Download presentation
Presentation is loading. Please wait.

1
Linked Metabolic Abnormalities:
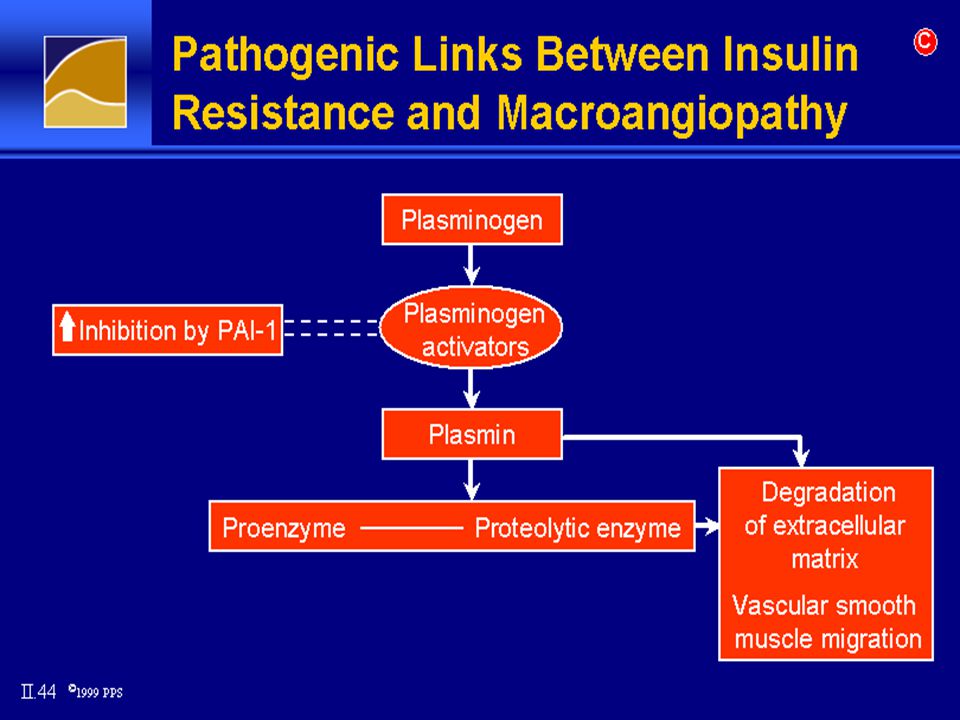
Impaired glucose handling/ insulin resistance Atherogenic dyslipidemia Endothelial dysfunction Prothrombotic state Hemodynamic changes Proinflammatory state Excess ovarian testosterone production Sleep-disordered breathing 1. IGT. IFG, DM 2. Incr. TG, Decr. HDL, Increased concentration small dense LDL particles, Increased post-meal accuumulation of TG-rich lipoproteins 3. Monomucear cell adhesion, Decreased endothel. Dependent vasodil Incr. Plasma conc. Cellular adhesion molecules, microal bumenuria 4. Increased fibrinogen, Pkasminogen activator inhibitor-I 5. Increased Sympathetic nervous syctem activity, Increased renal sodium retention 6. Inflammatory cytokines (liver/ fat) CRP, acute phase reactants
 CRP, acute phase reactants.")
2
Resulting Clinical Conditions:
Type 2 diabetes Essential hypertension Polycystic ovary syndrome (PCOS) Nonalcoholic fatty liver disease Sleep apnea Cardiovascular Disease (MI, PVD, Stroke) Cancer (Breast, Prostate, Colorectal, Liver)
 Nonalcoholic fatty liver disease. Sleep apnea. Cardiovascular Disease (MI, PVD, Stroke) Cancer (Breast, Prostate, Colorectal, Liver)")
3
Multiple Risk Factor Management
Obesity Glucose Intolerance Insulin Resistance Lipid Disorders Hypertension Goals: Minimize Risk of Type 2 Diabetes and Cardiovascular Disease

4
Glucose Abnormalities:
IDF: FPG >100 mg/dL (5.6 mmol. L) or previously diagnosed type 2 diabetes WHO: Presence of diabetes, IGT, IFG, insulin resistance ATP III: FBS >110 mg/dL, <126 mg/dL ( mmol/L ) (ADA: FBS >100 mg/dL [ 5.6 mmol/L ])
 or previously diagnosed type 2 diabetes. WHO: Presence of diabetes, IGT, IFG, insulin resistance. ATP III: FBS >110 mg/dL, <126 mg/dL ( mmol/L ) (ADA: FBS >100 mg/dL [ 5.6 mmol/L ])")
5
Hypertension: IDF: BP >130/85 or on Rx for previously diagnosed hypertension WHO: BP >140/90 NCEP ATP III: BP >130/80

6
Dyslipidemia: IDF: Triglycerides - >150mg/dL (1.7 mmol /L)
HDL - <40 mg/dL (men), <50 mg/dL (women) WHO: Triglycerides - >150 mg/dL (1.7 mmol/L) HDL - <35 mg/dL (men), >39 mg/dL) women ATP III: Same as IDF
, <50 mg/dL (women) WHO: Triglycerides - >150 mg/dL (1.7 mmol/L) HDL - <35 mg/dL (men), >39 mg/dL) women. ATP III: Same as IDF.")
7
Adipokines and Metabolic Syndrome
Adipocytokines and Insulin Resistance Adipokines and Metabolic Syndrome Adipocytokines have been associated with obesity and type 2 diabetes. This figure depicts a hypothetical model of the mechanism by which increased adiposity may contribute to insulin resistance and endothelial dysfunction. Lyon CJ, et al. Endocrinology. 2003;144:

8
Growth & Proliferation
INSULIN MODULATION OF ENDOTHELIAL ACTIVITIES I n s u l i G t 4 N O M A P K R S - 1 3 IL-1 IL-6 TNFa CCR-2 MMP VCAM PAI-1 VEGF Growth & Proliferation Transcription Factors

10
Insulin Resistance: Hyperinsulinemic individuals are at risk for developing Diabetes, Dyslipidemia, Hypertension & ultimately Cardiovascular disease Patients with Metabolic Syndrome are 3.5 times as likely to die from Cardiovascular disease compared to normal people

11
Screening/Public Health Approach
Public Education Screening for at risk individuals: Blood Sugar/ HbA1c Lipids Blood pressure Tobacco use Body habitus Family history Public education is key! Recognizing risk factors and dealing with them is important, Recognizing clusters of risk factors is important, i.e, when some of the factors are recognized others should be investigated. Using the correct drugs to treat the various risk factors is important. ACEI or ARB TZD’s or Glitazars Metformin Statins with or without fibric acid derivatives Treating to goal. Smoking cessation.

12
Life-Style Modification: Is it Important?
Exercise Improves CV fitness, weight control, sensitivity to insulin, reduces incidence of diabetes Weight loss Improves lipids, insulin sensitivity, BP levels, reduces incidence of diabetes Goals: Brisk walking min./day 10% reduction in body wt. Finnish Diaabetes Prevention Study - 30 min. walking/day DPP - Life-style modification 58% effective in preventing diabetes vs 31% for metformin. Weight loss is difficult to achieve and maintain. Can be done. New medications are being developed to assist with this. Life-style modification programs do not necessarily require professional health care providers to be successful. Smoking cessation is KEY. Can be more successful with use of counselling, and pharmacologic support - Transdermal nicotine, bupropion or nortriptyline.

13
Smoking Cessation / Avoidance:
A risk factor for development in children and adults Both passive and active exposure harmful A major risk factor for: insulin resistance and metabolic syndrome macrovascular disease (PVD, MI, Stroke) microvascular complications of diabetes pulmonary disease, etc.
 microvascular complications of diabetes. pulmonary disease, etc.")
14
Diabetes Control - How Important?
For every 1% rise in Hb A1c there is an 18% rise in risk of cardiovascular events & a 28% increase in peripheral arterial disease Evidence is accumulating to show that tight blood sugar control in both Type 1 and Type 2 diabetes reduces risk of CVD Goals: FBS - premeal <110, postmeal <180. HbA1c <7%

15
Overcome Insulin Resistance/ Diabetes:
Insulin Sensitizers: Biguanides - metformin PPAR α, γ & δ agonists – Glitazones, Gltazars Rosiglitazon, Pioglitazon Can be used in combination Insulin Secretagogues: Sulfonylurea - glipizide, glyburide, glimeparide, glibenclamide Meglitinides - repaglanide, netiglamide Metformin useful in overwt., insulin resistant people with nl renal function. Suppresses appetite, assists with weight control. Use of Metformin diabetic patients with heart failurehas recently been reported to be associated with lower morbidity and mortality compared to sulfonylurea drugs Glimeparide better than other sulfonylurea drugs in patients with MI TZD’s are selective PPAR gamma selective - Improve insulin sensitivity but also improve FFA metabooism and markers of inflammation (Cardio CRP) and lipids. Do cause adipocyte proliferation and lipid storage in adipocytes, ie, weight gain. Pioglitazone has more alpha agonist effect than does rosiglitazone and therefore has more favorable effect on lipids (Incr. HDL, Decr. Trigl and VLDL) TZD’s also protective in early glucose intolerance from development of diabetes. Two Glitazars now in phase III trials. These are dual PPARs- Muraglitazar - more effective in lowering Hg A1c and triglycerides than pioglitazone. Tesaglitazar - similar to muraglitazar but associated with more weight gain.
 and lipids. Do cause adipocyte proliferation and lipid storage in adipocytes, ie, weight gain. Pioglitazone has more alpha agonist effect than does rosiglitazone and therefore has more favorable effect on lipids (Incr. HDL, Decr. Trigl and VLDL) TZD’s also protective in early glucose intolerance from development of diabetes. Two Glitazars now in phase III trials. These are dual PPARs- Muraglitazar - more effective in lowering Hg A1c and triglycerides than pioglitazone. Tesaglitazar - similar to muraglitazar but associated with more weight gain.")
16
Insulin Insulin Analogues: Lyspro /Aspart /glulysine used with meals
Glargine & Livemer as basal insulin Continuous Subcutaneous Insulin Infusion (CSII) NPH/Regular, NPH/logs - Mixed or in fixed combinations (70/30, 75/25, 50/50) Insulin combined with oral agents Short-acting analogs: Onset - 15 min. Peak hrs. Duration: 4-6 hrs. Reg.: Onset min. Peak:2-4 hrs. Duration: 6-8 hrs. Glargine: Onset hrs. Peak: flat. Duration: 24 hrs R Insulin analogues offer a much more physiologic insulin profile than do older insulin preparations and allow development of a treatment strategy that gives patients much more dietary freedom using a basal-bolus insulin with carbohydrate counting. CSII provides the ultimate in physiologic insulin delivery and will soon be linked to a continuous glucose monitoring technology that brings insulin treatment closer to the dream of a closed loop system or “artificial pancreas”.
 NPH/Regular, NPH/logs - Mixed or in fixed combinations (70/30, 75/25, 50/50) Insulin combined with oral agents. Short-acting analogs: Onset - 15 min. Peak hrs. Duration: 4-6 hrs. Reg.: Onset min. Peak:2-4 hrs. Duration: 6-8 hrs. Glargine: Onset hrs. Peak: flat. Duration: 24 hrs. R. Insulin analogues offer a much more physiologic insulin profile than do older insulin preparations and allow development of a treatment strategy that gives patients much more dietary freedom using a basal-bolus insulin with carbohydrate counting. CSII provides the ultimate in physiologic insulin delivery and will soon be linked to a continuous glucose monitoring technology that brings insulin treatment closer to the dream of a closed loop system or artificial pancreas .")
17
BP Control - How Important?
MRFIT and Framingham Heart Studies: Conclusively proved the increased risk of CVD with long-term sustained hypertension Demonstrated a 10 year risk of cardiovascular disease in treated patients vs non-treated patients to be 0.40. 40% reduction in stroke with control of HTN Precedes literature on Metabolic Syndrome Goal: BP.<130/80

18
Lipid Control - How Important?
Multiple major studies show % reductions in cardiovascular disease risk with use of statins and fibrates in the control of hyperlipidemia. Goals: LDL <100 mg/dL (<3.0 mmol /l) (high risk <70 mg/dL- <2.6 mmol/L) TG <150 mg% (<1.7 mmol /l) HDL >40 mg% (>1.1 mmol /l)
 (high risk <70 mg/dL- <2.6 mmol/L) TG <150 mg% (<1.7 mmol /l) HDL >40 mg% (>1.1 mmol /l)")
19
Medications: Hypertension: ACE inhibitors, ARBs
Others - thiazides, calcium channel blockers, beta blockers, alpha blockers Central acting Alfa agonist : Moxolidin Dylipidemia: Statins, Fibrates, Niacin Platelet inhibitors: ASA, clopidogrel RAAS interruption improvescardioprotection, improved insulin sensitivity, slow nephropathy - reduces membrane permeability to albumen, maxangial matrix expansion and intraglomerular pressure. Influence adipocyte differentiation. ACEI and ARB drugs not only effective in controlling hypertension and providing renal protection but also seem to be effective in lowering the odds of risk of developing Type 2 diabetes in those patients who are at risk. Another reason for trying to identify those who are at risk. Diabetes Care Sept Must watch renal function and potassium Vasodilating Beta Blockers are useful in BP control, may improve insulin sensitivity. ASA - 30% reduction in MI and 20% reduction in CVA

20
Antihypertensive Medications:
Angiotensin -converting Enzyme Inhibitors (ACEI) Angiotensin II Receptor (ARB) Blockers Combination with Thiazides, Calcium Channel Blockers, Cardioselective Beta Blockers Target BP: <130/80 ACEI’s and ARB’s lower BP but also provide renal protection from nephropathy and lower risk of developing Type 2 diabetes in those who are at risk. Should be first line Rx for HTN in metabolic syndrome. Often combinations of antihypertensives must be used to achieve target BP levels.
 Angiotensin II Receptor (ARB) Blockers. Combination with Thiazides, Calcium Channel Blockers, Cardioselective Beta Blockers. Target BP: <130/80. ACEI’s and ARB’s lower BP but also provide renal protection from nephropathy and lower risk of developing Type 2 diabetes in those who are at risk. Should be first line Rx for HTN in metabolic syndrome. Often combinations of antihypertensives must be used to achieve target BP levels.")
21
A Critical Look at the Metabolic Syndrome
Is it a Syndrome?* “…too much clinically important information is missing to warrant its designations as a syndrome.” Unclear pathogenesis, Insulin resistance may not underlie all factors, & is not a consistent finding in some definitions. CVD risks associated with metabolic syndrome has not shown to be greater than the sum of it’s individual components. *ADA & EASD Diagnostic criteria from ATP III, WHO and IDF vary enough that different segments of populations are identified as having MS . Emphasizes the need to treat individually all components of the syndrome. It is still important to recognize that clustering of CVD risk factor does occur and to be astute in looking for and addressing all the factors. As more research is done the underlying common biochemical denominators are being identified and medications are being developed that address the root causes of the various components of the syndrome.

22
A Critical Look at the Metabolic Syndrome
“Until much needed research is completed, clinicians should evaluate and treat all CVD risk factors without regard to whether a patient meets the criteria for diagnosis of the ‘metabolic syndrome’.” The advice remains to treat individual risk factors when present & to prescribe therapeutic lifestyle changes & weight management for obese patients with multiple risk factors.

23
Individual metabolic abnormalities among Qatari population according to gender (Musallam et al 08)
Men (n = 405) Women (n=412) Variable n(%) n(%) p-Value ATP III Abdominal obesity 227(56.0) 308(74.8) <0.001 Hypertension 143(35.3) 156(37.9) Diabetes 77(19.0) 107(26.0) Hypertriglyceridemia 113(27.9) 83(20.1) Low HDL 95(23.5) 121(29.4)
 Women (n=412) Variable n(%) n(%) p-Value. ATP III. Abdominal obesity 227(56.0) 308(74.8) < Hypertension 143(35.3) 156(37.9) Diabetes 77(19.0) 107(26.0) Hypertriglyceridemia 113(27.9) 83(20.1) Low HDL 95(23.5) 121(29.4)")
24
Individual metabolic abnormalities among Qatari population according to gender
No of components of ATP III Men (n = 405) Women (n=412) Variable n(%) n(%) p-Value None 88(21.7) 74(18.0) – One (25.4) 100(24.3) Two (30.9) 111(26.9) – Three or more 89(22.0) 127(30.8) –
 Women (n=412) Variable n(%) n(%) p-Value. None 88(21.7) 74(18.0) – One 103(25.4) 100(24.3) Two 125(30.9) 111(26.9) – Three or more 89(22.0) 127(30.8) –")
25
Multivariate logistic regression analysis of factors associated with Metabolic Syndrome according to (ATP III criteria) Odds ratio 95% CI p-Value Age –1.09 <0.001 Female gender – Body Mass Index –1.07 <0.001 Fam his of DM – Smoking –

26
Prevalence of MeS in different Countries
Sample Year Country 23 542 2003 Arab Americans 21 1419 2001 Oman 36 1121 2002 Jordan 20.8 2250 2004 Saudi Arabia 17* 1998 Palestine 27.6 817 2007 Qatar 33.4* 1637 Turkey 33.7 10368 ? Iran * Crude rates Mussallam et al. Int J Food Safety and PH 2008

27
Prevalence of MeS in different Countries
Sample Year Country 34* 2002 2005 USA 21 1419 Greece 15.3 4060 South Australia 6.8 40,698 2001 S. Korea 10.2* 2776 2000 China 33.4* 1637 2004 Turkey 41* 475 2003 Chennai India 27.6 817 Qatar * Crude rates Mussallam et al. Int J Food Safety and PH 2008

31
Thank You

Similar presentations