Download presentation
Presentation is loading. Please wait.

1
Cardiometabolic Syndrome Nabil Sulaiman HOD Family and Community Medicine, Sharjah University and University of Melbourne & Dr Dhafir A. Mahmood Consultant Endocrinologist Al- Qassimi & Al-Kuwait Hospital Sharjah

2
Cardiometabolic Syndrome II Aims Abdominal obesity prevalence Targeting Cardiometabolic Risk factors Multiple Risk Factor management A Critical Look at the Metabolic Syndrome

3
Clustering of Components: Hypertension: BP. > 140/90 Dyslipidemia: TG > 150 mg/ dL ( 1.7 mmol/L ) HDL- C < 35 mg/ dL (0.9 mmol/L) Obesity (central): BMI > 30 kg/M2 Waist girth > 94 cm (37 inch) Waist/Hip ratio > 0.9 Impaired Glucose Handling: IR, IGT or DM FPG > 110 mg/dL (6.1mmol/L) 2hr.PG >200 mg/dL(11.1mmol/L) Microalbuninuria (WHO)
 HDL- C < 35 mg/ dL (0.9 mmol/L) Obesity (central): BMI > 30 kg/M2 Waist girth > 94 cm (37 inch) Waist/Hip ratio > 0.9 Impaired Glucose Handling: IR, IGT or DM FPG > 110 mg/dL (6.1mmol/L) 2hr.PG >200 mg/dL(11.1mmol/L) Microalbuninuria (WHO).")
4
Global cardiometabolic risk* Gelfand EV et al, 2006; Vasudevan AR et al, 2005 * working definition

5
The new IDF definition focusses on abdominal obesity rather than insulin resistance International Diabetes Federation (IDF) Consensus Definition 2005
 Consensus Definition 2005")
6
Why a New Definition of the MeS: IDF Objectives Needs: To identify individuals at high risk of developing cardiovascular disease (and diabetes) To be useful for clinicians To be useful for international comparisons
 To be useful for clinicians To be useful for international comparisons")
7
Central Obesity IDF: IDF: –Central obesity - waist circumference >94 cm for Europid men, >80 Europid women with ethnicity specific values for other groups WHO: WHO: –Waist-hip ratio >0.9 - men or >0.85 - women ATP III: ATP III: –Waist circumference >40 in. - men, > 35 in. - women

8
Fat Topography In Type 2 Diabetic Subjects Intramuscular Intrahepatic Subcutaneous Intra- abdominal FFA * TNF-alpha * Leptin * IL-6 (CRP) * Tissue Factor * PAI-1 * Angiotensinogen *
 * Tissue Factor * PAI-1 * Angiotensinogen *")
9
Abdominal obesity and increased risk of cardiovascular events Dagenais GR et al, 2005 Adjusted relative risk 111 1.17 1.16 1.14 1.29 1.27 1.35 0.8 1 1.2 1.4 CVD deathMIAll-cause deaths Tertile 1 Tertile 2 Tertile 3 MenWomen <95 95–103 >103 <87 87–98 >98 Waist circumference (cm): The HOPE study Adjusted for BMI, age, smoking, sex, CVD disease, DM, HDL-cholesterol, total-C; CVD: cardiovascular disease; MI: myocardial infarction; BMI: body mass index; DM: diabetes mellitus; HDL: high-density lipoprotein cholesterol
: The HOPE study Adjusted for BMI, age, smoking, sex, CVD disease, DM, HDL-cholesterol, total-C; CVD: cardiovascular disease; MI: myocardial infarction; BMI: body mass index; DM: diabetes mellitus; HDL: high-density lipoprotein cholesterol")
10
Abdominal obesity increases the risk of developing type 2 diabetes <7171–75.976–8181.1–8686.1–9191.1–96.3>96.3 24 20 16 12 8 4 0 Relative risk Waist circumference (cm) Carey VJ et al, 1997
 Carey VJ et al, 1997")
11
Abdominal obesity is linked to an increased risk of coronary heart disease Waist circumference has been shown to be independently associated with increased age-adjusted risk of CHD, even after adjusting for BMI and other cardiovascular risk factors 0.0 0.5 1.0 1.5 2.0 2.5 3.0 <69.8 69.8 <74.2 74.2 <79.2 79.2 <86.3 86.3 <139.7 1.27 2.06 2.31 2.44 p for trend = 0.007 Relative risk Quintiles of waist circumference (cm) Rexrode KM et al, 1998 CHD: coronary heart disease; BMI: body mass index
 Rexrode KM et al, 1998 CHD: coronary heart disease; BMI: body mass index")
12
Diabetes in the new millennium Interdisciplinary problem Diabetes

13
Diabetes in the new millennium Interdisciplinary problem OBESITY

14
Diabetes in the new millennium Interdisciplinary problem DIAB ESITY

15
Targeting Cardiometabolic Risk

16
Central obesity: a driving force for cardiovascular disease & diabetes “Balzac” by Rodin Front Back

17
Intra-abdominal adiposity is closely correlated with abdominal obesity To assess IAA, the simplest measure of abdominal obesity is waist circumference, which is strongly correlated with direct measurement of IAA by CT scan or MRI, considered to be the gold standard Després JP et al, 2001; Pouliot MC et al, 2004 300 200 100 0 r = 0.80 6080100120 IAA Waist circumference (cm) IAA (cm 2 ) IAA: intra-abdominal adiposity; CT: computed tomography; MRI: magnetic resonance imaging
 IAA (cm 2 ) IAA: intra-abdominal adiposity; CT: computed tomography; MRI: magnetic resonance imaging")
18
Intra-abdominal adiposity is a major contributor to increased cardiometabolic risk Kershaw EE et al, 2004; Lee YH et al, 2005; Boden G et al, 2002 Associated with inflammatory markers (C-reactive protein) Free fatty acids Inflammation Insulin resistance Dyslipidaemia Increased cardiometabolic risk IAA = high risk fat Secretion of adipokines ( ↓ adiponectin) IAA: intra-abdominal adiposity
 Free fatty acids Inflammation Insulin resistance Dyslipidaemia Increased cardiometabolic risk IAA = high risk fat Secretion of adipokines ( ↓ adiponectin) IAA: intra-abdominal adiposity")
19
Waist Circumference

20
Intra-abdominal adiposity and dyslipidaemia Pouliot MC et al, 1992 310 248 186 124 62 0 60 45 30 mg/dL Triglycerides Lean HDL-cholesterol Visceral fat (obese subjects) LowHigh Lean Visceral fat (obese subjects) LowHigh HDL: high-density lipoprotein
 LowHigh Lean Visceral fat (obese subjects) LowHigh HDL: high-density lipoprotein")
21
Insulin Resistance: Associated Conditions

22
Targeting Cardiometaboilc Risk Defining cardiometabolic Risk Cardiovascular Disease Abdominal Obesity Glucose intolerance Insulin Resistance Dyslipedemia Hypertension

23
Targeting Cardiometaboilc Risk Defining cardiometabolic Risk Major Unmet Clinical Need Classical Risk Factors Novel Risk Factors Cluster Risk Factors LDL-C BP Smoking DM-2 Insulin HDL-C TNF & IL-6 Abdominal Obesity Glucose PAI-1 TG Cardiovascular Disease

24
Linked Metabolic Abnormalities: Impaired glucose handling/ insulin resistance Atherogenic dyslipidemia Endothelial dysfunction Prothrombotic state Hemodynamic changes Proinflammatory state Excess ovarian testosterone production Sleep-disordered breathing

25
Resulting Clinical Conditions: Type 2 diabetes Essential hypertension Polycystic ovary syndrome (PCOS) Nonalcoholic fatty liver disease Sleep apnea Cardiovascular Disease (MI, PVD, Stroke) Cancer (Breast, Prostate, Colorectal, Liver)
 Nonalcoholic fatty liver disease Sleep apnea Cardiovascular Disease (MI, PVD, Stroke) Cancer (Breast, Prostate, Colorectal, Liver)")
26
Targeting Cardiometaboilc Risk Site of Action Mechanisms Addresses Adipose tissues Adiponectin Dyslipidemia Lipogeenesis Insulin resistance Muscle G uptake Insulin resistance Liver Lipogeenesis Dyslipidemia Insulin resistance GI tract Satiety signals Body weight Waist circumference Hypothalamus Food intake Body weight Waist circumference Genetic?

27
Multiple Risk Factor Management Obesity Glucose Intolerance Insulin Resistance Lipid Disorders Hypertension Goals: Minimize Risk of Type 2 Diabetes and Cardiovascular Disease Goals: Minimize Risk of Type 2 Diabetes and Cardiovascular Disease

28
Glucose Abnormalities: IDF: IDF: –FPG >100 mg/dL (5.6 mmol. L) or previously diagnosed type 2 diabetes –(ADA: FBS >100 mg/dL [ 5.6 mmol/L ])
 or previously diagnosed type 2 diabetes –(ADA: FBS >100 mg/dL [ 5.6 mmol/L ]).")
29
Hypertension: IDF: IDF: hypertension –BP >130/85 or on Rx for previously diagnosed hypertension

30
Dyslipidemia: IDF: IDF: –Triglycerides - >150mg/dL (1.7 mmol /L) – HDL - <40 mg/dL (men), <50 mg/dL (women)
 – HDL - <40 mg/dL (men), <50 mg/dL (women)")
31
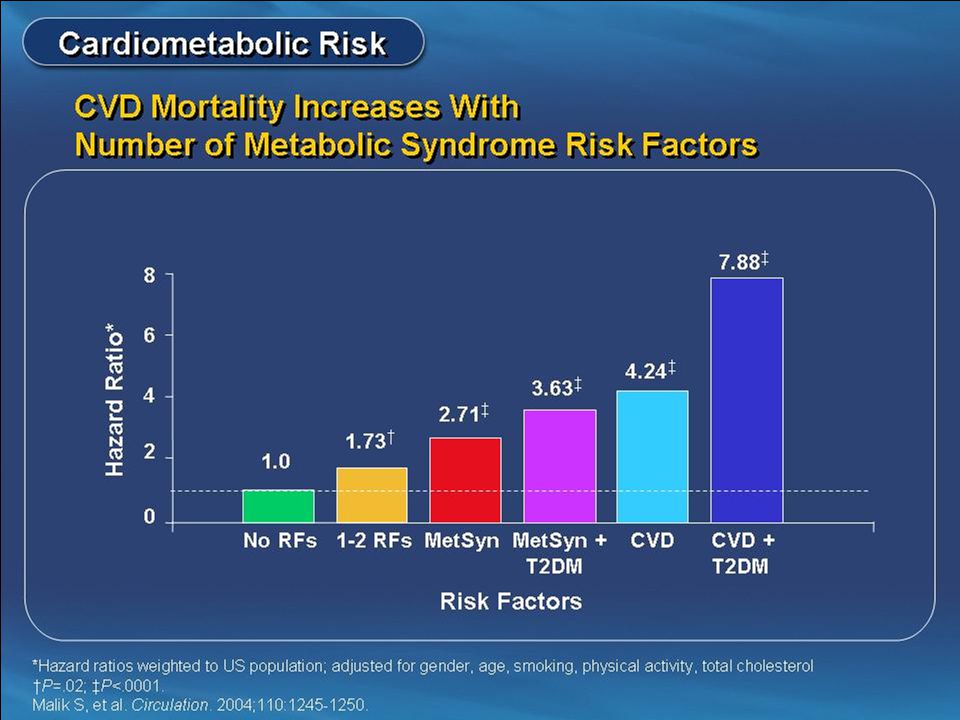
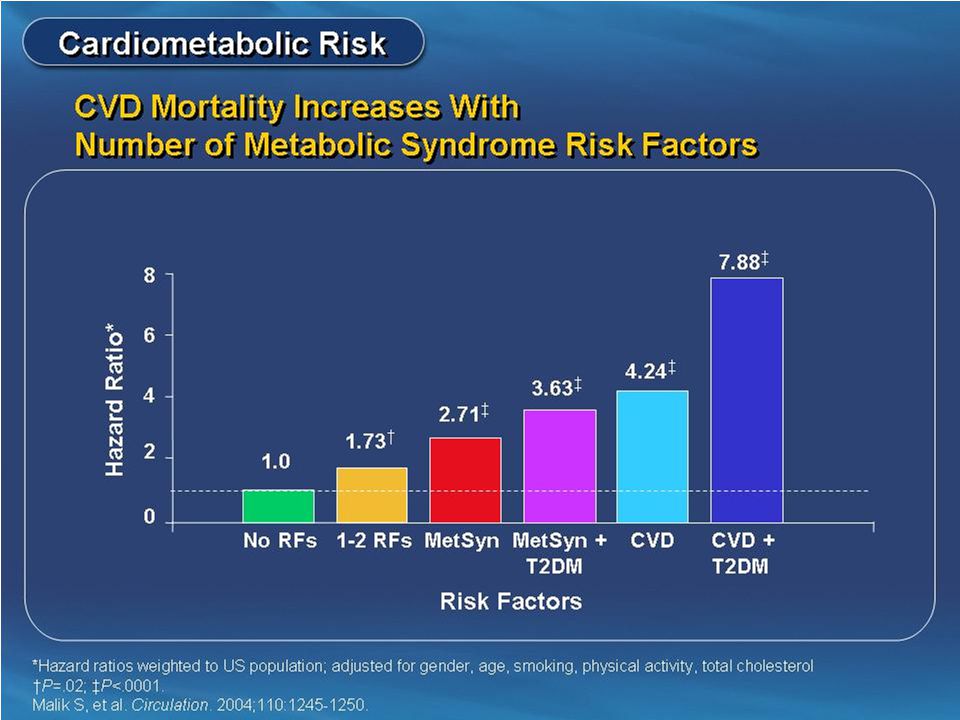
Insulin Resistance: Hyperinsulinemic individuals are at risk for developing Diabetes, Dyslipidemia, Hypertension & ultimately Cardiovascular disease Patients with Metabolic Syndrome are 3.5 times as likely to die from Cardiovascular disease compared to normal people

32
Public Health Approach

33
Screening/Public Health Approach Public Education Screening for at risk individuals: –Blood Sugar/ HbA1c –Lipids –Blood pressure –Tobacco use –Body habitus –Family history

34
Life-Style Modification: Is it Important? Exercise –Improves CV fitness, weight control, sensitivity to insulin, reduces incidence of diabetes Weight loss –Improves lipids, insulin sensitivity, BP levels, reduces incidence of diabetes Goals: Goals: Brisk walking - 30 min./day 10% reduction in body wt. 10% reduction in body wt.

35
Smoking Cessation / Avoidance: A risk factor for development in children and adults Both passive and active exposure harmful A major risk factor for: –insulin resistance and metabolic syndrome –macrovascular disease (PVD, MI, Stroke) –microvascular complications of diabetes –pulmonary disease, etc.
 –microvascular complications of diabetes –pulmonary disease, etc.")
36
Diabetes Control - How Important? Goals Goals: FBS - premeal <110, FBS - premeal <110, postmeal <180. postmeal <180. HbA1c <7% HbA1c <7% For every 1% rise in Hb A1c there is an 18% rise in risk of cardiovascular events & a 28% increase in peripheral arterial disease Evidence is accumulating to show that tight blood sugar control in both Type 1 and Type 2 diabetes reduces risk of CVD

37
Lifestyle modification Diet Exercise Weight loss Smoking cessation If a 1% reduction in HbA 1c is achieved, you could expect a reduction in risk of: 21% for any diabetes- related endpoint 37% for microvascular complications 14% for myocardial infarction However, compliance is poor and most patients will require oral pharmacotherapy within a few years of diagnosis Stratton IM et al. BMJ 2000; 321: 405–412.

38
Overcome Insulin Resistance/ Diabetes: Insulin Sensitizers: –Biguanides – metformin –Glitazones, Gltazars –Can be used in combination Insulin Secretagogues: –Sulfonylurea - glipizide, glyburide, glimeparide, glibenclamide –Meglitinides - repaglanide, netiglamide

39
Insulin Insulin Analogues: –Lyspro /Aspart /glulysine used with meals –Glargine & Livemer as basal insulin Continuous Subcutaneous Insulin Infusion (CSII) NPH/Regular, NPH/logs - Mixed or in fixed combinations (70/30, 75/25, 50/50) Insulin combined with oral agents
 NPH/Regular, NPH/logs - Mixed or in fixed combinations (70/30, 75/25, 50/50) Insulin combined with oral agents")
40
BP Control - How Important? BP. <130/80 Goal: BP. <130/80 MRFIT and Framingham Heart Studies: –Conclusively proved the increased risk of CVD with long-term sustained hypertension –Demonstrated a 10 year risk of cardiovascular disease in treated patients vs non-treated patients to be 0.40. –40% reduction in stroke with control of HTN Precedes literature on Metabolic Syndrome

41
Lipid Control - How Important? Goals:HDL >40 mg% (>1.1 mmol /l) Goals: HDL >40 mg% (>1.1 mmol /l) LDL <100 mg/dL (<3.0 mmol /l) LDL <100 mg/dL (<3.0 mmol /l) TG <150 mg% (<1.7 mmol /l) TG <150 mg% (<1.7 mmol /l) Multiple major studies show 24 - 37% reductions in cardiovascular disease risk with use of statins and fibrates in the control of hyperlipidemia.
 Goals: HDL >40 mg% (>1.1 mmol /l) LDL <100 mg/dL (<3.0 mmol /l) LDL <100 mg/dL (<3.0 mmol /l) TG <150 mg% (<1.7 mmol /l) TG <150 mg% (<1.7 mmol /l) Multiple major studies show % reductions in cardiovascular disease risk with use of statins and fibrates in the control of hyperlipidemia..")
42
Substantial residual cardiovascular risk in statin-treated patients Placebo Statin Year of follow-up % patients 0123456 10 20 30 0 Risk reduction=24% (p<0.0001) The MRC/BHF Heart Protection Study Heart Protection Study Collaborative Group, 2002 19.8% of statin-treated patients had a major cardiovascular event by 5 years
 The MRC/BHF Heart Protection Study Heart Protection Study Collaborative Group, % of statin-treated patients had a major cardiovascular event by 5 years")
43
Medications: Hypertension: –ACE inhibitors, ARBs –Others - thiazides, calcium channel blockers, beta blockers, alpha blockers –Central acting Alfa agonist : Moxolidin Dylipidemia: –Statins, Fibrates, Niacin Platelet inhibitors: –ASA, clopidogrel

45
Antihypertensive Medications: <130/80 Target BP: <130/80 Angiotensin -converting Enzyme Inhibitors (ACEI) Angiotensin II Receptor (ARB) Blockers Combination with Thiazides, Calcium Channel Blockers, Cardioselective Beta Blockers
 Angiotensin II Receptor (ARB) Blockers Combination with Thiazides, Calcium Channel Blockers, Cardioselective Beta Blockers")
48
Individual metabolic abnormalities among Qatari population according to gender (Musallam et al 08) Men (n = 405) Women (n=412) Variable n(%) n(%) p-Value ATP III Abdominal obesity 227(56.0) 308(74.8) <0.001 Hypertension 143(35.3)156(37.9) 0.448 Diabetes 77(19.0) 107(26.0) 0.017 Hypertriglyceridemia 113(27.9) 83(20.1) 0.009 Low HDL 95(23.5) 121(29.4) 0.055
 Men (n = 405) Women (n=412) Variable n(%) n(%) p-Value ATP III Abdominal obesity 227(56.0) 308(74.8) <0.001 Hypertension 143(35.3)156(37.9) Diabetes 77(19.0) 107(26.0) Hypertriglyceridemia 113(27.9) 83(20.1) Low HDL 95(23.5) 121(29.4) 0.055")
49
Individual metabolic abnormalities among Qatari population according to gender Men (n = 405) Women (n=412) Variable n(%) n(%) p-Value None 88(21.7) 74(18.0) – One 103(25.4) 100(24.3) 0.033 Two 125(30.9) 111(26.9) – Three or more 89(22.0) 127(30.8) – No of components of ATP III
 Women (n=412) Variable n(%) n(%) p-Value None 88(21.7) 74(18.0) – One 103(25.4) 100(24.3) Two 125(30.9) 111(26.9) – Three or more 89(22.0) 127(30.8) – No of components of ATP III")
50
Prevalence of MeS in different Countries Prevalence (%) SampleYearCountry 235422003Arab Americans 2114192001Oman 3611212002Jordan 20.822502004Saudi Arabia 17*1998Palestine 27.68172007Qatar 33.4*16372004Turkey 33.710368?Iran * Crude rates Mussallam et al. Int J Food Safety and PH 2008

51
A Critical Look at the Metabolic Syndrome Is it a Syndrome?* “…too much clinically important information is missing to warrant its designations as a syndrome.” Unclear pathogenesis, Insulin resistance is not a consistent finding in some definitions. CVD risks has not shown to be greater than the sum of it’s individual components. * ADA

52
A Critical Look at the Metabolic Syndrome Research “Until much needed research is completed, clinicians should evaluate and treat all CVD risk factors without regard to whether a patient meets the criteria for diagnosis of the ‘metabolic syndrome’.”

53
A Critical Look at the Metabolic Syndrome Lifestyle The advice remains to treat individual risk factors when present & to prescribe therapeutic lifestyle changes & weight management for obese patients with multiple risk factors.

54
Insulin Resistance: Associated Conditions

57
Determinants and dynamics of the CVD Epidemic in the developing Countries Data from South Asian Immigrant studies Excess, early, and extensive CHD in persons of South Asian origin The excess mortality has not been fully explained by the major conventional risk factors. Diabetes mellitus and impaired glucose tolerance highly prevalent.(Reddy KS, circ 1998). Central obesity, ↑ triglycerides, ↓ HDL with or without glucose intolerance, characterize a phenotype. genetic factors predispose to ↑ lipoprotein(a) levels, the central obesity/glucose intolerance/dyslipidemia complex collectively labeled as the “metabolic syndrome”
. Central obesity, ↑ triglycerides, ↓ HDL with or without glucose intolerance, characterize a phenotype. genetic factors predispose to ↑ lipoprotein(a) levels, the central obesity/glucose intolerance/dyslipidemia complex collectively labeled as the metabolic syndrome .")
58
Determinants and dynamics of the CVD epidemic in the developing countries Other Possible factors Relationship between early life characteristics and susceptibility to NCD in adult hood ( Barker’s hypothesis) (Baker DJP,BMJ,1993) –Low birth weight associated with increased CVD –Poor infant growth and CVD relation Genetic–environment interactions (Enas EA, Clin. Cardiol. 1995; 18: 131–5) -Amplification of expression of risk to some environmental changes esp. South Asian population) -Thrifty gene (e.g. in South Asians)
 -Amplification of expression of risk to some environmental changes esp. South Asian population) -Thrifty gene (e.g. in South Asians).")
59
CVD epidemic in developing & developed countries. Are they same? Urban populations have higher levels of CVD risk factors related to diet and physical activity (overweight, hypertension, dyslipidaemia and diabetes) Tobacco consumption is more widely prevalent in rural population The social gradient will reverse as the epidemics mature. The poor will become progressively vulnerable to the ravages of these diseases and will have little access to the expensive and technology-curative care. The scarce societal resources to the treatment of these disorders dangerously depletes the resources available for the ‘unfinished agenda’ of infectious and nutritional disorders that almost exclusively afflict the poor
 Tobacco consumption is more widely prevalent in rural population The social gradient will reverse as the epidemics mature. The poor will become progressively vulnerable to the ravages of these diseases and will have little access to the expensive and technology-curative care. The scarce societal resources to the treatment of these disorders dangerously depletes the resources available for the ‘unfinished agenda’ of infectious and nutritional disorders that almost exclusively afflict the poor.")
60
Burden of CVD in Pakistan Coronary heart disease Mortality statistics Specific mortality data ideal for making comparisons with other countries are not available Inadequate and inappropriate death certification, and multiple concurrent causes of death

61
Central obesity: a driving force for cardiovascular disease & diabetes “Balzac” by Rodin Front Back

62
Why people physically inactive? Lack of awareness regarding the of physical activity for health fitness and prevention of diseases Social values and traditions regarding physical exercise (women, restriction). Non-availability public places suitable for physical activity (walking and cycling path, gymnasium). Modernization of life that reduce physical activity (sedentary life, TV, Computers, tel, cars).
. Non-availability public places suitable for physical activity (walking and cycling path, gymnasium). Modernization of life that reduce physical activity (sedentary life, TV, Computers, tel, cars)..")
63
Insulin Resistance: Associated Conditions

64
Prevalence of the Metabolic Syndrome Among US Adults NHANES 1988-1994 Prevalence (%) 0 5 10 15 20 25 30 35 40 45 20-2930-3940-4950-5960-69> 70 Men Women Age (years) Ford E et al. JAMA. 2002(287):356. 1999-2002 Prevalence by IDF vs. NCEP Definitions (Ford ES, Diabetes Care 2005; 28: 2745-9) (unadjusted, age 20+) NCEP : 33.7% in men and 35.4% in women IDF: 39.9% in men and 38.1% in women
: Prevalence by IDF vs. NCEP Definitions (Ford ES, Diabetes Care 2005; 28: ) (unadjusted, age 20+) NCEP : 33.7% in men and 35.4% in women IDF: 39.9% in men and 38.1% in women.")
66
Prevention of CVD There is an urgent need to establish appropriate research studies, increase awareness of the CVD burden, and develop preventive strategies. Prevention and treatment strategies that have been proven to be effective in developed countries should be adapted for developing countries. Prevention is the best option as an approach to reduce CVD burden. Do we know enough to prevent this CVD Epidemic in the first place.

67
The new IDF definition focusses on abdominal obesity rather than insulin resistance International Diabetes Federation (IDF) Consensus Definition 2005
 Consensus Definition 2005")
68
Central Obesity Waist circumference – ethnicity specific* – for Europids: Male > 94 cm Female > 80 cm plus any two of the following: Raised triglycerides> 150 mg/dL (1.7 mmol/L) or specific treatment for this lipid abnormality Reduced HDL cholesterol< 40 mg/dL (1.03 mmol/L) in males < 50 mg/dL (1.29 mmol/L) in females or specific treatment for this lipid abnormality Raised blood pressureSystolic : > 130 mmHg or Diastolic: > 85 mmHg or Treatment of previously diagnosed hypertension Raised fasting plasma glucose Fasting plasma glucose > 100 mg/dL (5.6 mmol/L) or Previously diagnosed type 2 diabetes If above 5.6 mmol/L or 100 mg/dL, OGTT is strongly recommended but is not necessary to define presence of the syndrome.
 or specific treatment for this lipid abnormality Reduced HDL cholesterol< 40 mg/dL (1.03 mmol/L) in males < 50 mg/dL (1.29 mmol/L) in females or specific treatment for this lipid abnormality Raised blood pressureSystolic : > 130 mmHg or Diastolic: > 85 mmHg or Treatment of previously diagnosed hypertension Raised fasting plasma glucose Fasting plasma glucose > 100 mg/dL (5.6 mmol/L) or Previously diagnosed type 2 diabetes If above 5.6 mmol/L or 100 mg/dL, OGTT is strongly recommended but is not necessary to define presence of the syndrome.")
69
Treatment of Metabolic Syndrome: 2005 Aspirin Diet, Exercise, Lifestyle change Stop smoking CB1 Receptor Blocker Oral hypoglycaemics Antihypertensives Statins & Fibrates Insulin ACEI &/or A2 receptor blockers

70
Primary management for the Metabolic Syndrome is healthy lifestyle promotion. This includes: moderate calorie restriction (to achieve a 5-10% loss of body weight in the first year) moderate increases in physical activity change dietary composition to reduce saturated fat and total intake, increase fibre and, if appropriate, reduce salt intake. Recommendations for treatment
 moderate increases in physical activity change dietary composition to reduce saturated fat and total intake, increase fibre and, if appropriate, reduce salt intake. Recommendations for treatment.")
71
Appropriate & aggressive therapy is essential for reducing patient risk of cardiovascular disease Lifestyle measures should be the first action Pharmacotherapy should have beneficial effects on –Glucose intolerance/diabetes –Obesity –Hypertension –Dyslipidaemia Ideally, treatment should address all of the components of the syndrome and not the individual components Management of the Metabolic Syndrome

72
Summary: new IDF definition for the Metabolic Syndrome The new IDF definition addresses both clinical and research needs: provides a simple entry point for primary care physicians to diagnose the Metabolic Syndrome providing an accessible, diagnostic tool suitable for worldwide use, taking into account ethnic differences establishing a comprehensive ‘platinum standard’ list of additional criteria that should be included in epidemiological studies and other research into the Metabolic Syndrome

Similar presentations






















![LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]](/19/5810187/big_thumb.jpg "LIFESTYLE MODIFICATIONS FOR PREVENTING HEART DISEASE [e.g. HEART ATTACKS] [ primary prevention of coronary artery disease ] DR S. SAHAI MD [Med.], DM [Card]>")
