Download presentation
Presentation is loading. Please wait.

1
Disorders of Red Blood Cells
Professor Myat Thandar Department of Physiology University of Medicine 1

2
Functions of RBCs O2 transport (Hb in the RBCs) CO2 transport
Acid-base balance

3
Functional Importance of the Biconcave Shape of RBCs
Larger surface area for O2 diffusion Thinness of cell membrane enables O2 to diffuse easily Flexibility of membrane facilitates the transport function

4
Network of Fibrous Proteins of RBCs
Spectrin and Ankyrin Imparts elasticity and stability to membrane and allows RBCs to deform easily

5
Haemoglobin A natural pigment, reddish when oxygenated
4 polypeptide chains (a globin portion and a heme unit)
")
6
Haemoglobin F in Fetus Higher affinity for O2 than adult Hb
HbF is replaced within 6 months of birth with HbA

7
Haemoglobin Synthesis
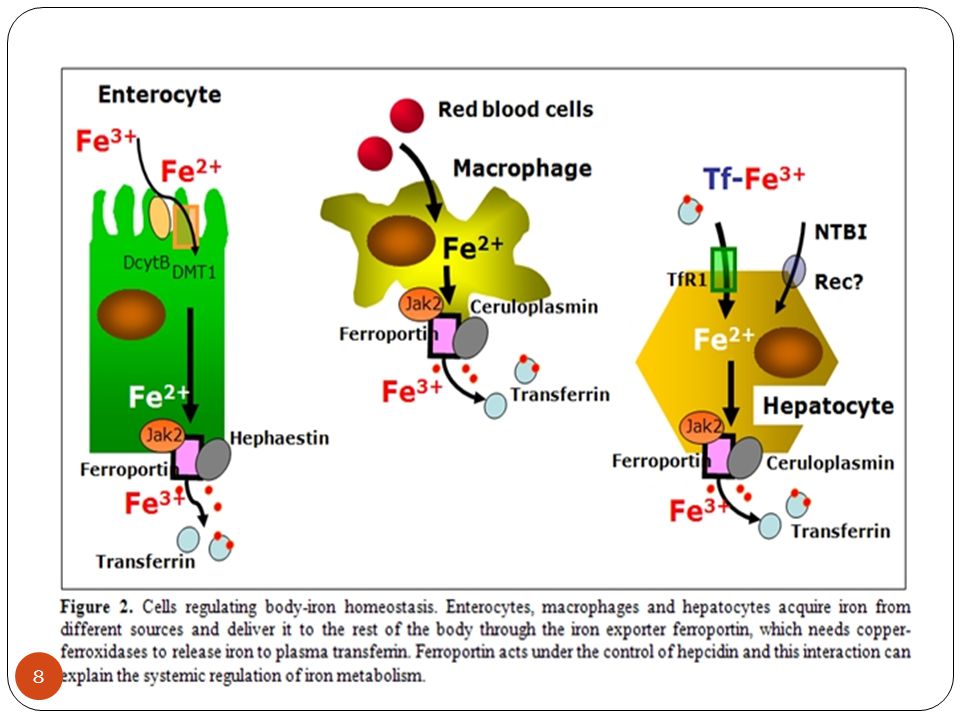
Availability of iron for heme synthesis Amount of iron: 2 g in women and 6 g in men Clinically, decreased ferritin levels usually indicate the need for prescription of iron supplements.

9
Red Cell Production Until 5, almost all bones; After 20, membranous bones Approximately 1% of total RBC is generated from bone marrow each day Reticulocyte count serves as an index of erythropoietic activity of bone marrow

10
Stages of Erythropoiesis
Hematopoietic stem cell (HSCs) Unipotent committed stem cell Proerythroblast (15-20 mm) Early normoblast (12-16 mm) Intermediate normoblast (10-14 mm) Haemoglobinization begins Late normoblast (10-14 mm) Haemoglobinization ++ Nuclear disintegration Reticulocyte (7-8 mm) Nucleus remains only as strands of reticular element Erythrocyte (7.5 mm) IL-1, IL-6, IL-3 (interleukins) GM-CSF, G-CSF, SCF Erythropoietin GM-CSF
 Unipotent committed stem cell. Proerythroblast (15-20 mm) Early normoblast (12-16 mm) Intermediate normoblast (10-14 mm) Haemoglobinization begins. Late normoblast (10-14 mm) Haemoglobinization ++ Nuclear disintegration. Reticulocyte (7-8 mm) Nucleus remains only as strands of reticular element. Erythrocyte (7.5 mm) IL-1, IL-6, IL-3 (interleukins) GM-CSF, G-CSF, SCF. Erythropoietin. GM-CSF.")
11
Red Cell Production

12
Red Cell Maturation Reduction in the cell size
Increase in the amount of haemoglobin Disappearance of nucleus, and Change in staining characteristics of cytoplasm: basophilic to eosinophilic. This is partly due to a fall in content of RNA.

13
Erythropoietin

14
Human Erythropoietin Produced by recombinant DNA technology
Used for anaemia induced by chemotherapy in cancer patients, and HIV infected persons treated with zidovudine In severe anaemia, retic count may be as much as 30% (normal about 1%); numerous erythroblasts may appear in the blood
; numerous erythroblasts may appear in the blood.")
15
Destruction of Red Blood Cells

16
Excretion of Bilirubins
Excess bilirubin elimination leads to bilirubin gallstones If red cell destruction and bilirubin production is excessive, yellow discoloration of the skin, jaundice, occurs due to accumulation of unconjugated bilirubin

17
Haemoglobinuria Haemoglobin binding protein – Haptoglobin – in the plasma Other plasma proteins – albumin – also binds to Hb Extensive destruction of RBCs (haemolytic transfusion reactions), binding capacity is exceeded Haemoglobinaemia and haemoglobinuria results
, binding capacity is exceeded. Haemoglobinaemia and haemoglobinuria results.")
18
Red Cell Metabolism 2,3-DPG decreases affinity of Hb for O2, facilitating the release of O2 at tissue levels Increased 2,3-DPG occurs in chronic hypoxia such as chronic lung diseases, anemia and residence at high altitude

19
Inhibition of Oxygen Haemoglobin Binding
Certain chemicals : nitrates and sulfates Hb reacts with nitrite to form methaemoglobin G6PD deficiency predisposes to oxidative denaturation of hemoglobin with resultant red cell injury and lysis (oxidative stress generated by infection or exposure to certain drugs)
")
20
Laboratory Tests Using automated blood cell counters: red cell content and indices Red cell indices are used to differentiate type of anemias by size or color of red cells Haemoglobin Hematocrit Mean corpuscular volume (MCV falls in microcytic and rises in macrocytic anemia) Mean corpuscular haemoglobin concentration (normochromic or normal MCHC; hypochromic or decreased color or decreased MCHC)
 Mean corpuscular haemoglobin concentration (normochromic or normal MCHC; hypochromic or decreased color or decreased MCHC)")
21
Laboratory Tests Mean cell haemoglobin
A stained blood smear: information about size, color and shape of red cells and the presence of immature or abnormal cells If blood smear is abnormal, bone marrow examination may be indicated Bone marrow aspiration from posterior iliac crest or the sternum

22
Red cell count and Haemoglobin severity of anemia
Red cell characteristics Size normocytic, microcytic or macrocytic Color normochromic, hypochromic Shape the cause of anemia

23
Anemia Values of hemoglobin, hematocrit or RBC counts which are more than 2 standard deviations below the mean HGB<13.5 g/dL (men) <12 (women) HCT<41% (men) <36 (women) Normal Hb Concentration Western value Myanmar value Male : 16 g / dL ( g/dL) g / dL Female : 14 g / dL ( g/dL) g / dL
 <12 (women) HCT<41% (men) <36 (women) Normal Hb Concentration. Western value Myanmar value. Male : 16 g / dL ( g/dL) 14.4 g / dL. Female : 14 g / dL ( g/dL) 12.5 g / dL.")
24
Pathophysiology of Anemia
Blood Loss Decreased Production (lack of nutritional elements or bone marrow failure) Increased Destruction (haemolysis)
 Increased Destruction (haemolysis)")
25
Effects of Anemia Manifestations of impaired oxygen transport and the resultant compensatory mechanisms Reduction in red cell indices and hemoglobin levels Signs and symptoms associated with the pathophysiologic process that causes anemia Manifestations depend on its severity, the rapidity of its development and the person’s age and health status

26
Symptoms of Anemia

27
Impaired oxygen transport and tissue hypoxia
Weakness, fatigue, dyspnoea and angina Brain hypoxia results in headache, faintness and dim vision Redistribution of blood results in pallor of skin, conjunctiva, mucous membranes and nail beds

28
Compensatory Mechanisms
Tachycardia, palpitations and increased cardiac output A flow type of systolic murmur Ventricular hypertrophy and high output heart failure Accelerated erythropoiesis results in diffuse bone pain and sternal tenderness Haemolytic anemia : jaundice Aplastic anemia : petechiae and purpura due to reduced platelet functions

29
Blood Loss Anemias Depends on rate of haemorrhage and blood loss is external or internal Rapid loss causes circulatory shock and collapse; fall in red cell count, Hb, hematocrit due to fluid shift into vessels Initially red cells are normocytic, normochromic Increased erythropoietin and retic count Slow loss (GI bleeding, menstrual disorders) causes anemia; signs and symptoms develop if the amount of red cell mass loss reach 50% (Hb <8 g/dL)(iron deficiency anemia) External bleeding leads to iron loss and iron deficiency
 causes anemia; signs and symptoms develop if the amount of red cell mass loss reach 50% (Hb <8 g/dL)(iron deficiency anemia) External bleeding leads to iron loss and iron deficiency.")
30
Haemolytic Anemias Characterized by premature destruction of red cells, retention in the body of iron and other products of Hb destruction and increased erythropoiesis Normocytic normochromic red cells Increased retic count in the circulating blood Haemoglobinemia, haemoglobinuria, jaundice, haemosiderinuria

31
Haemolytic Anemias Intravascular haemolysis is less common, caused by complement fixation in transfusion reactions, mechanical injury or toxic factors Extravascular haemolysis occurs when RBCs are less deformable to traverse splenic sinusoids, characterized by anemia and jaundice Intrinsic : defects of red cell membrane, haemoglobinopathies (sickle cell disease and thalassemias) and enzymes defect Extrinsic or acquired : drugs, bacteria and other toxins, antibodies and physical trauma
 and enzymes defect. Extrinsic or acquired : drugs, bacteria and other toxins, antibodies and physical trauma.")
32
Inherited Disorders of Red Cell Membrane
Hereditary spherocytosis : abnormalities of spectrin and ankyrin Mild hemolytic anemia, jaundice, splenomegaly and bilirubin gallstones Splenectomy done to reduce red cell destruction and blood transfusion in a crisis

33
Sickle Cell Disease Haemoglobin S (point mutation in the β chain of Hb, valine for glutamic acid) Haemolytic anaemia, jaundice, gallbladder stones, pain and organ failure (infarction of organs) Hb S becomes sickled when deoxygenated or at a low oxygen Deoxygenated Hb aggregates and polymerizes in the cytoplasm, creating a semisolid gel that changes the shape and deformability of the cell
 Hb S becomes sickled when deoxygenated or at a low oxygen. Deoxygenated Hb aggregates and polymerizes in the cytoplasm, creating a semisolid gel that changes the shape and deformability of the cell.")
34
Red Cell Sickling Chronic hemolytic anemia Blood vessel occlusion
Associated conditions: cold, stress, physical exertion, infection, illnesses that cause hypoxia, dehydration or acidosis

35
Features of Sickle Cell Disease

36
Diagnosis and Treatment
Neonates : clinical findings and haemoglobin electrophoresis Prenatal diagnosis : analysis of fetal DNA by amniocentesis Prevention of sickling episodes, symptomatic treatment and treatment of complications (prophylactic penicillin and full immunization) Cytotoxic drug – hydroxyurea – to allow synthesis of more HbF and less HbS Nitric oxide appears to be a promising new drug Bone marrow or stem cell transplantation
 Cytotoxic drug – hydroxyurea – to allow synthesis of more HbF and less HbS. Nitric oxide appears to be a promising new drug. Bone marrow or stem cell transplantation.")
37
Thalassemias Inherited disorders of haemoglobin synthesis and decreased synthesis of α or β globin chains of HbA Heterozygous or homozygous

38
Thalassemias β thalassemias – Cooley anaemia or Mediterranean anemia – common in Mediterranean population of southern Italy and Greece α thalassemias more common among Asians Anemia due to low production of affected chain and continued production and accumulation of unaffected globin chain Reduced Hb synthesis leads to hypochromic microcytic anemia; accumulation of unaffected chain interferes with normal red cell maturation, and membrane changes leading to hemolysis and anemia

39
β - thalassemias Excess α chains are denatured to form precipitates (Heinz bodies) in the bone marrow red cell precursors Heinz bodies impair DNA synthesis and damage to red cell membrane Coagulation abnormalities, thrombotic events (stroke and pulmonary embolism) in moderate to severe form
 in moderate to severe form.")
40
Pathophysiology of β - thalassemias
Thinning of cortical bones

41
Treatment of β - thalassemias
Regular transfusion to maintain Hb at 9 to 10 g/dL Iron chelation therapy to reduce iron load Stem cell transplantation Stem cell gene replacement

42
α - thalassemias Synthesis of globin chains is controlled by 4 genes
Deletion of single gene : silent carrier; two genes is α thalassemia trait Deletion of three genes leads to unstable aggregates of α chains – HbH Four globin chains are deleted : Hb Bart (extremely high oxygen affinity, cannot release oxygen in the tissues Chronic hemolytic anemia

43
Inherited Enzymes Defect
G6PD deficiency RBCs vulnerable to oxidants, direct oxidation of Hb to methaemoglobin, and denaturation of Hb to form Heinz bodies Anti-malaria drug primaquine, the sulfonamides, nitrofurantoin, aspirin, phenacetin, some chemotherapeutics and other drugs cause hemolysis Diagnosed through G6PD assay or screening test

44
Acquired Hemolytic Anaemias
By direct membrane destruction or antibody mediated lysis Various chemicals, toxins, venoms, malaria infection, prosthetic heart valves, vasculitis, severe burns, septicaemia, thrombotic thrombocytopenic purpura, renal disease Warm reacting antibodies (IgG) and cold reacting antibodies (IgM) Warm antibodies bind with Ag on red cell membrane (Rh Ag), resulting in spherocytosis and destruction by RE system Cold antibodies activate complements; as in lymphoproliferative disorder and idiopathic
 and cold reacting antibodies (IgM) Warm antibodies bind with Ag on red cell membrane (Rh Ag), resulting in spherocytosis and destruction by RE system. Cold antibodies activate complements; as in lymphoproliferative disorder and idiopathic.")
45
Rh incompatibility

47
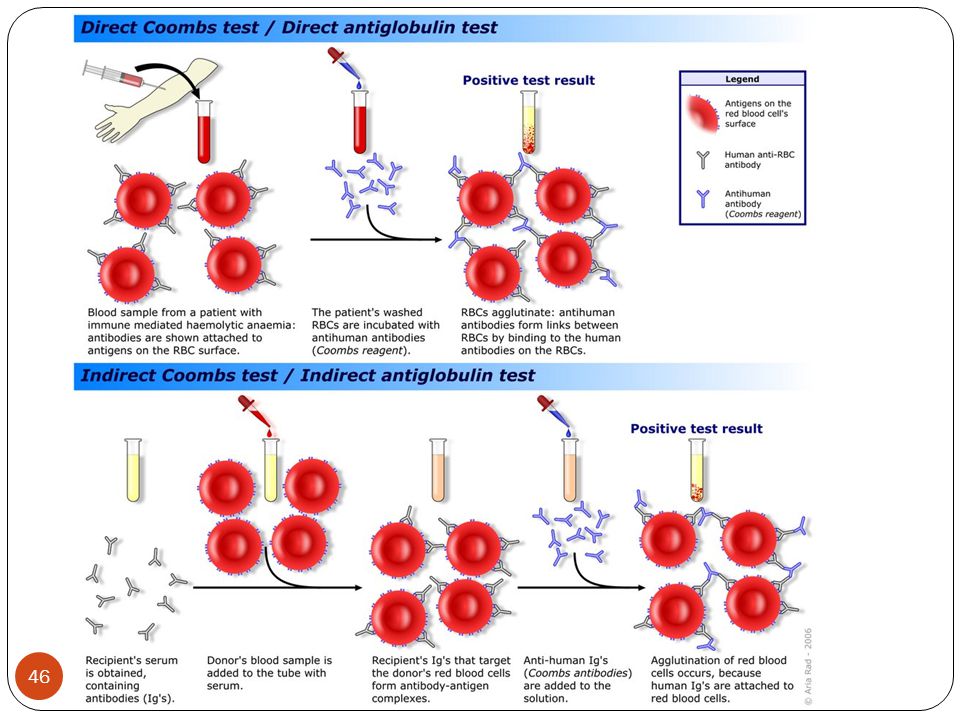
Coomb’s Test Direct Antiglobulin Test (DAT) is positive in autoimmune hemolytic anaemia, erythroblastosis fetalis, transfusion reactions, transfusion reactions and drug induced hemolysis Indirect antiglobulin test is used for antibody detection and crossmatching before transfusion
 is positive in autoimmune hemolytic anaemia, erythroblastosis fetalis, transfusion reactions, transfusion reactions and drug induced hemolysis. Indirect antiglobulin test is used for antibody detection and crossmatching before transfusion.")
48
Anemias of Deficient Red Cell Production
Deficiency of nutrients for hemoglobin synthesis (iron) Deficiency of nutrients for DNA synthesis (Cobalamin or folic acid) Marrow is replaced by nonfunctional tissues
 Deficiency of nutrients for DNA synthesis (Cobalamin or folic acid) Marrow is replaced by nonfunctional tissues.")
49
Iron Deficiency Anemia
Dietary deficiency (vegetarians) Loss of iron through bleeding (peptic ulcer, polyps, cancer, menstrual bleeding) Increased demands (growing children, pregnancy)
 Loss of iron through bleeding (peptic ulcer, polyps, cancer, menstrual bleeding) Increased demands (growing children, pregnancy)")
50
Iron Metabolism

51
Characteristics of Iron Deficiency Anemia
Low haemoglobin and hematocrit Decreased iron stores, low serum iron and ferritin Red cells number decreased and are microcytic and hypochromic Poikilocytosis (irregular shape) Anisocytosis (irregular size) Reduced MCHC and MCV Membrane changes predispose to hemolysis
 Anisocytosis (irregular size) Reduced MCHC and MCV. Membrane changes predispose to. hemolysis.")
52
Manifestations of Iron Deficiency Anemia

53
Treatment of Iron Deficiency Anemia
Prevention and treatment of the cause Ferrous sulfate Parenteral iron (iron dextran or sodium ferric gluconate) Initial test dose to prevent severe anaphylactic reactions
 Initial test dose to prevent severe anaphylactic reactions.")
54
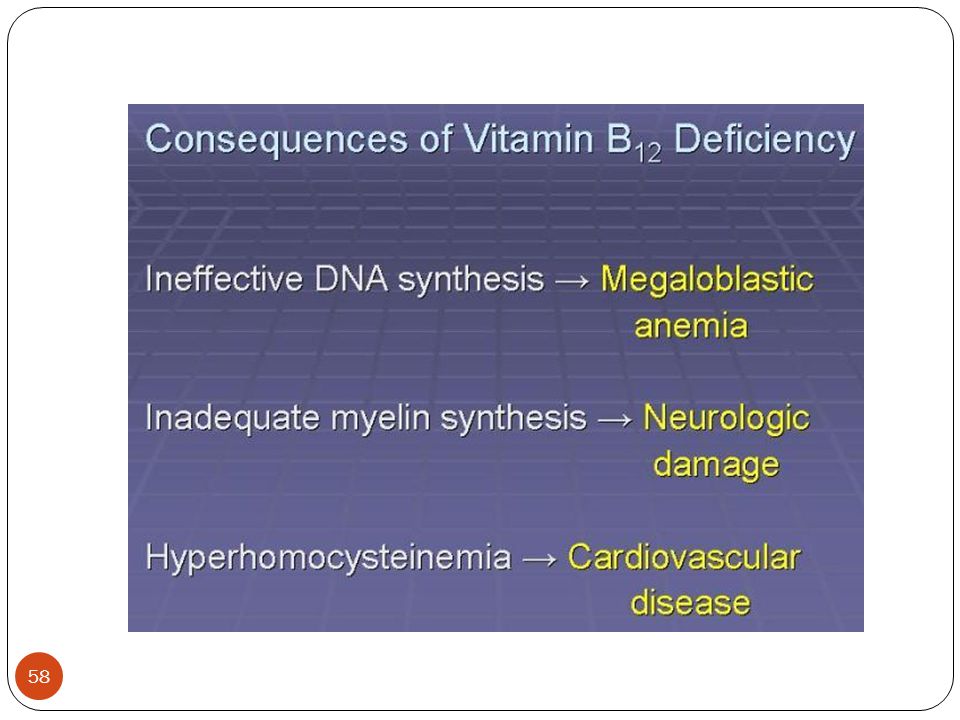
Megaloblastic Anemia Impaired DNA synthesis
Enlarged red cells (MCV >100 fL) Develop slowly Vitamin B12 and folic acid deficiency
 Develop slowly. Vitamin B12 and folic acid. deficiency.")
55
Vitamin B12 Deficiency Anemia: B12 Absorption

56
Pernicious Anemia Atrophic gastritis
Autoimmune destruction of gastric mucosa Gastrectomy, ileal resection, inflammation or neoplasms in terminal ileum, malabsorption syndrome MCV elevated; MCHC is normal

57
Vitamin B12 Containing Food
Normal body stores of 1000 to 5000 µg provide the daily requirement of 1 µg for a number of years. Therefore, deficiency develops slowly

59
Diagnosis of B12 Deficiency
The Shilling test – 24 hour urinary excretion of radiolabelled vitamin B12 administered orally Detection of parietal cell and intrinsic factor antibodies Lifelong intramuscular or high oral doses of vitamin B12 is required

60
Folic Acid

61
Folic Acid Deficiency Total body stores amount to 2000 to 5000 µg and 50µg is required in the daily diet. A dietary deficiency may result in anaemia in a few months Pregnancy increases the need for folic acid 5 to 10 fold

62
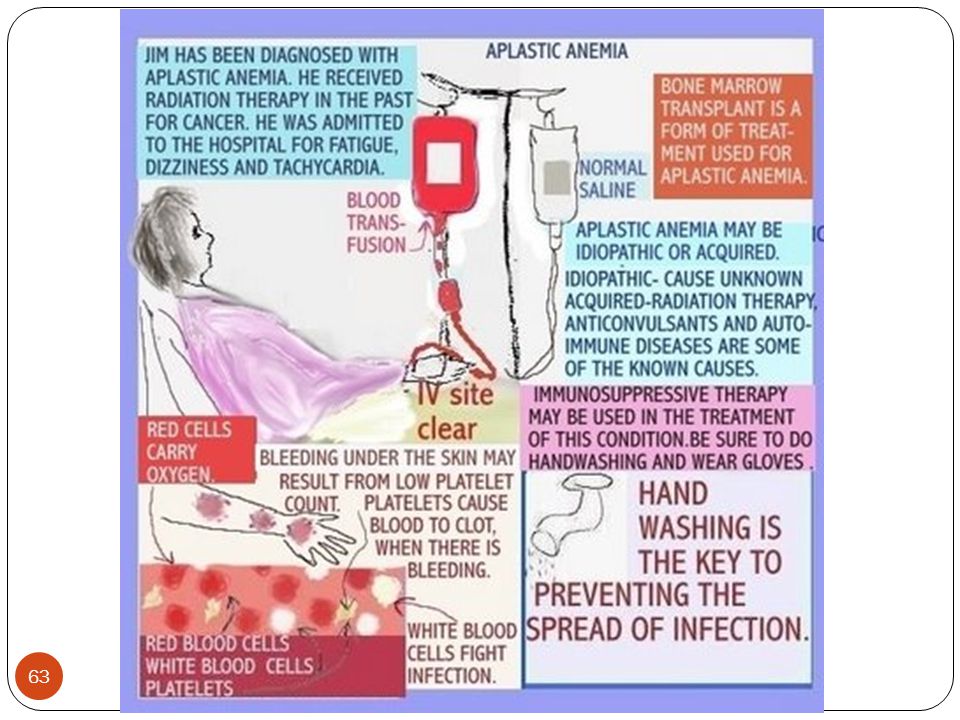
Aplastic Anemia Reduction of all 3 hemopoietic cell lines
Onset may be insidious but may be abrupt and severe

64
Therapy in Aplastic Anemia

65
Therapy in Aplastic Anemia
Immunosuppressive therapy with lymphocyte immune globulin Avoid offending agents Antibiotics for infection Red cell transfusion to correct anaemia Platelets and corticosteroid therapy to minimize bleeding

66
Chronic Disease Anemia
Occur as a complication of chronic infections, inflammation, cancer and chronic kidney diseases Short red cell life span; deficient red cell production; a blunted response to erythropoietin, and low serum iron Mild anemia – normocytic and normochromic – with low reticulocyte counts In chronic renal diseases, uremic toxins and retained nitrogen interfere with actions of erythropoietin; hemolysis and blood loss associated with hemodialysis and bleeding tendencies also contribute to anemia

67
Therapy in Chronic Disease Anemia
Short-term erythropoietin therapy Iron supplementation Blood transfusions In future – iron chelating agents and cytokines to stimulate erythropoietin production

68
Thank You

Similar presentations



















 Course code: MLHE-201 Supervisor: Prof>")