIOGENIC OBSTRUCTIVE DISTRIBUTIVE

14
DISTRIBUTIVE SHOCK

15
Hypovolaemic Volume Loss Blood loss -Haemorrhage Plasma Loss -Burns
ECF Loss - Vomiting & Diarrhoea

16
Cardiogenic Pump Failure May be due to
Inability of heart to Contract or Inability of heart to pump blood Myocardial damage ( M.I) Arrhythmias Valvular damage
 Arrhythmias. Valvular damage.")
17
Distributive Decreased Peripheral Vascular Resistance
Septic Shock (inflammatory mediators) Neurogenic Shock (loss of sympathetic control on vascular tone) ANAPHYLACTIC shock (presence of vasodilator substances like histamine)
 Neurogenic Shock (loss of sympathetic control on vascular tone) ANAPHYLACTIC shock (presence of vasodilator substances like histamine)")
18
PATHOPHYSIOLOGY OF SHOCK
The manifestation of shock reflects both The impaired perfusion of body tissue & The body’s attempt to maintain tissue perfusion (compensatory mechanism)
")
19
COMPENSATORY MECHANISMS

20
Compensatory mechanism and shock
PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac Output (SV x HR) Vascular Diameter (SVR)
 Cardiac. Output. (SV x HR) Vascular. Diameter. (SVR)")
21
Hypovolaemic shock PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac
Output (SV x HR) Vascular Diameter (SVR) 1
 Vascular. Diameter. (SVR) 1.")
22
Hypovolaemic shock PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac
Output (SV x HR) Vascular Diameter (SVR) 1 2
 Vascular. Diameter. (SVR)")
23
Hypovolaemic shock PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac
Output (SV x HR) Vascular Diameter (SVR) 1 2 3
 Vascular. Diameter. (SVR)")
24
Cardiogenic shock PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac
Output (SV x HR) Vascular Diameter (SVR) 1
 Vascular. Diameter. (SVR) 1.")
25
Cardiogenic shock PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac
Output (SV x HR) Vascular Diameter (SVR) 1 2
 Vascular. Diameter. (SVR)")
26
Cardiogenic shock PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac
Output (SV x HR) Vascular Diameter (SVR) 3 1 2
 Vascular. Diameter. (SVR)")
27
Distributive shock PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac
Output (SV x HR) Vascular Diameter (SVR) 1
 Vascular. Diameter. (SVR) 1.")
28
Distributive shock PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac
Output (SV x HR) Vascular Diameter (SVR) 2 1
 Vascular. Diameter. (SVR)")
29
Distributive shock PRE-LOAD AFTER-LOAD Fluid Volume (CVP/JVP) Cardiac
Output (SV x HR) Vascular Diameter (SVR) 2 3 1
 Vascular. Diameter. (SVR)")
30
Sympatho-Adrenal Response to Shock
Most immediate of compensatory mechanisms are those of sympathetic nervous system and renin angiotensin mechanism Sympathetic nervous system NE, epinephrine, and cortisol release Causes vasoconstriction, increase in HR, and increase of cardiac contractility (cardiac output) Renin-angiotensin axis Water and sodium conservation and vasoconstriction Increase in blood volume and blood pressure
 Renin-angiotensin axis. Water and sodium conservation and vasoconstriction. Increase in blood volume and blood pressure.")
31
Sympatho-Adrenal Response to Shock

33
Compensatory reactions activated by hemorrhage.
Vasoconstriction Tachycardia Venoconstriction Tachypnea→increased thoracic pumping Restlessness→increased skeletal muscle pumping (in some cases) Increased movement of interstitial fluid into capillaries Increased secretion of norepinephrine and epinephrine Increased secretion of vasopressin Increased secretion of renin and aldosterone Increased secretion of erythropoietin Increased plasma protein synthesis Restlessness and agitation is common in early shock , it is because of increase sympathetic stimulation and epinephrine release .as shock progresses blood supply to brain is decreased and restlessness is replaced by altered mentation and uncontiousness.
 Increased movement of interstitial fluid into capillaries. Increased secretion of norepinephrine and epinephrine. Increased secretion of vasopressin. Increased secretion of renin and aldosterone. Increased secretion of erythropoietin. Increased plasma protein synthesis. Restlessness and agitation is common in early shock , it is because of increase sympathetic stimulation and epinephrine release .as shock progresses blood supply to brain is decreased and restlessness is replaced by altered mentation and uncontiousness.")
34
Effect of hemorrhage on mean arterial pressure

35
Sympathetic activation
Tachycardia Increased myocardial contractility (β1) α-adrenergic receptor-mediated vasoconstriction (β2-receptor-mediated vasodilatation in skeletal muscle, bronchodialatation ) Overall increased COP and redistribution of flow: cardiac, cerebral, hepatic and muscle vascular beds There are other effects mediated by the SNS, but these are the important factors when considering shock.
 α-adrenergic receptor-mediated vasoconstriction (β2-receptor-mediated vasodilatation in skeletal muscle, bronchodialatation ) Overall increased COP and redistribution of flow: cardiac, cerebral, hepatic and muscle vascular beds. There are other effects mediated by the SNS, but these are the important factors when considering shock.")
36
Points to Ponder Goal is to maintain cerebral and cardiac perfusion
Vasoconstriction of splanchnic, and renal blood flow Compensatory mechanisms are not effective over the long term and fails when shock state is prolonged.

37
Neuroendocrine response
Release of pituitary hormones such as adrenocorticotrophic hormone (ACTH), vasopressin(antidiuretic hormone, ADH). There is release of cortisol, which causes fluid retention and antagonizes insulin. There is release of glucagon, which raises the blood sugar level. Absolute adrenocortical insufficiency due to bilateral adrenal hemorrhage or necrosis is rare(in septic shock) and that this may be associated with an impaired pressor response to norepinephrine(noradrenaline) and a worsen the prognosis. cause of this phenomenon remain unclear.
, vasopressin(antidiuretic hormone, ADH). There is release of cortisol, which causes fluid retention and antagonizes insulin. There is release of glucagon, which raises the blood sugar level. Absolute adrenocortical insufficiency due to bilateral adrenal hemorrhage or necrosis is rare(in septic shock) and that this may be associated with an impaired pressor response to norepinephrine(noradrenaline) and a worsen the prognosis. cause of this phenomenon remain unclear.")
38
Pathophysiology of shock cellular responses
Inadequate tissue perfusion Decreased oxygen supply Anaerobic metabolism Accumulation metabolic waste & lactate Cellular failure (limited ATP produce) Inadequate tissue perfusion due to inadequate blood supply.
 Inadequate tissue perfusion due to inadequate blood supply.")
39
Understanding Shock Cellular responses to decreased systemic oxygen delivery ATP depletion → Na+/ K+ pump dysfunction Cellular edema – Due to accumulation of Na+ inside the cell Hydrolysis of cellular membranes and cellular death Mitochondrial activity severely depressed and lysosomal rupture may occur systemic metabolic lactic acidosis that overcomes the body’s compensatory mechanisms

40
Release of Pro- and Anti Inflammatory Mediators
Trigger an exaggerated inflammatory response (systemic activation of leucocytes & release of potentially damaging ‘mediators’) Severe infection (bacteraemia/endotoxaemia), Presence of large areas of damaged tissue (following trauma /extensive surgery) Prolonged episodes of hypoperfusion
 Severe infection. (bacteraemia/endotoxaemia), Presence of large areas of. damaged tissue. (following trauma /extensive surgery) Prolonged episodes of hypoperfusion.")
41
Release of Pro- and Anti Inflammatory Mediators (continued)
Pro inflammatory Mediators: Proteases Toxic free radicals & other reactive oxygen species Cytokines IL TNF Platelet activating factor Hypotension, Inc. vascular permeability, platelet aggregation. Anti inflammatory mediators: Interleukin 10 ( IL-10) Are involved in leukocyte adhesion ,local inflammation, neutrophil activation, fever, lactic acidosis, ventilation perfusion abnormalities
 Are involved in leukocyte adhesion ,local inflammation, neutrophil activation, fever, lactic acidosis, ventilation perfusion abnormalities.")
42
Release of Pro- and Anti Inflammatory Mediators (continued)
Although beneficial when targeted against local areas of infection or necrotic tissue--dissemination of this ‘innate immune’ response can produce shock and widespread tissue damage. Characteristically the initial episode of overwhelming inflammation is followed by a period of immune suppression--- increased risk of developing secondary infections.

43
Harmful effects of inflammatory mediators
Damage to cell membranes Impaired mitochondrial respiration DNA strand breakage Apoptosis, which may contribute to the organ damage Vasodilatation Maldistribution of regional blood flow Abnormalities in the microcirculation: – capillaries are obstructed – increased capillary permeability with interstitial oedema. and immune hypo-responsiveness associated with sepsis. Coagulation disorders

44
VICIOUS CYCLE Hypoperfusion
Cellular injury Inflammatory mediators Functional & structural changes in microvascular circulation

45
Global Tissue Hypoxia Endothelial inflammation and disruption
Inability of O2 delivery to meet demand Result: Lactic acidosis Cardiovascular insufficiency Increased metabolic demands

46
BREAK !

47
CLINICAL FEATURES OF SHOCK

48
Symptoms of Shock Hx of Trauma / other illness Vomiting & Diarrhoea
General Symptoms Specific Symptoms Anxiety /Nervousness Dizziness Weakness Faintness Nausea & Vomiting Thirst Confusion Decreased UO Hx of Trauma / other illness Vomiting & Diarrhoea Chest Pain Fevers / Rigors SOB

49
Signs of Shock Pale Cold & Clammy skin Sweating Cyanosis Tachycardia
Tachypnoea Confused / Aggiatated Unconscious Hypotensive Stridor / SOB

50
Hypovolaemic Shock

51
Clinical Feature of Hypovolaemic shock
Inadequate tissue perfusion: Skin – Cold, Pale, Slate-grey, ‘Clammy’, Slow capillary refill, Kidneys – Oliguria, Anuria (c) Brain – Drowsiness, Confusion and Irritability.
 Brain – Drowsiness, Confusion and Irritability.")
52
Clinical Feature of Hypovolaemic shock
Increased sympathetic tone: Tachycardia, narrowed pulse pressure, ‘weak’ or ‘thready’ pulse (b) Sweating (c) Blood pressure – may be maintained initially (despite up to a 25% reduction in circulating volume if the patient is young and fit),but later hypotension supervenes.
 Sweating. (c) Blood pressure – may be maintained initially (despite up to a 25% reduction in circulating volume if the patient is young and fit),but later hypotension supervenes.")
53
Clinical Feature of Hypovolaemic shock
Metabolic acidosis – compensatory tachypnoea. Extreme hypovolaemia may be associated with bradycardia.

54
Cardiogenic Shock

56
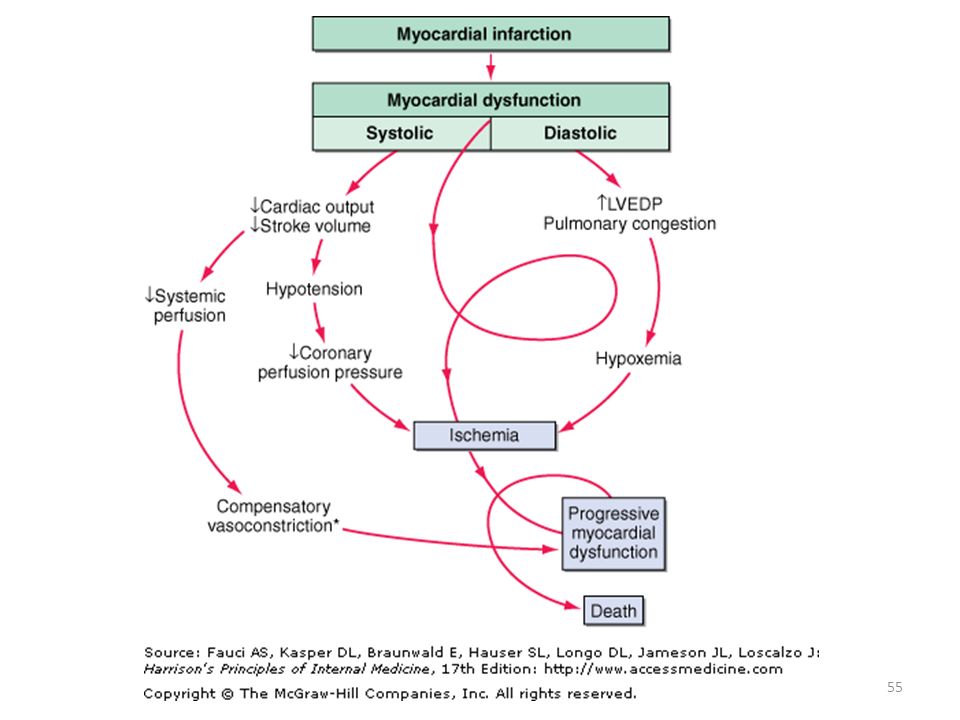
Clinical Feature of Cardiogenic Shock
Sign & symptoms are consistent with those of heart failure Stagnation of blood flow & increase extraction of O2 from hemoglobin: Lips, nail beds and skin become cyanotic Poor stroke volume : Decrease in MAP & SBP Near normal diastolic B.P due to vasoconstriction Narrow pulse pressure

57
Clinical Feature of Cardiogenic Shock
Low renal perfusion pressure & aldosterone release: Decrease urine output Elevated preload : Rise in CVP and pulmonary capillary wedge pressure Poor cerebral perfusion: Alteration in cognition and consciousness

58
Clinical Feature of Cardiogenic Shock
Acute pulmonary oedema: Tachypnoea, orthopnea, pulmonary crackles, oxygen saturation < 90% on air, pulmonary oedema on CXR

59
Obstructive Shock

60
Clinical Feature of Obstructive Shock
Elevated JVP and CVP Pulsus paradoxus and muffled heart sounds in cardiac ,tamponade. Signs of pulmonary embolism Pulmonary oligaemia on X-ray Dyspnoea On ECG – P-Pulmonale, RAD Systolic blood pressure normally falls during quiet inspiration in normal individuals. Pulsus paradoxus is defined as a fall of systolic blood pressure of >10 mmHg during the inspiratory phaseNormally during inspiration, systolic blood pressure decreases ≤10 mmHg.,[1] and pulse rate goes up slightly. This is because inspiration makes intrathoracic pressure more negative relative to atmospheric pressure. The negative pressure in the thorax increases venous return, so more blood flows into the right side of the heart. However, the decrease in intrathoracic pressure also expands the compliant pulmonary vasculature. This increase in pulmonary blood capacity pools the blood in the lungs, and decreases pulmonary venous return, so flow is reduced to the left side of the heart. Also the increased systemic venous return to the right side of the heart expands the right heart and directly compromises filling of the left side of the heart. Reduced left-heart filling leads to a reduced stroke volume which manifests as a decrease in systolic blood pressure. The decrease in systolic blood pressure leads to a faster heart rate due to the baroreceptor reflex, which stimulates sympathetic outflow to the heart.

61
Distributive Shock

62
Causes of Distributive Shock
Decreased sympathetic activity: neurogenic Brain or spine injury; anesthetics; emotion Vasodilator substances in blood Type I hypersensitivity (anaphylactic shock) Inflammatory response to infection (sepsis) Vessel damage from severe hypervolemia
 Inflammatory response to infection (sepsis) Vessel damage from severe hypervolemia.")
63
Neurogenic Shock Occurs after acute spinal cord injury or
defect in vasomotor center in brainstem or sympathetic outflow to blood vessels Brain injury Depressant action of drugs General anesthesia (barbiturate) Hypoxia/hypoglycemia Sympathetic outflow is disrupted leaving unopposed vagal tone Results in hypotension and bradycardia Skin is dry and warm
 Hypoxia/hypoglycemia. Sympathetic outflow is disrupted leaving unopposed vagal tone. Results in hypotension and bradycardia. Skin is dry and warm.")
64
Anaphylaxis Systemic response to the inflammatory mediators released in type I hypersensitivity Histamine, acetylcholine, kinins, leukotrienes, and prostaglandins all cause vasodilation What will happen when arterioles vasodilate throughout the body? Acetylcholine, kinins, leukotrienes, and prostaglandins all can cause bronchoconstriction What will happen when the bronchioles constrict?

65
Clinical Feature of Anaphylactic shock
Signs of profound vasodilatation: (a) Warm peripheries (b) Low blood pressure (c) Tachycardia. Erythema, urticaria, angio-oedema, pallor, cyanosis. Bronchospasm, rhinitis. Oedema of the face, pharynx and larynx. Pulmonary oedema. Hypovolaemia due to capillary leak. Nausea, vomiting, abdominal cramps, diarrhea.
 Warm peripheries. (b) Low blood pressure. (c) Tachycardia. Erythema, urticaria, angio-oedema, pallor, cyanosis. Bronchospasm, rhinitis. Oedema of the face, pharynx and larynx. Pulmonary oedema. Hypovolaemia due to capillary leak. Nausea, vomiting, abdominal cramps, diarrhea.")
66
Angio-oedema

67
Septic Shock

68
Sepsis or Systemic Inflammatory Response Syndrome (SIRS)
Inflammatory mediators released into the circulation Tumor necrosis factor Interleukins Prostaglandins Cause systemic signs of inflammation Fever and increased respiration, respiratory alkalosis, vasodilation, warm flushed skin Activate inflammatory pathways Coagulation, complement

69
Sepsis and Systemic Inflammatory Response
Infection: Invasion of normally sterile host tissue by microorganisms Bacteremia: Viable bacteria in blood Systemic inflammatory response syndrome (SIRS):The systemic inflammatory response to a variety of severe clinical insults. The response is manifested by two or more of the following: ■ Temperature > 38°C or < 36°C ■ Heart rate > 90 beats/min ■ Respiratory rate > 20 breaths/min or Paco2 < 4.3 kPa ■ White cell count > 12 × 109/L, < 4 × 109/L or > 10% immature forms Sepsis: SIRS resulting from documented infection Partial pressure of oxygen (PaO2) mmHg Partial pressure of carbon dioxide (PaCO2) mmHg Arterial blood pH of Oxygen saturation (SaO2) % Bicarbonate - (HCO3) mEq/L
:The systemic inflammatory response to a variety of severe clinical insults. The response is manifested by two or more of the following: ■ Temperature > 38°C or < 36°C. ■ Heart rate > 90 beats/min. ■ Respiratory rate > 20 breaths/min or Paco2 < 4.3 kPa. ■ White cell count > 12 × 109/L, < 4 × 109/L or > 10% immature forms. Sepsis: SIRS resulting from documented infection. Partial pressure of oxygen (PaO2) mmHg. Partial pressure of carbon dioxide (PaCO2) mmHg. Arterial blood pH of Oxygen saturation (SaO2) % Bicarbonate - (HCO3) mEq/L.")
70
Sepsis

71
Severe sepsis :Sepsis associated with organ dysfunction, hypoperfusion or hypotension. Hypoperfusion and perfusion abnormalities may include, but are not limited to, lactic acidosis, oliguria or an acute alteration in mental state, thrombocytopenia Septic shock: Severe sepsis with hypotension (systolic BP < 90 mmHg or a reduction of > 40 mmHg from baseline) in the absence of other causes for hypotension and despite adequate fluid resuscitation
 in the absence of other causes for hypotension and despite adequate fluid resuscitation.")
72
Sepsis or Systemic Inflammatory Response Syndrome (SIRS) (cont.)
Discussion: Why is septic shock called distributive? In the later phases of septic shock, blood volume decreases. What part of the inflammatory process explains this?

73
Septic Shock vasodilation decreased peripheral resistance decreased
blood pressure SEPTIC SHOCK 40% mortality

74
Septic Shock Also called systemic inflammatory response syndrome (SIRS) Inflammatory mediators also increase the metabolic rate of tissues, so they need more oxygen

75
Pattern of systemic inflammatory response
CARS: compensatory anti-inflammatory response syndrome; SIRS: systemic inflammatory response syndrome.

76
Clinical Feature of Septic shock
■ Pyrexia and rigors, or hypothermia (unusual). ■ Nausea, vomiting. ■ Vasodilatation, warm peripheries. ■ Bounding pulse. ■ Rapid capillary refill. ■ Hypotension (septic shock). ■ Other signs: (a) Jaundice (b) Coma, stupor (c) Bleeding due to coagulopathy (e.g. from vascular puncture sites, GI tract and surgical wounds) (d) Rash and meningism
. ■ Nausea, vomiting. ■ Vasodilatation, warm peripheries. ■ Bounding pulse. ■ Rapid capillary refill. ■ Hypotension (septic shock). ■ Other signs: (a) Jaundice. (b) Coma, stupor. (c) Bleeding due to coagulopathy (e.g. from vascular puncture sites, GI tract and surgical wounds) (d) Rash and meningism.")
77
Shock Types & Physiology
CVP/PCWP CO PVR Hypovolumic Septic Cardiogenic Neurogenic Cardiac temponade Anaphylactic

78
Shock Types & Physiology
CVP/PCWP CO PVR Hypovolemic ↓ ↑ Septic Cardiogenic Neurogenic Cardiac temponade Anaphylactic

79
Shock Types & Physiology
CVP/PCWP CO PVR Hypovolemic ↓ ↑ Septic Cardiogenic Neurogenic Cardiac temponade Anaphylactic

80
Shock Types & Physiology
CVP/PCWP CO PVR Hypovolemic ↓ ↑ Septic Cardiogenic Neurogenic Cardiac temponade Anaphylactic

81
Shock Types & Physiology
CVP/PCWP CO PVR Hypovolemic ↓ ↑ Septic Cardiogenic Neurogenic Cardiac temponade Anaphylactic

82
Shock Types & Physiology
CVP/PCWP CO PVR Hypovolemic ↓ ↑ Septic Cardiogenic Neurogenic Cardiac temponade Anaphylactic

83
Shock Types & Physiology
CVP/PCWP CO PVR Hypovolemic ↓ ↑ Septic Cardiogenic Neurogenic Cardiac temponade Anaphylactic

84
Any questions?

85
Refrences Essentials of pathophysiology by carol Mattson Porth, 3rd edition. Kumar & Clark's Clinical Medicine, 7th Edition

Similar presentations





 ~5% of total.>")












 leading to inadequate oxygen delivery to tissues.>")

 system is an important endocrine component of autoregulation. Renin is released by kidneys when.>")