Download presentation
Presentation is loading. Please wait.

1
CHRONIC COUGH 2014 Mandel Sher, MD Clinical Professor of Medicine and Pediatrics Division of Allergy and Immunology Morsani College of Medicine University of South Florida

2
www.centerforcough.comwww.centerforcough.com
3
Cough Defense mechanism to clear secretions and foreign materials from airways Convert dysrhythmias and maintain consciousness during severe dysrhythmias Factor in spread of infection Common symptom prompting medical attention

4
Cough Acute cough- less than three weeks – Common cold Subacute cough- three to eight weeks – Post infectious cough Chronic cough- greater than eight weeks

5
Acute Cough Common cold Viral bronchitis Non- viral infection – Pertussis, Chlamydia, mycoplasma Environmental irritant Foreign body aspiration Pneumonia CHF

6
Postinfectious Cough Diagnosis of exclusion Prolonged cough after URI with normal chest radiograph Resolves over time e.g. multiple months Oral steroids, inhaled steroids, ipratropium bromide therapies ?role of leukotriene inhibitors Braman, SS Chest 2006;129(suppl),138S-146S
,138S-146S.")
8
Chronic Cough Case 61 y/o non smoking female with ten years of continuous cough with onset after URI. Dry cough prompted by throat tickle and triggered by talking, scents/odors, and by changes in temperatures. Cough can induce incontinence. Feels socially isolated, anxious, and can be depressed. Family members and co-workers have expressed annoyance. Finds throat lozenges and sipping on water helpful. Evaluated by primary care MD, two ENT’s, GI, Pulmonary and Allergy. Unresponsive to multiple therapies.

9
The Key to Chronic Cough Anatomic Approach In the non smoker, without ACE inhibitors, and a normal chest x-ray GERD – NERD POST NASAL DRIP(Upper Airway Cough Syndrome)- allergic rhinitis, vasomotor rhinitis, sinusitis COUGH VARIANT ASTHMA – Non Asthmatic Eosinophilic Bronchitis Idiopathic cough Irwin etal. Diagnosis and Management of Cough AACP Evidence basedClinical Practice Guidelines.Chest.2006; S1-S237.

10
It’s the Cough Reflex, Stupid! Chronic cough is the result of cough reflex hypersensitivity with triggers from associated anatomic entities

11
Anatomy of Cough Afferent stimulus, central processing and control, and efferent output – Complex and not well understood Cough is involuntary to protect from inhaled, aspirated and intrapulmonary Cough can be voluntary The “Urge to Cough” irritant type cough Canning, B. J. Chest 2006;129:33S-47S

12
Anatomy Of Cough Mechanosensory cough – “true cough receptor” – Protect against aspiration of objects and acid – Conscious and anesthetized in Guinea pigs not human – Involves vagal/Alpha delta myelinated pathways – RAR and SAR receptors Brooks. Cough. 2011, 7:10 Mazzone.Cough.1;2doi:10.1186/1745-9974-1-

13
Anatomy of Cough Chemicosensory cough – Chemical, irritants and lung inflammation – Conscious but not anesthetized – Nociceptive Type C unmyelinated fibers – TRPV1 and TRPA1 receptors Also in pain and itch pathways Capsaicin- irritant bradykinin & tachykinin(inflammation) Brooks. Cough. 2011, 7:10 Mazzone.Cough.1;2doi:10.1186/1745-9974-1-

14
Anatomy of Cough Poorly defined, diffuse “cough center” in medulla separate from breathing center Possible state of “excitability’ from different afferent pathways – Esophageal, upper and lower respiratory Heightened responses to innocuous stimuli eg perfume or cold air, laughing or talking Anti-tussive effects of opiates, N-methyl-D- aspartate and possibly anti-histamines Canning, B. J. Chest 2006;129:33S-47S

15
Cough reflex after URI McGarvey etal: oi:10.1016/j.pupt.2008.11.003 oi:10.1016/j.pupt.2008.11.003 d

16
Capsaicin Cough Challenge Women have increased sensitivity Smokers have decreased sensitivity URI has transient increase sensitivity Allergic rhinitis> normals Stable asthmatics=normals Cough asthma> non cough asthma Acid in distal esophagus increases sensitivity Dicpingaitis:Pulmonary Pharmacology & Therapeutics Volume 20, Issue 4Volume 20, Issue 4, August 2007, Pages 319-324

17
Confessions of a Cough Doctor Chronic coughers have heightened Cough Reflex Sensitivity(CRS) CRS has variable inflammatory, neurogenic and behavioral components UACS, GERD, and asthma associated with chronic cough – Direct activation of cough – By increasing CRS – Innocent bystander Diagnostics studies-specificity/sensitivity?
 CRS has variable inflammatory, neurogenic and behavioral components UACS, GERD, and asthma associated with chronic cough – Direct activation of cough – By increasing CRS – Innocent bystander Diagnostics studies-specificity/sensitivity")
18
Upper Airway Cough Syndrome A major contributor to chronic cough – Allergic rhinitis, vasomotor rhinitis, sinusitis Mechanisms – Nasal inflammation from allergy and infection causes CRS – Vasomotor neuropathy causes CRS – Post nasal drip- causative or associated only? Symptoms can be “silent” in 20%(based on response to therapy with first generation antihistamines) A sensation of post nasal drip, nasal discharge, or throat clearing First generation antihistamines more effective than new non sedating antihistamines. Act as antitussive via anticholinergic or TRPV1 receptors
 A sensation of post nasal drip, nasal discharge, or throat clearing First generation antihistamines more effective than new non sedating antihistamines. Act as antitussive via anticholinergic or TRPV1 receptors.")
19
Rhinitis Treatment Nasal steroids – Allergic rhinitis(AR) and non allergic rhinitis(NAR *Intranasal anti-histamines – Both for AR and NAR(helps congestion) – May be additive to nasal steroids Anti-histamines – AR only *Classical anti-histamines in chronic cough *Ipratropium bromide – NAR(rhinorrhea) Nasal saline
 and non allergic rhinitis(NAR *Intranasal anti-histamines – Both for AR and NAR(helps congestion) – May be additive to nasal steroids Anti-histamines – AR only *Classical anti-histamines in chronic cough *Ipratropium bromide – NAR(rhinorrhea) Nasal saline")
21
Laryngopharyngeal Reflux Vocal Cord Hyperfunction

22
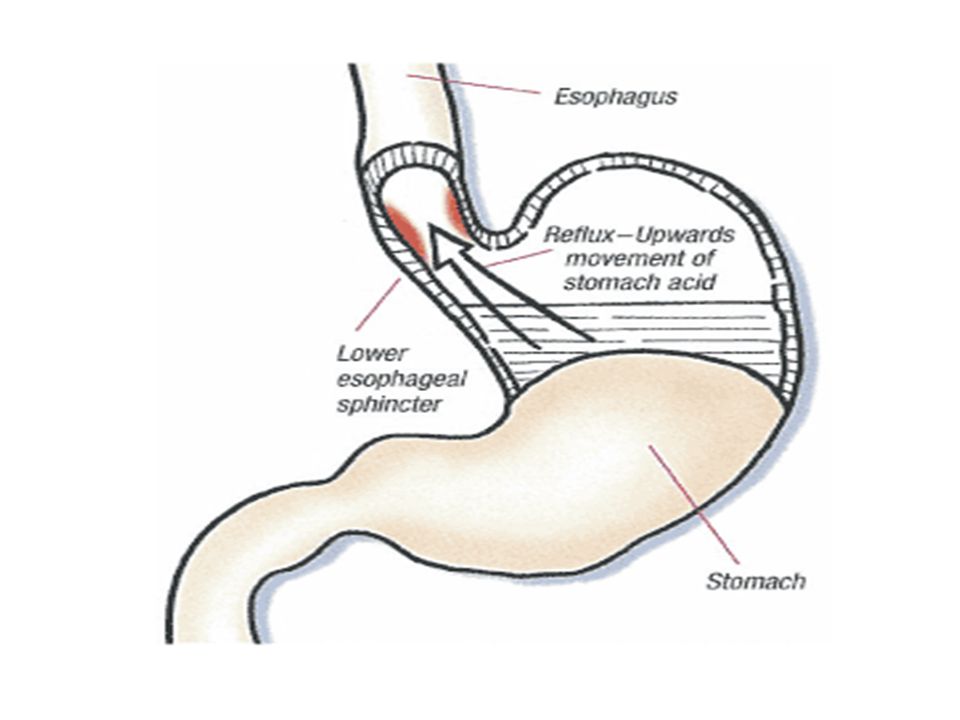
GERD and Chronic Cough Proximal vs Distal GERD/NERD as trigger/cause of cough? – Hoarseness, throat clear, and sore throat imply LPR – Microaspiration probably not common Possibly in elderly? – GERD symptoms – Asymptomatic Mechansims – Direct acid, pepsin, gas – Esophageal activation of cough reflex – Associative but not causative Woodcock etal. British Medical Bulletin 2010;96:61-73

23
GERD and Chronic Cough Cough triggers GERD/NERD – Most chronic coughers probably have GERD/NERD Esophageal dysmotility – Possible rational of response to macrolide antibioticcs Diagnostics have poor specificity/ sensitivity – EGD to identify Barrett’s, strictures, eosinophilic esophagitis – pH probe, manometry and multichannel intraluminal impedance

24
GERD and Chronic Cough Diagnosis and Treatment Coughing decreasing with PPI and/or dietary therapy Response to PPI therapy may takes months Not all PPI’s are alike and benefit from twice daily dosing PPI therapy should not be indefinite due to potential side effects Dietary therapy

26
Cough Variant Asthma and Chronic Cough Clinical characteristics – With or without wheezing, SOB, chest findings – Generally increases with exercise, laughter, cold exposure and middle night(all non specific) – PFT’s generally normal – Allergy/atopy in 40-80% – Bronchial hyperreactivity is hallmark Non Asthma Eosinophilic Bronchitis – Absence of variable airway obstruction and bronchial hyperreactivity – Sputum eosinophils with mast cells in airway epithelium rather than smooth muscle – Both respond inhaled and oral corticosteroids
 – PFT’s generally normal – Allergy/atopy in 40-80% – Bronchial hyperreactivity is hallmark Non Asthma Eosinophilic Bronchitis – Absence of variable airway obstruction and bronchial hyperreactivity – Sputum eosinophils with mast cells in airway epithelium rather than smooth muscle – Both respond inhaled and oral corticosteroids")
27
Diagnosis of “Chest Cough” Expired nitric oxide(eNO) predicted positive response to ICS in chronic cough with a cut off of 38ppm 36/41 positive response to ICS high eNO 2/24 positive response to ICS – low eNO Methacholine challenge less sensitive/spec. Cough asthma and eosinophilic bronchitis Hahn PY - Mayo Clin Proc - 01-NOV-2007; 82(11): 1350-5
:")
28
Cough Variant Asthma and Chronic Cough Response to therapy can be diagnostic Traditional asthma treatment – ICS +/- LABA – May take 6-8 weeks for maximal response – Inhalers may be irritating – Use MDI with spacers – Value of oral corticosteroid trial

30
Chronic Cough Cough Reflex Treatment Oral corticosteroids – Peripheral and ??central Opiates-central – NDMA-dextromethorphan Classical antihistamines – Oral-central and peripheral e.g. chlorpheniramine – Intranasal-peripheral Benzonatate, menthol drops-peripheral Amitryptylline, gabapentin, pregabalin Speech therapy

31
Refractory Chronic Cough BREAK THE COUGH CYCLE Concurrent Therapy – GERD- Diet +/- PPI – UACS- INS, INA, chlorpheniramine – Asthma/eosinophilic bronchitis if indicated MDI ICS with spacer – Cough suppression Pharmacologic- opiate, antihistamines, benzonatate exercises – Cough inflammation Oral corticosteroids – Cough neuropathy Gabapentin, amitriptylline

Similar presentations













 BONUS.>")








 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")